м„ң лЎ
мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ(laryngopharyngeal reflux disease, LPRD)мқҖ н•ҳл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ кё°лҠҘ м Җн•ҳлЎң мң„мқҳ лӮҙмҡ©л¬јмқҙ мқёнӣ„л‘җлЎң м—ӯлҘҳн•ҳкұ°лӮҳ, м—ӯлҘҳн•ң мң„мӮ°мқҙ мӢқлҸ„м—җ лЁёл¬ҙлҘҙлҠ” мӢңк°„мқҙ кёём–ҙм§Җкұ°лӮҳ, мң„мӢқлҸ„ м—ӯлҘҳк°Җ мқёнӣ„л‘җлЎң л„ҳм–ҙмҳӨлҠ” кІғмқ„ л§үм•„мЈјлҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ л¶Җм „мңјлЎң мқён•ҙ л°ңмғқн• мҲҳ мһҲлӢӨ[1-4]. мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳмқҳ м№ҳлЈҢлҠ” мӢқмғқнҷң к°ңм„ л“ұмқҳ мғқнҷң мҠөкҙҖ к°ңм„ кіј н•Ёк»ҳ м•Ҫл¬ј м№ҳлЈҢлЎңмҚЁ м ңмӮ°м ң, H2 мҲҳмҡ©мІҙ м°ЁлӢЁм ң, мң„мһҘкҙҖ мҡҙлҸҷ мҙү진м ң, м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ң(proton pump inhibitor, PPI) л“ұмқ„ мӮ¬мҡ©н•ҳлҠ” кІғмқҙ нҡЁкіјм ҒмқҙлӢӨ[5,6].
к·ёлҹ¬лӮҳ мғқнҷң мҠөкҙҖ к°ңм„ л°Ҹ м•Ҫл¬јм—җ лҢҖн•ң м№ҳлЈҢлҘј мһҘкё°к°„ мӢңн–үн•Ём—җлҸ„ л¶Ҳкө¬н•ҳкі нҡЁкіјк°Җ м ңн•ңм Ғмқё нҷҳмһҗм—җм„ң мөңк·ј мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ л¶Җм „мқ„ к°ңм„ мӢңнӮӨлҠ” л°©лІ•мқҙ мӢңлҸ„лҗҳкі мһҲлҠ”лҚ°, к·ё мӨ‘ Reza band(Somna Therapeutics, Germantown, WI, USA)лҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ ліҙмЎ° мһҘм№ҳлЎңм„ң мғҒл¶ҖмӢқлҸ„мқҳ м••л Ҙмқ„ мҰқк°ҖмӢңмјң мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳмқ„ м№ҳлЈҢн•ҳкё° мң„н•ҙ кі м•Ҳлҗң мһҘм№ҳмқҙлӢӨ. Reza bandлЎң м№ҳлЈҢн•ҳмҳҖмқ„ л•Ң мқёнӣ„л‘җ м—ӯлҘҳмҰқмқҙ к°ңм„ лҗҳм—ҲлӢӨлҠ” лӘҮлӘҮмқҳ ліҙкі к°Җ н•ҙмҷём—җм„ңлҠ” мһҲмңјлӮҳ[7,8], н•ңкөӯм—җм„ңлҠ” м•„м§Ғ Reza bandмқҳ м№ҳлЈҢ кІҪн—ҳмқҙ м—ҶлӢӨ. мқҙм—җ м Җмһҗл“ӨмқҖ ліё м—°кө¬м—җм„ң н•ңкөӯмқё мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ нҷҳмһҗм—җм„ң Reza band мӮ¬мҡ© кІҪн—ҳмқ„ нҶ лҢҖлЎң м•Ҳм „м„ұ л°Ҹ нҡЁкіјлҘј нҷ•мқён•ҳкі мһҗ н•ҳмҳҖлӢӨ.
лҢҖмғҒ л°Ҹ л°©лІ•
ліё м—°кө¬м—җм„ңлҠ” мқёнӣ„л‘җ м—ӯлҘҳ мҰқмғҒмңјлЎң м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ң м№ҳлЈҢлҘј мөңмҶҢ 6к°ңмӣ” мқҙмғҒ м§ҖмҶҚн•Ём—җлҸ„ л¶Ҳкө¬н•ҳкі мқёнӣ„л‘җ м—ӯлҘҳ мҰқмғҒмқҙ м§ҖмҶҚлҗҳлҠ” нҷҳмһҗ мӨ‘ Reza band м№ҳлЈҢ м—°кө¬м—җ лҸҷмқҳн•ң 16лӘ…мқҳ мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ мқҳмӢ¬ нҷҳмһҗлҘј лҢҖмғҒмңјлЎң н•ҳмҳҖмңјл©°, 2017л…„ 1мӣ”л¶Җн„° м „н–Ҙм ҒмңјлЎң м—°кө¬лҘј мӢңн–үлҗҳм—ҲлӢӨ. ліё м—°кө¬лҠ” н•ңм–‘лҢҖн•ҷкөҗлі‘мӣҗ мһ„мғҒмӢңн—ҳ мӢ¬мӮ¬мң„мӣҗнҡҢ(Institutional Review Board)мқҳ мҠ№мқёмқ„ л°ӣм•ҳмңјл©° м Җмһҗл“Өкіј Reza bandмҷҖлҠ” мғҒ충лҗҳлҠ” мқҙн•ҙкҙҖкі„к°Җ м—Ҷм—ҲлӢӨ(IRB No. HYUH 2017-03-004-003).
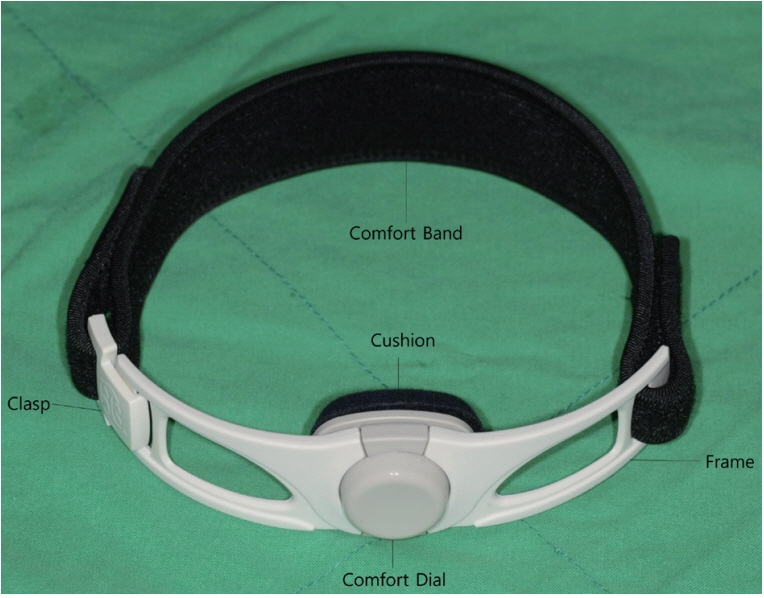
Reza bandлҠ” мңӨмғҒ м—°кіЁ л¶Җмң„ н”јл¶Җ мң„м—җ м°©мҡ©н•ҳм—¬ мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј мң„м—җ м••л Ҙмқ„ к°Җн•ҳлҠ” мһҘм№ҳмқҙлӢӨ. мңӨмғҒ м—°кіЁ л¶Җмң„ н”јл¶Җм—җ лӢҝлҠ” л¶Җмң„лҠ” мҝ м…ҳмңјлЎң мқҙлЈЁм–ҙм ё мһҲм–ҙ н”јл¶Җ мһҗк·№мқ„ мӨ„мқҙкі мҷёл¶Җ н”„л Ҳмһ„мқҙ мҝ м…ҳмқҙ м§ҖмҶҚм Ғмқё м••л Ҙмқ„ к°Җн• мҲҳ мһҲлҸ„лЎқ л°ӣміҗмӨҖлӢӨ. лҳҗ мһҗм„қмңјлЎң лҗҳм–ҙ мһҲлҠ” нҒҙлһ©мқҙ мһҲм–ҙ м°©мҡ©мқҙ мҡ©мқҙн•ҳлҸ„лЎқ м„Өкі„лҗҳм–ҙ мһҲмңјл©°, к°ҖмҡҙлҚ° мһҲлҠ” мЎ°м Ҳ мһҘм№ҳлЎң к°ңмқёмқҙ м••л Ҙмқ„ мЎ°м Ҳн• мҲҳ мһҲлӢӨ(Fig. 1). мҷёлһҳм—җм„ң Reza band м°©мҡ© л°Ҹ мӮ¬мҡ©м—җ лҢҖн•ң көҗмңЎмқ„ мӢңн–үн•ҳмҳҖлҠ”лҚ°, Reza bandк°Җ мңӨмғҒ м—°кіЁ л¶Җмң„ мң„лҘј лҲ„лҘј мҲҳ мһҲлҸ„лЎқ м°©мҡ©н•ҳкІҢ н•ҳмҳҖмңјл©°(Fig. 2), м••л ҘмқҖ лҢҖк°ң 20 mm Hg мқҙмғҒмңјлЎң мӢңмһ‘н•ҳм—¬ м••л Ҙ мЎ°м Ҳ мһҘм№ҳлЎң м°©мҡ© мӢң нҒ° л¶ҲнҺён•Ёмқҙ м—ҶлҠ” м••л ҘмңјлЎң мһҗк°Җ мЎ°м Ҳн•ҳлқј н•ҳмҳҖлӢӨ(Fig. 3). мЈјлЎң мҲҳл©ҙ мӢңм—җ м°©мҡ©н•ҳлҸ„лЎқ н•ҳмҳҖмңјлӮҳ нҷҳмһҗк°Җ к°ҖлҠҘн•ҳл©ҙ лӮ®м—җ нҷңлҸҷ мӨ‘м—җлҸ„ м°©мҡ©н•ҳлҸ„лЎқ к¶Ңкі н•ҳмҳҖлӢӨ.
к°җм—јм„ұ мқёл‘җм—јмқҙлӮҳ нӣ„л‘җм—јмқҙ мһҲкұ°лӮҳ, мһ„мӮ°л¶Җ лҳҗлҠ” лӘЁмң мҲҳмң мӨ‘мқё кІҪмҡ°, нҸҗмҮ„м„ұ л¬ҙнҳёнқЎмқҙ лҸҷл°ҳлҗң кІҪмҡ°, к°‘мғҒм„ лҳҗлҠ” нӣ„л‘җ мў…м–‘мқҙ мһҲлҠ” кІҪмҡ° л°Ҹ кё°нғҖ м—°кө¬м—җ мҳҒн–Ҙмқ„ лҜём№ мҲҳ мһҲлҠ” кё°мҷ•л Ҙмқ„ м§ҖлӢҢ нҷҳмһҗлҠ” м—°кө¬м—җм„ң м ңмҷён•ҳмҳҖлӢӨ.
ліё м—°кө¬м—җм„ң лӘ©н‘ң м№ҳлЈҢ кё°к°„ л°Ҹ 추м Ғ кҙҖм°° кё°к°„мқҖ 12мЈјлЎң Reza bandлҘј мІҳл°©н•ҳкі м°©мҡ© м „кіј м°©мҡ© нӣ„ 2, 4, 8, 12мЈјм—җ кұёміҗ мҷёлһҳлЎң л°©л¬ён•ҳм—¬ м—ӯлҘҳ мҰқмғҒ м§ҖмҲҳ(Reflux Symptom Index, RSI)мҷҖ нӣ„л‘җ м—ӯлҘҳ мҶҢкІ¬(Reflux Finding Score, RFS)мқ„ мёЎм •н•ҳкі Reza band м°©мҡ©кіј кҙҖл Ёлҗң н•©лі‘мҰқмқ„ мЎ°мӮ¬н•ҳмҳҖлӢӨ. RSIлҠ” нҷҳмһҗ ліёмқём—җ мқҳн•ҙ мһ‘м„ұлҗң м„Өл¬ём§ҖлЎң нҸүк°Җн•ҳмҳҖкі [9] RFSлҠ” м—°м„ұ нӣ„л‘җкІҪмңјлЎң мҙ¬мҳҒлҗң мҳҒмғҒмқ„ н•ң лӘ…мқҳ мқҳмӮ¬к°Җ мқјкҙ„м ҒмңјлЎң нҸүк°Җн•ҳмҳҖмңјл©°[10] лҳҗн•ң кё°лҸ„ нҸҗмғү, м—°н•ҳ кіӨлһҖ, нҳёнқЎ кіӨлһҖ, мқёнӣ„л‘җ м¶ңнҳҲ, нҶөмҰқ л“ұмқҳ н•©лі‘мҰқ л°Ҹ мһҘм№ҳмқҳ м§ҖмҶҚм Ғ мӮ¬мҡ© м—¬л¶ҖлҘј нҷ•мқён•ҳмҳҖлӢӨ. RSIлҠ” 13м җ, RFSлҠ” 7м җ мқҙмғҒмқј кІҪмҡ° мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ мқҳмӢ¬ нҷҳмһҗлЎң 진лӢЁн•ҳмҳҖмңјл©° 24 hr pH monitoring лҳҗлҠ” 24 hr intraluminal impedance кІҖмӮ¬лҘј мӢңн–үн•ҳм§ҖлҠ” м•Ҡм•ҳлӢӨ[11].
Reza band м№ҳлЈҢ м „нӣ„м—җ RSI л°Ҹ RFSмқҳ ліҖнҷ”лҘј 비лӘЁмҲҳ кІҖм •лІ•мқё Wilcoxon signed-rank testлҘј мқҙмҡ©н•ҳм—¬ 비көҗн•ҳмҳҖмңјл©°, нҶөкі„н•ҷм Ғ мң мқҳ мҲҳмӨҖмқҖ 95% мқҙмғҒ(pпјң0.05)мңјлЎң н•ҳмҳҖлӢӨ.
кІ° кіј
мҙқ 16мҳҲ мӨ‘ 1мҳҲк°Җ лӮЁм„ұ(6.3%), 15мҳҲк°Җ м—¬м„ұ(93.7%)мқҙм—Ҳмңјл©° нҸүк· м—°л №мқҖ 62.6Вұ9.02м„ёмҳҖлӢӨ. лҢҖмғҒ нҷҳмһҗ 16мҳҲ лӘЁл‘җ 비нқЎм—°мһҗмҳҖмңјл©°, мӮ¬нҡҢ нҶөмғҒм Ғ мқҢмЈјл ҘмқҖ 10мҳҲм—җм„ң мһҲм—Ҳмңјл©° 6мҳҲлҠ” мқҢмЈјл Ҙмқҙ м—Ҷм—ҲлӢӨ. Body mass index(BMI)лҘј нҷ•мқён• мҲҳ мһҲм—ҲлҚҳ нҷҳмһҗлҠ” 16мҳҲ мӨ‘ мҙқ 12мҳҲмҳҖмңјл©° нҸүк· BMIлҠ” 24.9Вұ3.24мҳҖлӢӨ. Reza bandлҘј м°©мҡ©н•ҳкё° м „ лӘЁл“ нҷҳмһҗл“ӨмқҖ мқёнӣ„л‘җ м—ӯлҘҳмҰқмңјлЎң PPI м•Ҫл¬јм№ҳлЈҢ лӢЁлҸ…мқҙлӮҳ, PPIмҷҖ мң„мһҘкҙҖ мҡҙлҸҷ мҙү진м ңмқҳ лі‘н•© м•Ҫл¬јм№ҳлЈҢлҘј л°ӣм•ҳмңјл©°, Reza band м°©мҡ© м „ м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ңмқҳ нҸүк· м№ҳлЈҢ кё°к°„мқҖ 12.7Вұ23.8к°ңмӣ”мқҙм—ҲлӢӨ. лҢҖмғҒ нҷҳмһҗл“ӨмқҖ Reza bandмҷҖ PPI м№ҳлЈҢлҘј к°ҷмқҙн•ҳкұ°лӮҳ Reza bandл§Ңмқ„ лӢЁлҸ…мңјлЎң мӮ¬мҡ©н•ҳмҳҖлҠ”лҚ°, Reza bandмҷҖ PPI лі‘н•©м№ҳлЈҢк°Җ 14мҳҲ, Reza bandл§Ңмқ„ лӢЁлҸ… мӮ¬мҡ©н•ң кІҪмҡ°к°Җ 2мҳҲмҳҖлӢӨ.
мҙқ 16лӘ…мқҳ нҷҳмһҗ мӨ‘ Reza band м°©мҡ© нӣ„, 1лӘ…(6.25%)мқҙ 2мЈј л’Ө мҷёлһҳ м •кё° лӮҙмӣҗ мӢң Reza band м°©мҡ© мӢң л¶ҲнҺёк°җл§Ң мһҲкі нҳём „лҗҳлҠ” кІғ к°ҷм§Җ м•ҠлӢӨкі н•ҳм—¬ мһ„мқҳлЎң м°©мҡ©мқ„ мӨ‘м§Җн•ҳмҳҖмңјл©° лӮҳлЁём§Җ 15лӘ…мқҖ м§ҖмҶҚм ҒмңјлЎң Reza bandлҘј мӮ¬мҡ©н•ҳмҳҖлӢӨ. мӨ‘лҸ„ нғҲлқҪн•ң нҷҳмһҗ 1лӘ…мқ„ м ңмҷён•ң 15лӘ… мӨ‘ 12мЈјк№Ңм§Җ лӘЁл‘җ 추м Ғ кҙҖм°°кіј нҸүк°Җк°Җ к°ҖлҠҘн•ҳмҳҖлҚҳ нҷҳмһҗлҠ” 10лӘ…мқҙм—Ҳкі 8мЈј кҙҖм°°н•ң нҷҳмһҗк°Җ 3лӘ…, 4мЈј кҙҖм°°н•ң нҷҳмһҗк°Җ 2лӘ…мқҙм—ҲлӢӨ. Reza band м°©мҡ© нӣ„мқҳ н•©лі‘мҰқмңјлЎңлҠ” м°©мҡ© мӢң к°ҖлІјмҡҙ лӘ©мқ„ мЎ°лҘҙлҠ” л“Ҝн•ң нҶөмҰқмқ„ нҳёмҶҢн•ң 1лӘ… мҷём—җ лӢӨлҘё нҠ№мқҙ н•©лі‘мҰқмқҖ м—Ҷм—ҲлӢӨ.
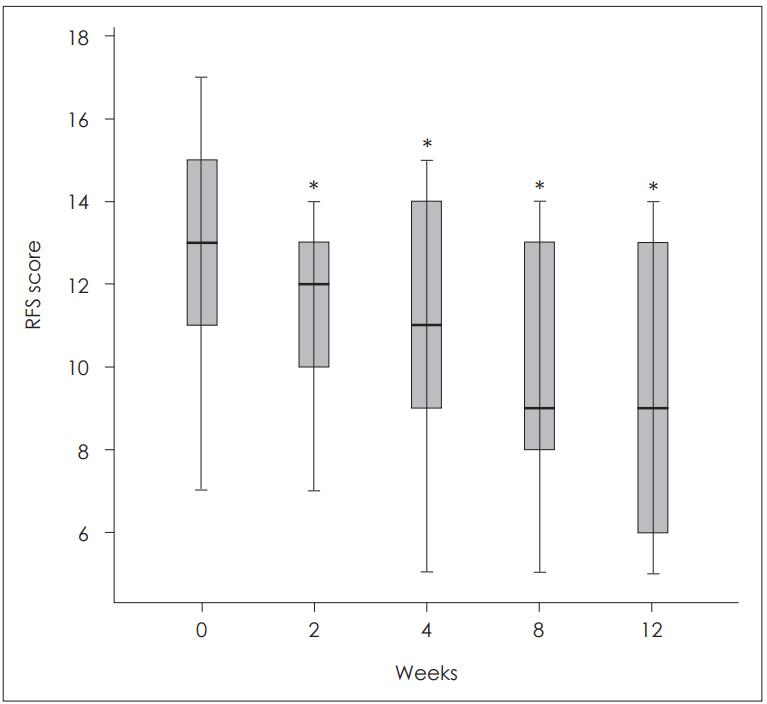
мӨ‘лҸ„ нғҲлқҪн•ң 1лӘ…мқ„ м ңмҷён•ң 15лӘ…м—җм„ң RSIлҠ” м°©мҡ© м „ліҙлӢӨ м°©мҡ© нӣ„ 8мЈј(p=0.005)мҷҖ 12мЈј(p=0.007)м—җ нҶөкі„м ҒмңјлЎң мң мқҳн•ҳкІҢ нҳём „лҗҳм—Ҳмңјл©°(Fig. 4), RFSлҠ” м°©мҡ© м „м—җ 비н•ҙ м°©мҡ© нӣ„ 2мЈј(p=0.011), 4мЈј(p=0.001), 8мЈј(p=0.002), 12мЈј(p=0.005)м—җм„ң лӘЁл‘җ нҶөкі„м ҒмңјлЎң мң мқҳн•ҳкІҢ к°җмҶҢн•ҳмҳҖлӢӨ(Fig. 5).
Reza bandмҷҖ PPIлҘј лҸҷмӢңм—җ мӮ¬мҡ©н•ң кө°(13мҳҲ)кіј Reza bandл§Ңмқ„ мӮ¬мҡ©н•ң кө°(2мҳҲ)мңјлЎң лӮҳлҲ„м–ҙ 분м„қн•ҳмҳҖмқ„ л•ҢлҠ” Reza bandмҷҖ PPI лҸҷмӢң мӮ¬мҡ© кө°м—җм„ңлҠ” нҶөкі„м ҒмңјлЎң мң мқҳн•ҳкІҢ RSI л°Ҹ RFSк°Җ нҳём „лҗҳм—Ҳкі (Table 1), Reza bandл§Ңмқ„ мӮ¬мҡ©н•ң кө°(2мҳҲ)м—җм„ңлҸ„ RSI л°Ҹ RFSк°Җ м°©мҡ© м „ліҙлӢӨ м°©мҡ© нӣ„ нҳём „лҗҳм—ҲмңјлӮҳ нҶөкі„м Ғ нҸүк°ҖлҠ” н• мҲҳ м—Ҷм—ҲлӢӨ.
кі м°°
мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳмқҳ м№ҳлЈҢлҠ” мқҙм „м—җлҠ” мҰқмғҒмқҳ м •лҸ„м—җ л”°лқј лӢЁкі„лі„лЎң мғқнҷңмҠөкҙҖмқҳ к°ңм„ л°Ҹ лӢӨм–‘н•ң м•Ҫл¬јм№ҳлЈҢк°Җ мқҙлЈЁм–ҙмЎҢмңјлӮҳ мөңк·јм—җлҠ” м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ңк°Җ м•Ҫл¬јм№ҳлЈҢмқҳ кё°ліёмқҙлӢӨ[12]. м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ңлҘј 3к°ңмӣ” м •лҸ„ мӮ¬мҡ©н•ҳмҳҖмқ„ л•Ң лҢҖл¶Җ분 нҳём „лҗҳкі л§Ңм•Ҫ м№ҳлЈҢм—җ л°ҳмқ‘мқҙ м—ҶлҠ” кІҪмҡ° мҡ©лҹүмқ„ л‘җ л°°лЎң мҰқлҹүн•ҳкұ°лӮҳ м№ҳлЈҢ кё°к°„мқ„ лҠҳлҰ¬лҠ” кІғмқҙ н‘ңмӨҖм Ғмқё м№ҳлЈҢлЎң м •лҰҪлҗҳм—ҲлӢӨ[5,12-14]. н•ҳм§Җл§Ң к·ёлҹјм—җлҸ„ л¶Ҳкө¬н•ҳкі м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ңлЎң нҳём „лҗҳм§Җ м•ҠлҠ” мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ нҷҳмһҗк°Җ мһҲмңјл©° лҳҗ мһҘкё°к°„мқҳ м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ң м№ҳлЈҢм—җ лҢҖн•ң л¶Ҳм•Ҳк°җ л°Ҹ кұ°л¶Җк°җмқ„ к°–лҠ” кІҪмҡ°лҸ„ мһҲлӢӨ. к·ёлҹ° кІҪмҡ° мҲҳмҲ м Ғ м№ҳлЈҢлҘј кі л Өн• мҲҳлҸ„ мһҲлӢӨ[14].
мғҲлЎңмҡҙ мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳмқҳ м№ҳлЈҢлІ•мңјлЎң мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј ліҙмЎ° мһҘм№ҳ(UES assist device)к°Җ кі м•Ҳлҗҳм–ҙ көӯмҷём—җм„ңлҠ” мқҙлҜё мӮ¬мҡ©лҗҳкі мһҲмңјл©° мқҙм—җ лҢҖн•ң м—°кө¬к°Җ 진н–үлҗҳкі мһҲлӢӨ[7,8,15]. LPRDлҠ” мң„мӢқлҸ„мқҳ м—ӯлҘҳл¬јмқҙ мқёнӣ„л‘җлЎң мҳ¬лқјмҳӨлҠ” кІғмқ„ л°©м§Җн•ҳлҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ м••л Ҙмқҙ л¶Ҳ충분н•ҳм—¬ м•јкё° лҗҳкё° л•Ңл¬ём—җ мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ м••л Ҙмқ„ лҶ’мқҙл©ҙ мқёнӣ„л‘җ м—ӯлҘҳлҘј мӨ„мқј мҲҳ мһҲлӢӨ. El-Rifai л“ұ[16]мқҖ LPR мҰқмғҒмқҙ мһҲлҠ” нҷҳмһҗкө°мқҳ 91%м—җм„ң мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҙ мқҙмҷ„лҗҳм–ҙ мӮ°мқҙ м—ӯлҘҳлҗңлӢӨ ліҙкі н•ҳмҳҖмңјл©° Shaker л“ұ[8]мқҖ мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј ліҙмЎ° мһҘм№ҳлЎң мҷёл¶Җм—җм„ң мңӨмғҒ м—°кіЁм—җ 20~30 mm Hgмқҳ м••л Ҙмқҙ к°Җн•ҳл©ҙ мқёнӣ„л‘җ м—ӯлҘҳлҘј л°©м§Җн• мҲҳ мһҲлҠ” 충분н•ң мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј м••л Ҙмқ„ м–»мқ„ мҲҳ мһҲлӢӨ н•ҳмҳҖлӢӨ. Reza bandлҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј л¶Җмң„лҘј лҲҢлҹ¬ мқёнӣ„л‘җлЎң мң„ лӮҙмҡ©л¬јмқҙ м—ӯлҘҳн•ҳлҠ” кІғмқ„ л§үм•„ LPRDмқҳ мҰқмғҒмқ„ нҳём „мӢңнӮӨл©°, лҢҖк°ң мңӨмғҒ м—°кіЁ мң„ мң„м№ҳм—җ мң„м№ҳмӢңнӮӨкі м Ғм Ҳн•ң м••л Ҙмқ„ к°Җн•ҳл©°, м••л Ҙ мёЎм •кё° л°Ҹ м••л Ҙ мЎ°м Ҳкё°к°Җ л”°лЎң мһҲм–ҙ м Ғм Ҳн•ң м••л Ҙмқ„ мЎ°м Ҳн• мҲҳ мһҲлӢӨ.
мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳмқҳ мҰқмғҒмқ„ мқјмңјнӮӨлҠ” л‘җ к°Җм§Җ кё°м „мқҙ мһҲлҠ”лҚ°, н•ҳлӮҳлҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ м•Ҫнҷ”лЎң мқён•ң м§Ғм ‘м Ғмқё мң„мӮ° м—ӯлҘҳлЎң мқён•ҙ нӣ„л‘җ л°Ҹ мқёл‘җк°Җ мһҗк·№лҗҳкі м—јмҰқмқҙ мқјм–ҙлӮҳл©°, лӢӨлҘё н•ҳлӮҳлҠ” лҜёмЈј мӢ кІҪ л°ҳмӮ¬ мһ‘мҡ©мқҙ кҙҖл ЁлҗңлӢӨ[17]. лҜёмЈј мӢ кІҪ л°ҳмӮ¬ мһ‘мҡ© мқҙлЎ мқҖ л°ңмғқн•ҷм ҒмңјлЎң мӢқлҸ„мҷҖ кё°кҙҖм§Җмқҳ кё°мӣҗмқҙ 비мҠ·н•ҳкі кіөнҶөм ҒмңјлЎң лҜёмЈј мӢ кІҪмқҙ 분нҸ¬н•ҳлҠ”лҚ°, мӮ°мқҳ м—ӯлҘҳк°Җ мқјм–ҙлӮ л•Ң мӣҗмң„ мӢқлҸ„мқҳ мӮ°м„ұнҷ”к°Җ мӮ° лҜјк°җм„ұ мҲҳмҡ©мІҙлҘј мһҗк·№н•ҳм—¬ мӢқлҸ„ л°Ҹ нӣ„л‘җ мһҗмІҙмқҳ мҰқмғҒ л°Ҹ кё°м№Ё л“ұмқҳ нҳёнқЎкё° мҰқмғҒлҸ„ мқјм–ҙлӮңлӢӨлҠ” кІғмқҙлӢӨ[18]. л”°лқјм„ң Reza band к°ҷмқҖ мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј ліҙмЎ° мһҘм№ҳлЎң мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ м••л Ҙмқҙ лҶ’м•„м§Җл©ҙ мӣҗмң„ мӢқлҸ„мқҳ мӮ°м„ұнҷ”к°Җ к°җмҶҢн•ҳм—¬ мҰқмғҒмқҙ нҳём „лҗ мҲҳ мһҲлӢӨ. Slivers л“ұмқҳ м—°кө¬м—җм„ңлҠ” Reza bandлҘј 4мЈјк°„ мҲҳл©ҙ мӢңм—җ м°©мҡ©н•ҳкІҢ н•ҳмҳҖмңјл©° RSIк°Җ Reza band м°©мҡ© нӣ„ 2мЈјл¶Җн„° нҶөкі„м ҒмңјлЎң мң мқҳн•ҳкІҢ 32~61% м •лҸ„ нҳём „лҗҳм—Ҳкі LPRDм—җ мқҳн•ң мҰқмғҒл“Өмқё к°ҖмҠҙ м“°лҰј(78%), мӮјнӮҙ кіӨлһҖ(64%), мӢқнӣ„ кё°м№Ё(63%), мү° лӘ©мҶҢлҰ¬(62%) л“ұлҸ„ нҳём „лҗҳм—ҲлӢӨкі ліҙкі н•ҳмҳҖлӢӨ. л¶Җмһ‘мҡ©мңјлЎңлҠ” лӘ© л”°к°ҖмӣҖ, мү° лӘ©мҶҢлҰ¬, к°ҖлІјмҡҙ н”јл¶Җ л°ң진 л°Ҹ м•Ҫк°„мқҳ лӘ©мЎ°лҰ„ лҠҗлӮҢ м •лҸ„мҳҖмңјл©° мӢ¬к°Ғн•ң л¶Җмһ‘мҡ©мқҙ ліҙкі лҗң л°”лҠ” м—ҶлӢӨ[7,8].
ліё м—°кө¬лҠ” PPI м№ҳлЈҢм—җ 충분н•ң нҡЁкіјк°Җ м—ҶлҠ” мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ мқҳмӢ¬ нҷҳмһҗлҘј лҢҖмғҒмңјлЎң мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳмқҳ лі‘нғң мғқлҰ¬мқҳ к·јліём Ғмқё мӣҗмқёмқҙлқјкі м—¬кІЁм§ҖлҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·јмқҳ м••л Ҙмқ„ лҶ’мқј мҲҳ мһҲлҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј ліҙмЎ° мһҘм№ҳмқё Reza band м Ғмҡ©мқҳ м•Ҳм •м„ұкіј мҳҲ비 нҡЁкіјлҘј нҸүк°Җн•ң көӯлӮҙ мІ« мҳҲ비 м—°кө¬лқјлҠ” лҚ° мқҳмқҳк°Җ мһҲлӢӨ. Reza bandмқҳ мӮ¬мҡ©м—җм„ң к°ҖмһҘ нҒ° мҡ°л ӨлҠ” мҷёл¶Җм—җм„ң м§Ғм ‘м Ғмқё мҷёл Ҙмқҙ к°Җн•ҙм§ҖлҠ” л§ҢнҒј нҶөмҰқ л°Ҹ кІҪл¶Җ м••л°•м—җ мқҳн•ң л¶ҲнҺёк°җм—җ мқҳн•ң мӮ¬мҡ© мӨ‘лӢЁмқҙм—ҲлҠ”лҚ°, 1лӘ…мқ„ м ңмҷён•ң м•Ҫ 94%мқҳ нҷҳмһҗм—җм„ң Reza band м Ғмҡ©мқҙ к°ҖлҠҘн•ҳмҳҖмңјл©°, кё°кө¬мқҳ м••л Ҙ мЎ°м Ҳ мһҘм№ҳлЎң м Ғм Ҳн•ң м••л Ҙм җмқ„ м°ҫм•„лӮҙм–ҙ н•©лі‘мҰқмқ„ мөңмҶҢнҷ”н• мҲҳ мһҲм—ҲлӢӨ. м№ҳлЈҢ нҡЁкіј л©ҙм—җм„ңлҸ„ Reza band мӮ¬мҡ© нӣ„ нҶөкі„м ҒмңјлЎң мң мқҳн•ҳкІҢ RSIмҷҖ RSFк°Җ нҳём „лҗҳм–ҙ м№ҳлЈҢ нҡЁкіјк°Җ мһҲмңјлҰ¬лқј мғқк°ҒлҗҳлӮҳ, л§ҺмқҖ кІҪмҡ°м—җм„ң Reza bandмҷҖ лҸҷмӢңм—җ PPIлҘј к°ҷмқҙ мӮ¬мҡ©н•ҳм—¬ Reza band мһҗмІҙм—җ мқҳн•ң нҡЁкіјл§Ңмқ„ нҸүк°Җн•ҳкё°м—җ м–ҙл Өмҡҙ м җмқҙ мһҲкі Reza bandлҘј мӮ¬мҡ©н•ҳм§Җ м•ҠлҠ” лҢҖмЎ°кө°мқҙ м—ҶлҠ” м—°кө¬лқјлҠ” м ңн•ңм җмқҙ мһҲм–ҙ мқҙлҘј ліҙмҷ„н•ҳкё° мң„н•ң 추к°Җ м—°кө¬к°Җ н•„мҡ”н•ҳлӢӨкі мғқк°ҒлҗңлӢӨ. к·ёлҹ¬лӮҳ мөңмҶҢн•ң ліё м—°кө¬мқҳ кІ°кіјлЎң лҜёлЈЁм–ҙ мқёнӣ„л‘җ м—ӯлҘҳмҰқ нҷҳмһҗм—җм„ң Reza bandмқҳ мӮ¬мҡ©мқҖ мӨ‘мҡ” н•©лі‘мҰқмқҙ м—ҶлҠ” м•Ҳм „н•ң л°©лІ•мқҙлқј мғқк°Ғлҗҳл©°, мҳҲ비 м—°кө¬лЎң л§ҺмқҖ м ңн•ңм җмқҙ мһҲм§Җл§Ң н–Ҙнӣ„ мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј ліҙмЎ° мһҘм№ҳлҘј нҷңмҡ©н•ң м№ҳлЈҢ л°Ҹ м—°кө¬м—җ кё°ліё мһҗлЈҢлҘј м ңкіөн•ҳлҰ¬лқј мғқк°Ғн•ңлӢӨ.
мқҙ м—°кө¬лҠ” мғҒл¶ҖмӢқлҸ„ кҙ„м•Ҫк·ј ліҙмЎ° мһҘм№ҳмқё Reza bandм—җ кҙҖн•ң көӯлӮҙ мІ« мҳҲ비연кө¬лЎң мқёнӣ„л‘җ м—ӯлҘҳ м§Ҳнҷҳ нҷҳмһҗм—җм„ң м•Ҳм „н•ҳкІҢ м Ғмҡ©н• мҲҳ мһҲмңјл©° м–‘м„ұмһҗ нҺҢн”„ м–өм ңм ңмҷҖ лі‘н•©н•ҳм—¬ мӮ¬мҡ©н•ҳкұ°лӮҳ лӢЁлҸ…мңјлЎң м Ғмҡ©н• мҲҳ мһҲмңјлҰ¬лқј мғқк°ҒлҗңлӢӨ.