м„ң лЎ
м•…м„ұнқ‘мғүмў…мқҖ л©ңлқјлӢҢ м„ёнҸ¬к°Җ мһҲлҠ” лӘЁл“ л¶Җмң„м—җ л°ңмғқн• мҲҳ мһҲмңјлӮҳ, лҢҖл¶Җ분 н”јл¶Җм—җм„ң л°ңмғқн•ҳкі 1.3% м •лҸ„л§Ң м җл§үм—җм„ң л°ңмғқн•ңлӢӨ[1,2]. м „мІҙ м•…м„ұнқ‘мғүмў…м—җм„ң м•Ҫ 20%к°Җ л‘җкІҪл¶Җм—җм„ң л°ңмғқн•ҳкі , м җл§үнҳ• нқ‘мғүмў…мқҖ 50% мқҙмғҒмқҙ 비강, 비л¶Җ비лҸҷ л°Ҹ кө¬к°•м—җм„ң л°ңмғқн•ңлӢӨ[2]. кІҪл¶Җмқҳ м „мқҙм„ұ м•…м„ұнқ‘мғүмў…мқҖ л“ңл¬јл©°, нҠ№нһҲ мӣҗл°ңм§Җ л¶ҲлӘ…мқҖ м „мІҙ м•…м„ұ нқ‘мғүмў…мқҳ 2~5% м •лҸ„лЎң л§Өмҡ° л“ңл¬јлӢӨ[3].
71м„ё лӮЁмһҗк°Җ н”јн•ҳ нӣ„кІҪл¶Җ мў…л¬јм—җ лҢҖн•ҙ м Ҳм ңмғқкІҖмқ„ мң„н•ҙм„ң н”јл¶Җкіјм—җм„ң ліёкіјлЎң мқҳлў°лҗҳм–ҙ лҰјн”„м ҲлЎң м „мқҙлҗң мӣҗл°ңм§Җ л¶ҲлӘ…мқҳ м•…м„ұнқ‘мғүмў…мңјлЎң мөңмў… 진лӢЁлҗҳм—ҲлӢӨ. ліё мҰқлЎҖк°Җ нӣ„кІҪл¶Җм—җ л°ңмғқн•ң мӣҗл°ңм§Җ лҜёмғҒмқҳ м „мқҙм„ұ м•…м„ұнқ‘мғүмў…мқҳ көӯлӮҙм—җм„ң мІ« ліҙкі лЎң мӮ¬лЈҢлҗҳм–ҙ л¬ён—Ңкі м°°кіј н•Ёк»ҳ ліҙкі н•ҳкі мһҗ н•ңлӢӨ.
мҰқ лЎҖ
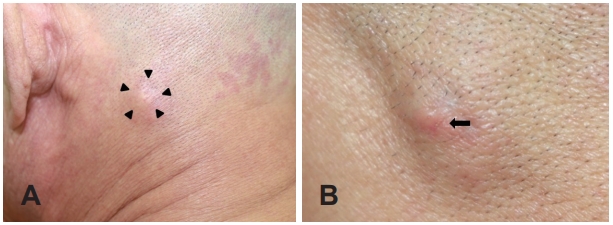
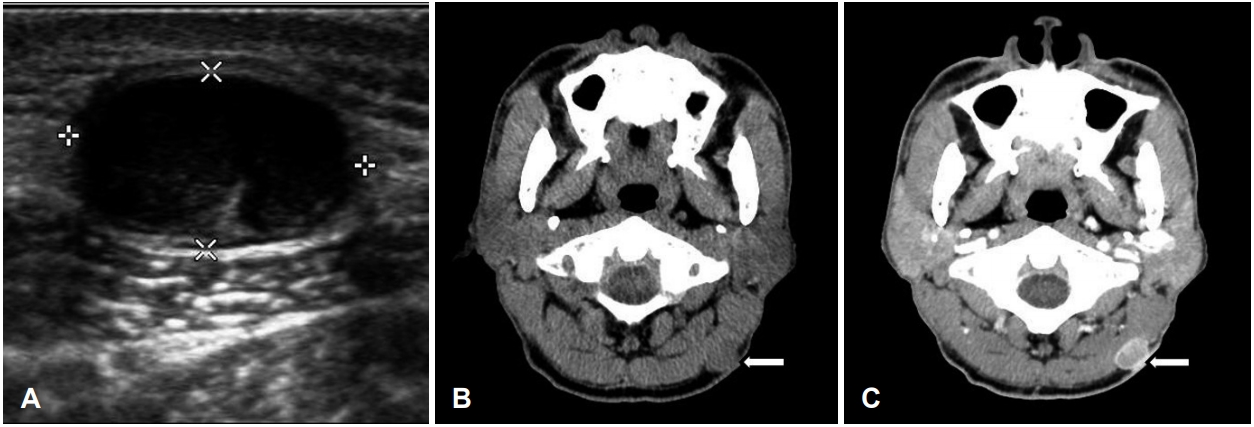
71м„ё лӮЁмһҗ нҷҳмһҗк°Җ лӮҙмӣҗ 5к°ңмӣ” м „л¶Җн„° л°ңмғқн•ң н”јн•ҳ нӣ„кІҪл¶Җ мў…л¬јлЎң н”јл¶Җкіјм—җм„ң мқҳлў°лҗҳм—ҲлӢӨ. кіјкұ°л ҘмғҒ Bнҳ• к°„м—ј ліҙк· мһҗмқҙл©°, нқЎм—° л°Ҹ мқҢмЈјл ҘмқҖ м—Ҷм—ҲлӢӨ. лӢӨлҘё н”јл¶Җм§Ҳнҷҳмқҳ лі‘л ҘмқҖ м—Ҷм—Ҳмңјл©°, к°ҖмЎұл ҘмғҒ нҠ№мқҙмӮ¬н•ӯмқҖ м—Ҷм—ҲлӢӨ. мў…л¬јмқҖ 3к°ңмӣ” м „л¶Җн„° нҒ¬кё°к°Җ м җм°Ё мҰқк°Җн•ҳмҳҖкі нҶөмҰқмқҙ лҸҷл°ҳлҗҳм—Ҳмңјл©°, м§Ғм „ н”јл¶Җкіјм—җм„ң мӢңн–үн•ң нҺҖм№ҳмғқкІҖм—җм„ нҠ№мқҙ мҶҢкІ¬ м—Ҷм—ҲлӢӨ. мӢ мІҙ кІҖмӮ¬м—җм„ң мўҢмёЎ нӣ„кІҪл¶Җ н”јн•ҳмёөм—җ м•Ҫ 2Г—2 cm нҒ¬кё°мқҳ м••нҶөмқ„ лҸҷл°ҳн•ҳл©° 비көҗм Ғ лӢЁлӢЁн•ҳкі н”јл¶Җ н‘ңл©ҙм—җ нҷҚл°ҳм„ұ кө¬м§„мқҙ лҸҷл°ҳлҗң кі м •м„ұ мў…л¬јмқҙ мҙү진лҗҳм—ҲлӢӨ(Fig. 1). кІҪл¶Җмқҳ лӢӨлҘё л¶Җмң„м—җ л№„м •мғҒм ҒмңјлЎң мҙүм§ҖлҗҳлҠ” мў…л¬јмқҖ м—Ҷм—Ҳкі , мқёнӣ„л‘җ лӮҙмӢңкІҪ мҶҢкІ¬м—җм„ң нҠ№мқҙ мҶҢкІ¬мқҖ м—Ҷм—ҲлӢӨ. м „мӢ мғҒнғңлҘј нҸүк°Җн•ҳлҠ” ECOG(Eastern Cooperative Oncology Group) нҷңлҸҷлҸ„лҠ” 0м җмқҙм—Ҳмңјл©°, л°ңм—ҙ л°Ҹ мІҙмӨ‘ к°җмҶҢ л“ұмқҳ м „мӢ мҰқмғҒлҸ„ м—Ҷм—ҲлӢӨ. мҳҒмғҒн•ҷм Ғ нҸүк°ҖлҘј мң„н•ҳм—¬ мӢңн–үн•ң мҙҲмқҢнҢҢ кІҖмӮ¬м—җм„ң мўҢмёЎ нӣ„кІҪл¶Җм—җ 1.9Г—1.4 cm нҒ¬кё°мқҳ кІҪкі„к°Җ 분лӘ…н•ҳкі лӮҙл¶Җм—җ нҳҲлҘҳ нқҗлҰ„мқҙ мһҲлҠ” м Җм—җмҪ” мқҢмҳҒмқҳ к· м§Ҳн•ң мў…л¬јмқҙ кҙҖм°°лҗҳм—Ҳкі (Fig. 2A), кІҪл¶Җ м „мӮ°нҷ” лӢЁмёө мҙ¬мҳҒм—җм„ңлҠ” мўҢмёЎ нӣ„кІҪл¶Җм—җ 2.1Г—1.4 cm нҒ¬кё°мқҳ кІҪкі„к°Җ лӘ…нҷ•н•ҳкі мЈјліҖл¶ҖлҠ” мЎ°мҳҒ мҰқк°•лҗҳл©° мӨ‘мӢ¬л¶Җк°Җ м Җл°ҖлҸ„ мҶҢкІ¬мқ„ ліҙмқҙлҠ” н”јн•ҳ мў…л¬јмқҙ кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 2B and C).
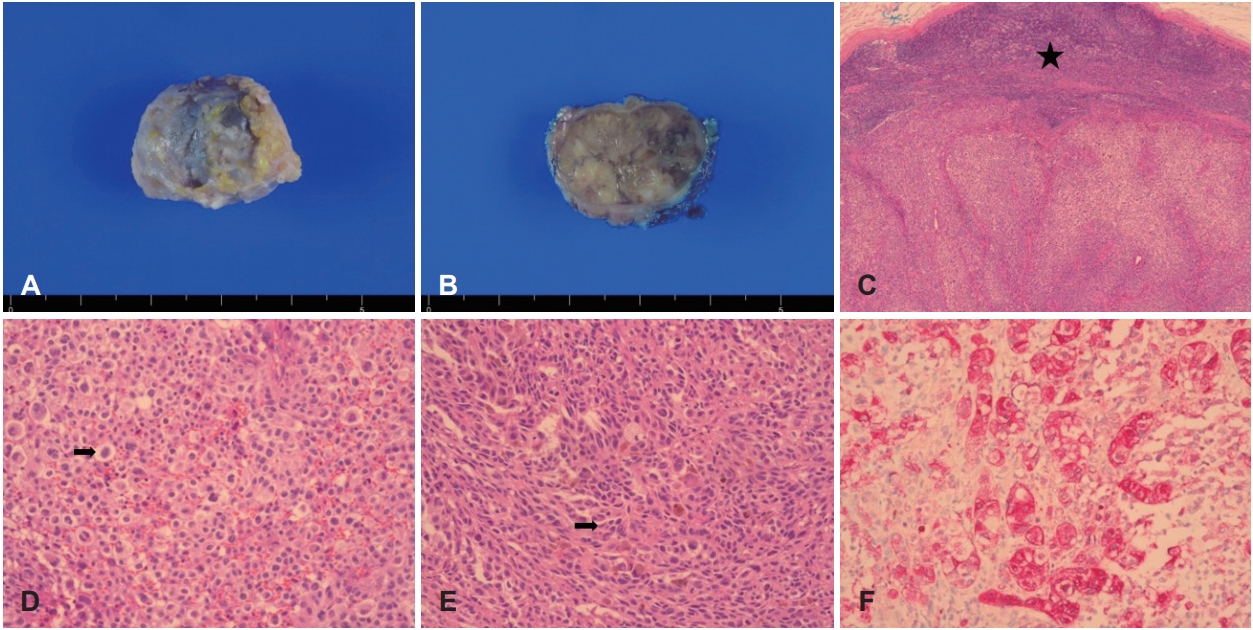
нӣ„кІҪл¶Җм—җ л°ңмғқн•ң н‘ңн”јлӮӯмў…, м§Җл°©мў…, 섬мң мў…, лӘЁкё°м§Ҳмў… л°Ҹ м•…м„ұ мў…м–‘ л“ұмқҳ к°ҖлҠҘм„ұмқ„ м—јл‘җм—җ л‘җкі м Ҳм ңмғқкІҖмқ„ мӢңн–үн•ҳмҳҖлӢӨ. мў…л¬јкіј к°ҖмһҘ мң м°©мқҙ мӢ¬н•ң л¶Җмң„м—җм„ң 5 mm м •лҸ„ мң„мҷҖ м•„лһҳлЎң нғҖмӣҗнҳ• лӘЁм–‘мңјлЎң н”јл¶ҖлҘј м Ҳк°ңн•ҳмҳҖлӢӨ. мў…л¬јмқҖ мЈјліҖл¶ҖмҷҖ мң м°©мқҙ мһҲм—Ҳмңјл©°, н•ҳл°©мқҳ к·јмңЎмёөкіј л°•лҰ¬н•ң нӣ„ мң м°©мқҙ мӢ¬н•ң н”јл¶ҖлҘј нҸ¬н•Ён•ҳм—¬ м ңкұ° н•ҳмҳҖмңјл©°, мӨ‘л“ұлҸ„мқҳ м¶ңнҳҲмқҙ мһҲм—ҲлӢӨ. лі‘лҰ¬ мңЎм•Ҳ мҶҢкІ¬м—җм„ң мў…л¬јмқҳ кІҪкі„лҠ” 분лӘ…н•ҳкі м ҲлӢЁл©ҙмқҖ л№„к· м§Ҳн•ң м–‘мғҒмқҙм—ҲлӢӨ(Fig. 3A and B). нҳ„лҜёкІҪ мҶҢкІ¬м—җм„ңлҠ” 진피 лӮҙ мң мғҒн”јм„ёнҸ¬мҷҖ 방추세нҸ¬к°Җ лӢӨмҲҳ кҙҖм°°лҗҳм—Ҳкі (Fig. 3C-E), л©ҙм—ӯ мЎ°м§Ғнҷ”н•ҷ м—јмғүм—җм„ң HMB-45, Melan A, S-100м—җ м–‘м„ұмқ„ ліҙм—¬(Fig. 3F) мөңмў…м ҒмңјлЎң лҰјн”„м Ҳм—җ м „мқҙлҗң м „мқҙм„ұ м•…м„ұнқ‘мғүмў…мңјлЎң 진лӢЁлҗҳм—ҲлӢӨ. мӣҗл°ңм§ҖлҘј м°ҫкё° мң„н•ҙ лҰјн”„м•Ўмқҳ л°°м•Ў кІҪлЎңлҘј кі л Өн•ҳм—¬ нӣ„л‘җл¶Җ м „мІҙмқҳ н”јл¶ҖлҘј мӢң진 л°Ҹ мҙү진н•ҳмҳҖм§Җл§Ң нҠ№мқҙм җмқҖ м—Ҷм—Ҳкі , нқүл¶Җ, ліөл¶Җ м „мӮ°нҷ” лӢЁмёө мҙ¬мҳҒ л°Ҹ м–‘м „мһҗлӢЁмёөмҙ¬мҳҒмҲ л“ұмқ„ мӢңн–үн•ҳмҳҖмңјлӮҳ, м—ӯмӢң нҠ№мқҙ мҶҢкІ¬ м—Ҷм—ҲлӢӨ. мқҙмғҒмқҳ мҶҢкІ¬л“Өмқ„ мў…н•©н•ҳм—¬ лҰјн”„м ҲлЎң м „мқҙлҗң мӣҗл°ңм§Җ л¶ҲлӘ…мқҳ м•…м„ұ лҰјн”„мў…мңјлЎң мөңмў… 진лӢЁлҗҳм—Ҳмңјл©°, лі‘кё°лҠ” Stage lVлЎң нҸүк°Җлҗҳм—ҲлӢӨ. к·јм№ҳ мҲҳмҲ мқ„ мң„н•ҙ нӣ„мҷёмёЎ кІҪл¶Җм Ҳм ңмҲ (posterolateral neck dissection)мқ„ к¶Ңмң н•ҳмҳҖмңјлӮҳ, нҷҳмһҗ분мқҙ к°•н•ҳкІҢ кұ°л¶Җн•ҳм—¬ нҳҲм•Ўмў…м–‘лӮҙкіјлЎң мқҳлў°н•ҳм—¬ н‘ңм Ғм№ҳлЈҢм ңмқё Nivolumab(Opdivoв“Ү, Ono Pharma, Osaka, Japan)мңјлЎң м№ҳлЈҢлҘј н•ҳмҳҖкі , 6к°ңмӣ”мқҙ м§ҖлӮң нҳ„мһ¬к№Ңм§Җ мһ¬л°ң мҶҢкІ¬ м—Ҷмқҙ кІҪкіјкҙҖм°° мӨ‘мқҙлӢӨ.
кі м°°
м•…м„ұнқ‘мғүмў…мқҖ м•„мӢңм•„ліҙлӢӨлҠ” л°ұмқём—җм„ң нқ”н•ҳкі , нғңм–‘кҙ‘ л…ём¶ңмқҙ л°ңлі‘ мң„н—ҳм„ұмқ„ лҶ’мқј мҲҳ мһҲм–ҙ л‘җкІҪл¶Җм—җм„ңлҠ” м•Ҳл©ҙл¶Җм—җм„ң нҳёл°ңн•ңлӢӨ[1,4,5]. лҢҖл¶Җ분 н”јл¶Җм—җм„ң л°ңмғқн•ҳм§Җл§Ң м•Ҫ 0.8~1.3%лҠ” м җл§үм—җм„ң л°ңмғқн•ҳл©°, нӣ„мһҗлҠ” м„ёнҸ¬л¶„м—ҙмқҳ л№ҲлҸ„к°Җ лҶ’кі нҳҲкҙҖмқҙлӮҳ лҰјн”„м Ҳ м№ЁмңӨмқҙ нқ”н•ҳм—¬ кі м•…м„ұлҸ„лЎң мҳҲнӣ„к°Җ л¶Ҳлҹүн•ҳлӢӨ[2,6]. м•…м„ұнқ‘мғүмў…мқҖ мһ¬л°ңкіј м „мқҙк°Җ нқ”н•ҳл©°, нҳҲн–үм„ұліҙлӢӨ лҰјн”„м Ҳмқ„ нҶөн•ң м „мқҙк°Җ лЁјм Җ л°ңмғқн•ңлӢӨ[7]. м „мқҙмқҳ нҳ•нғңлЎңлҠ” мӣҗл°ң нқ‘мғүмў…м—җм„ң 5 cm мқҙлӮҙм—җ л°ңмғқн•ҳлҠ” мң„м„ұм „мқҙ(satellite metastasis)мҷҖ мӣҗл°ңм§Җм—җм„ң 5 cm мқҙмғҒ л–Ём–ҙ진 кіім—җм„ңл¶Җн„° көӯмҶҢлҰјн”„м Ҳ мӮ¬мқҙм—җм„ң м „мқҙк°Җ мқјм–ҙлӮҳлҠ” нҶөкіјм „мқҙ(in-transit metastasis), көӯмҶҢ лҰјн”„м Ҳ м „мқҙ л°Ҹ мӣҗкІ©м „мқҙ л“ұмңјлЎң лӮҳлҲҢ мҲҳ мһҲлӢӨ[7]. 192лӘ…мқ„ лҢҖмғҒмңјлЎң н•ң ліҙкі м—җм„ң м „мқҙл¶Җмң„лҠ” н•ҳм§Җк°Җ к°ҖмһҘ л§Һм•ҳкі л‘җн”ј, нҢ”, м•Ҳл©ҙ л“ұмқҳ мҲңмңјлЎң л°ңмғқн•ҳмҳҖкі , кІҪл¶ҖлҠ” л“ңл¬јм—ҲлӢӨ[3]. мӣҗл°ңм§ҖлҘј м•Ң мҲҳ м—ҶлҠ” м „мқҙм„ұ м•…м„ұнқ‘мғқмў…мқҖ м „мІҙ м•…м„ұнқ‘мғүмў…мқҳ м•Ҫ 2~5%лҘј м°Ём§Җн•ҳл©° көӯлӮҙм—җм„ңлҠ” мёЎкІҪл¶Җм—җ л°ңмғқн•ң 2мҳҲл§Ң ліҙкі лҗҳм—Ҳкі [8,9], ліё мҰқлЎҖмІҳлҹј нӣ„кІҪл¶Җм—җм„ң л°ңмғқн•ң көӯлӮҙ ліҙкі лҠ” м—Ҷм—ҲлҚҳ кІғмңјлЎң мӮ¬лЈҢлҗңлӢӨ.
лҰјн”„м Ҳ м „мқҙлҠ” мӣҗл°ңм§Җм—җ л”°лқјм„ң лӢӨм–‘н•ҳл©°, л‘җкІҪл¶Җм—җм„ңлҠ” мЈјлЎң мқҙн•ҳм„ кіј кІҪл¶Җ в…Ўкө¬м—ӯмқҙ нқ”н•ң м „мқҙл¶Җмң„мқҙл©°[5,10], Vкө¬м—ӯ л°Ҹ нӣ„л‘җл¶Җ лҰјн”„м ҲмқҖ нӣ„л‘җл¶Җ л‘җн”јм—җм„ң м „мқҙлҗҳлҠ” кІҪмҡ°к°Җ нқ”н•ҳлӢӨ[5]. м•…м„ұнқ‘мғүмў…мқҳ мӣҗкІ© м „мқҙлҠ” к°„, лҮҢ, нҸҗ л°Ҹ кіЁ л“ұм—җ нқ”н•ҳлӢӨ[9]. мӣҗл°ңм§Җ л¶ҲлӘ…мқё кІҪмҡ°мқҳ мӣҗмқёмңјлЎңлҠ” мқём ‘ лҰјн”„м Ҳ м „мқҙ нӣ„ мӣҗл°ңлі‘мҶҢмқҳ мһҗм—° мҶҢл©ё, мӣҗл°ңлі‘мҶҢлҘј л°ңкІ¬н•ҳм§Җ лӘ»н•ң кІҪмҡ° л°Ҹ лҰјн”„м Ҳ лӮҙ л№„м •мғҒм Ғмқё м—јмғүм„ёнҸ¬мқҳ м•…м„ұ ліҖнҷ” л“ұмқҳ к°Җм„Өмқҙ мһҲлӢӨ[9]. лі‘лҰ¬мЎ°м§Ғн•ҷм ҒмңјлЎң м „мқҙм„ұ м•…м„ұнқ‘мғүмў…мқҖ л№„м •нҳ• л©ңлқјлӢҢм„ёнҸ¬к°Җ н‘ңн”јмқҳ м№ЁлІ” м—Ҷмқҙ 진피мҷҖ н”јн•ҳм§Җл°©мёөм—җ мЎҙмһ¬н•ҳл©°, мў…м–‘ лӮҙ л©ңлқјлӢҢмғүмҶҢлҘј нҷ•мқён•ҳл©ҙ 진лӢЁлҗҳм§Җл§Ң л¬ҙл©ңлқјлӢҢ м„ұ нқ‘мғүмў…мқҖ S-100, HMB-45 л“ұмқҳ л©ҙм—ӯм—јмғүмқ„ нҶөн•ҙм„ң 진лӢЁн• мҲҳ мһҲлӢӨ[7,9].
м•…м„ұнқ‘мғүмў…мқҙ мӣҗл°ң лҳҗлҠ” м „мқҙм„ұ лі‘ліҖ мқём§ҖлҘј кө¬л¶„н•ҳлҠ” кІғмқҖ мҳҲнӣ„ л°Ҹ м№ҳлЈҢ л°©лІ•мқҙ лӢӨлҘҙкё° л•Ңл¬ём—җ мӨ‘мҡ”н•ҳлӢӨ[6]. мЎ°кё° л°ңкІ¬ мӢңм—җлҠ” кҙ‘лІ”мң„ м Ҳм ңм—°мқ„ л‘җкі м Ҳм ңмҲ мқ„ мӢңн–үн•ҳлҠ” кІғмқҙ м№ҳлЈҢмӣҗм№ҷмқҙм§Җл§Ң, лі‘ліҖмқҳ мң„м№ҳ, лІ”мң„ л°Ҹ м „мқҙ м—¬л¶Җ л“ұм—җ л”°лқјм„ң мҲҳмҲ мқҙ м–ҙл Өмҡё мҲҳ мһҲлӢӨ[6]. мҲҳмҲ мқҙ л¶Ҳк°ҖлҠҘн•ҳкұ°лӮҳ, мһ¬л°ң лҳҗлҠ” мӣҗкІ© м „мқҙмқҳ кІҪмҡ° н•ӯм•”нҷ”н•ҷмҡ”лІ•мңјлЎң м„ёнҸ¬лҸ…м„ұ н•ӯм•”м ңмқё dacarbazineлҘј лӢЁлҸ… нҳ№мқҖ vincristine, CCNU[1-(2-chloroethyl)-3-cyclohexyl-1-nitrosourea], dactinomycin, belomycin л“ұкіј лі‘н•©н•ҳм—¬ мӮ¬мҡ©н•ҳкұ°лӮҳ[2], interleukin-2 л“ұмқ„ мқҙмҡ©н•ң л©ҙм—ӯм№ҳлЈҢмҡ”лІ•мқҙ к°ҖлҠҘн•ҳлӮҳ м№ҳлЈҢ л°ҳмқ‘лҘ мқҙ лӮ®кі мӢ¬к°Ғн•ң лҸ…м„ұмңјлЎң м ңн•ңмқҙ мһҲлӢӨ[1]. мөңк·јм—җлҠ” нқ‘мғүмў…мқҳ л°ңмғқ л°Ҹ 진н–үм—җ кҙҖм—¬н•ҳлҠ” B-Raf proto-oncogene(BRAF), neuroblastoma RAS viral oncogene homolog(NRAS), mast/stem cell growth factor receptor Kit(C-KIT)мҷҖ кҙҖкі„лҗҳлҠ” 분мһҗкё°м „кіј л©ҙм—ӯм„ёнҸ¬мқҳ мў…м–‘м„ёнҸ¬м—җ лҢҖн•ң л©ҙм—ӯнҡҢн”ј(immune escape)м—җ кҙҖм—¬н•ҳлҠ” cytotoxic T lymphocyte-associated antigen 4(CTLA-4), programmed death receptor-1(PD-1), programmed deathligand 1(PD-L1)мқ„ н‘ңм ҒмңјлЎң н•ҳлҠ” лӢӨм–‘н•ң н‘ңм Ғм№ҳлЈҢм ңлҘј мқҙмҡ©н•ң м№ҳлЈҢлҘј н•ҳкі мһҲлӢӨ[1]. н‘ңм Ғм№ҳлЈҢм ңлҠ” кё°мЎҙмқҳ н•ӯм•”м№ҳлЈҢмҡ”лІ•кіј 비көҗн•ҳм—¬ мң мқҳн•ҳкІҢ мғқмЎҙмңЁмқ„ н–ҘмғҒмӢңнӮЁлӢӨкі ліҙкі лҗҳм—ҲлӢӨ[1]. ліё мҰқлЎҖм—җм„ң мӮ¬мҡ©лҗң н‘ңм Ғм№ҳлЈҢм ңмқё Nivoluamb(Opdivoв“Ү)лҠ” Tм„ёнҸ¬ мҰқмӢқкіј нҷңм„ұнҷ”лҘј м–өм ңн•ҳлҠ” PD-1м—җ лҢҖн•ң н•ӯмІҙлЎң Tм„ёнҸ¬лҘј нҷңм„ұнҷ”мӢңмјң л©ҙм—ӯкі„к°Җ м•”мқ„ м ңкұ°н• мҲҳ мһҲкІҢ н•ҙмЈјлҠ” кё°м „мқҳ м•Ҫл¬јмқҙлӢӨ[11].
м Җмһҗл“ӨмқҖ ліё мҰқлЎҖлҘј нҶөн•ҙ лҜём„ён•ң н”јл¶ҖліҖнҷ”лҘј лҸҷл°ҳн•ҳлҠ” н‘ңмёө кІҪл¶Җ мў…л¬јмқҳ кІҪмҡ° к°җ별진лӢЁм—җ м•…м„ұнқ‘мғүмў…м—җ мқҳн•ң лҰјн”„м ҲлЎңмқҳ м „мқҙм„ұ лі‘ліҖмқ„ м—јл‘җм—җ л‘җм–ҙм•ј н•ҳкі , мӢ мҶҚн•ң мЎ°м§Ғн•ҷм Ғ нҷ•м§„мқ„ нҶөн•ҙ мЎ°кё°м—җ м№ҳлЈҢлҘј мӢңмһ‘н•ҳлҠ” кІғмқҙ мҳҲнӣ„м—җ мӨ‘мҡ”н•ҳлӢӨлҠ” көҗнӣҲмқ„ м–»м—ҲлӢӨ.