ņä£ ļĪĀ
ļ¬©ĻĘĀņ”Ø(mucormycosis)ņØĆ ņØĖĻ░äņŚÉĻ▓ī ļ░£ņāØĒĢśļŖö ņ¦äĻĘĀ Ļ░ÉņŚ╝ ņżæ Ļ░Ćņן ņ╣śļ¬ģņĀüņØ┤ļ®░ ļ╣ĀļźĖ ņåŹļÅäļĪ£ ņ¦äĒ¢ēļÉśļŖö ņ¦łĒÖśņ£╝ļĪ£ ļ╣äļćīļ¬©ĻĘĀņ”Ø(rhinocerebral mucormycosis)ņØ┤ Ļ░Ćņן ĒØöĒĢ£ ĒśĢĒā£ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[1,2]. ņŻ╝ļĪ£ ņĪ░ņĀłļÉśņ¦Ć ņĢŖļŖö ļŗ╣ļć©, ļīĆņé¼ņןņĢĀ, ņןĻĖ░ņØ┤ņŗØ ĒÖśņ×É, ņŖżĒģīļĪ£ņØ┤ļō£ļź╝ ņןĻĖ░Ļ░ä ņé¼ņÜ®ĒĢ£ ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖś ĒÖśņ×ÉņŚÉĻ▓īņä£ ĻĖ░ĒÜīĻ░ÉņŚ╝ņ£╝ļĪ£ ļ░£ņāØĒĢśļ®░ ĻĄŁļé┤ņŚÉļŖö 1980ļģäļīĆ ņØ┤Ēøä ņ×ÉĻ░Ćļ®┤ņŚŁņ¦łĒÖś ļ░Å ņןĻĖ░ņØ┤ņŗØ ĒÖśņ×ÉĻ░Ć ļŖśņ¢┤ļéśĻ▓ī ļÉśļ®┤ņä£ ņןĻĖ░Ļ░ä ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ ļ░Å ņŖżĒģīļĪ£ņØ┤ļō£ ņé¼ņÜ® ņ”ØĻ░ĆļĪ£ ļ░£ņāØļźĀņØ┤ ņĀÉņ░© ļŖśņ¢┤ļéśļŖö ņČöņäĖņØ┤ļŗż[3-5].
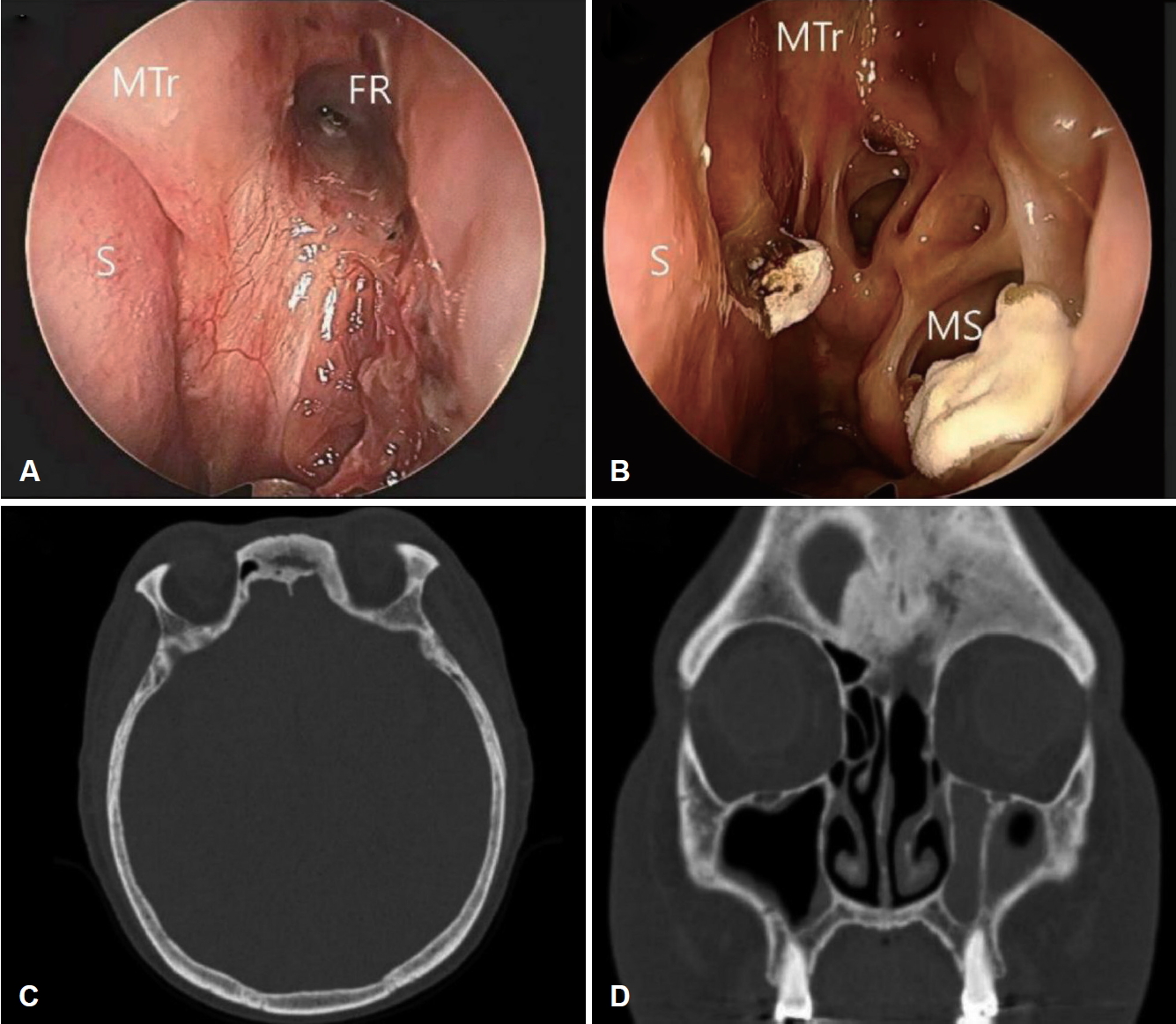
PottŌĆÖs puffy tumor(PPT)ļŖö ņÖĖņāüņØ┤ļéś ņĀäļæÉļÅÖ ļČĆļ╣äļÅÖņŚ╝ņØś ĒĢ®ļ│æņ”Øņ£╝ļĪ£ ņØĖĒĢ£ ņĀäļæÉĻ│©ņØś Ļ│©ļ¦ēĒĢś ļåŹņ¢æņØ┤ļ®░ ĒĢŁņāØņĀ£ņØś ļ│┤ĻĖēĒÖö ņØ┤Ēøä ļ¦żņÜ░ ļō£ļ¼╝Ļ▓ī ņØ╝ņ¢┤ļéśļ®░ ņä▒ņØĖņŚÉĻ▓īņä£ļŖö ļŹö ĒؼĻĘĆĒĢ£ ņ¦łļ│æņØ┤ļŗż. ņĀĆņ×ÉļōżņØĆ ĒÅÉņØ┤ņŗØņØä ļ░øņØĆ Ēøä ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ļź╝ ļ│ĄņÜ® ņżæņØĖ ņä▒ņØĖ ĒÖśņ×ÉņŚÉņä£ ļ¦īņä▒ņĀüņØĖ ĒśĢĒā£ļź╝ ļ│┤ņØ┤ļ®░ PPTļź╝ ļÅÖļ░śĒĢ£ ļ╣äļćīļ¬©ĻĘĀņ”Ø 1ņśłļź╝ Ļ▓ĮĒŚśĒĢśņśĆĻĖ░ņŚÉ ļ¼ĖĒŚī Ļ│Āņ░░Ļ│╝ ĒĢ©Ļ╗ś ļ│┤Ļ│ĀĒĢśļŖö ļ░öņØ┤ļŗż(Fig. 1).
ņ”Ø ļĪĆ
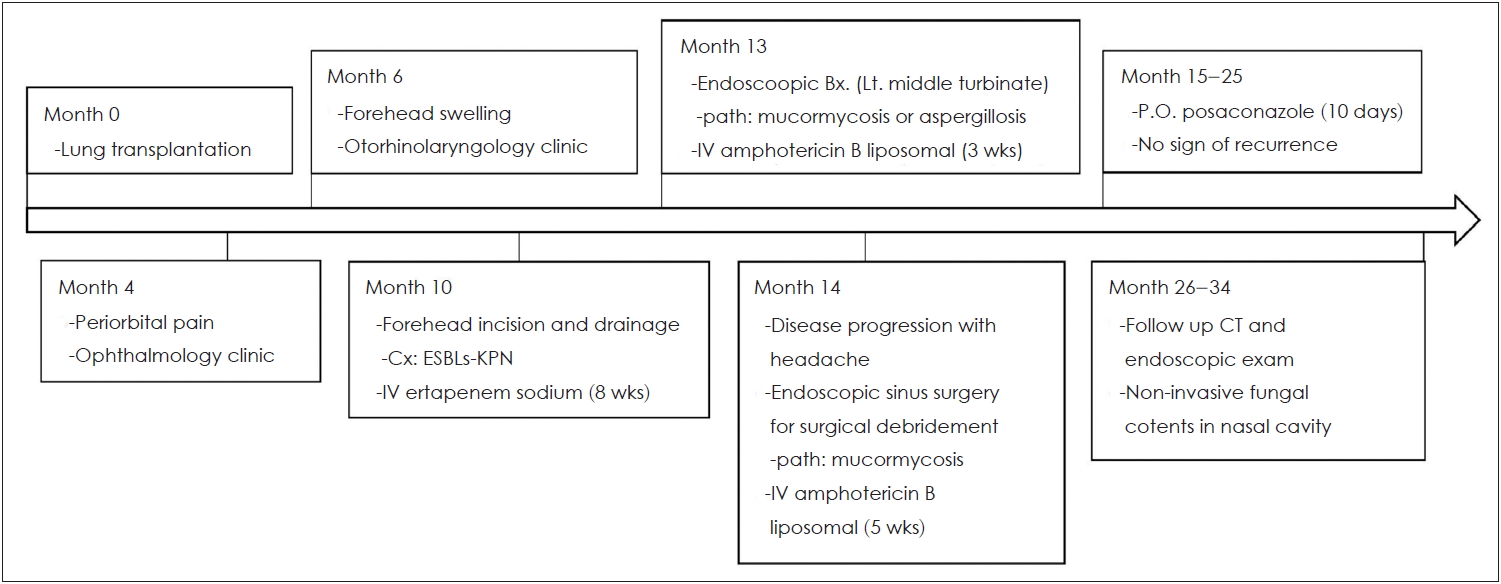
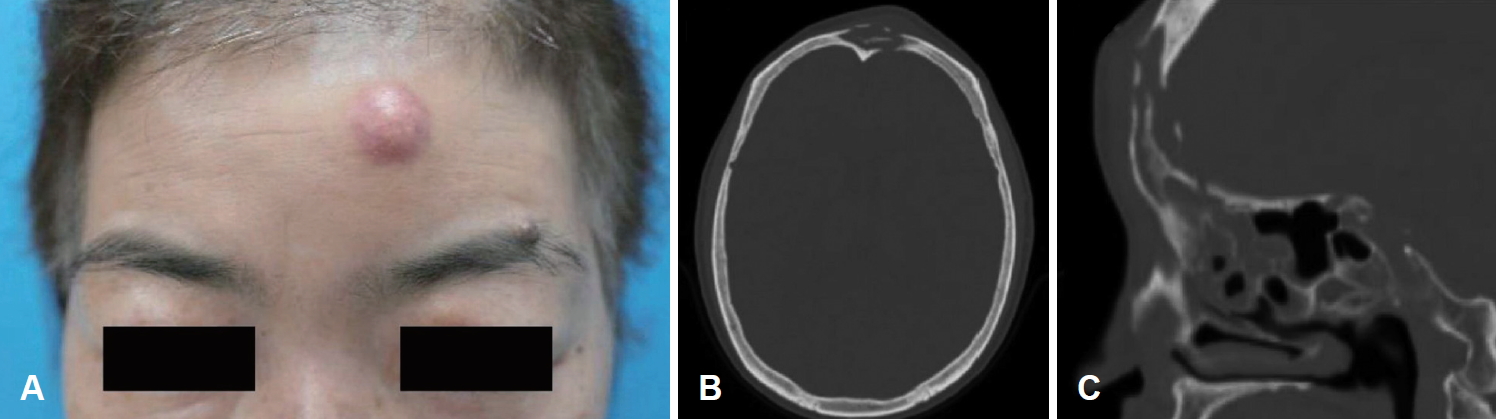
55ņäĖ ņŚ¼ņ×É ĒÖśņ×ÉĻ░Ć 6Ļ░£ņøö ņĀäļČĆĒä░ ņ¦ĆņåŹļÉśļŖö ņóīņĖĪ ņĢłņÖĆ ņŻ╝ņ£ä ļČĆņóģĻ│╝ ļÅÖĒåĄņ£╝ļĪ£ ņĢłĻ│╝ ņ¦äļŻī ņżæ, 4Ļ░£ņøö ņĀäļČĆĒä░ ņ▓£ņ▓£Ē׳ ņ¦äĒ¢ēļÉśļŖö ņóīņĖĪ ņØ┤ļ¦ł 2 cm Ēü¼ĻĖ░ņØś ļÅīņČ£ļÉ£ ĒśĢĒā£ņØś ļ░£ņĀüĻ│╝ ņĢĢĒåĄņØ┤ ļÅÖļ░śļÉ£ ņóģņ░Įņ£╝ļĪ£ ļ│ĖĻ│╝ ņÖĖļל ļé┤ņøÉĒĢśņśĆļŗż(Fig. 2A). ĒÖśņ×ÉļŖö Ļ│ĀĒśłņĢĢ, ņĪ░ņĀłļÉśņ¦Ć ņĢŖļŖö ļŗ╣ļć©, ļ¦īņä▒ņŗĀļČĆņĀäņØś Ļ│╝Ļ▒░ļĀźņØ┤ ņ׳ņŚłņ£╝ļ®░, 10Ļ░£ņøö ņĀä ĒÅÉ ņØ┤ņŗØ Ēøä ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ļź╝ ļ│ĄņÜ® ņżæņØĖ ņāüĒā£ņśĆļŗż.
Lipoid pneumoniaņØś ĻĖēņä▒ ņĢģĒÖöļĪ£ ņØæĻĖēņ£╝ļĪ£ ĒÅÉ ņØ┤ņŗØņØä ļ░øņØĆ ĒÖśņ×ÉņśĆĻĖ░ņŚÉ ĒÅÉ ņØ┤ņŗØ ņĀä paranasal sinus viewļŖö ņŗ£Ē¢ēĒĢśņ¦Ć ņĢŖņĢśņŚłņ£╝ļ®░ ņĢłņÖĆ ņŻ╝ņ£ä ļČĆņóģņØä ņØ┤ņ£ĀļĪ£ ĒÅÉ ņØ┤ņŗØ 4, 6, 10Ļ░£ņøö Ēøä ņĢłĻ│╝ņŚÉņä£ ņŗ£Ē¢ēĒĢ£ caldwell viewņāü ņóīņĖĪ ņĀäļæÉļÅÖņØś Ļ░ĆņĖĪ Ļ▓ĮĻ│ä Ļ▓ĮĒÖö ļ░Å Ļ│©ĒīīĻ┤┤ņä▒ ļ│ĆĒÖöļź╝ ļ│┤ņØ┤ļ®░ ņĀäļæÉļÅÖņØ┤ ĒÖĢņןļÉśĻ│Ā ņ׳ņŚłļŗż. ļ╣äļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņāü ļ╣äĻ░Ģ ļé┤ Ļ░ĆĒö╝ņÖĆ ņÜ®ņóģņä▒ ņĪ░ņ¦üņØ┤ ņżæļ╣äĻ░æĻ░£ ņŻ╝ņ£äņŚÉņä£ Ļ┤Ćņ░░ļÉśņŚłļŗż. Orbit computed tomography(CT)ņāü ņØ┤ļ¦łņØś ņóģņ░ĮĻ│╝ ņØ┤ņ¢┤ņ¦ä ņĀäļæÉļÅÖ ļé┤ ļ│æļ│Ć ļ░Å ņāüņĢłņÖĆļ▓ĮņØś Ļ▓░ņåÉņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 2B and C).
ņóīņĖĪ ņØ┤ļ¦ł ņóģņ░ĮņŚÉ ļīĆĒĢśņŚ¼ external eyebrow incision ņĀæĻĘ╝ļ▓ĢņØä ņØ┤ņÜ®ĒĢ£ ļ░░ļåŹ ļ░Å ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ļ│æļ”¼ ņåīĻ▓¼ņāü Ļ┤┤ņé¼ņä▒ ņĪ░ņ¦üļ¦ī Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░ ņ¦äĻĘĀņØ┤ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśļŗż. ļ░░ņ¢æĻ▓Ćņé¼ Ļ▓░Ļ│╝ extended spectrum ╬▓-lactamase producing Klebsiella pneumoniaeĻ░Ć ļÅÖņĀĢļÉśņ¢┤ 8ņŻ╝Ļ░äņØś IV ertapenem sodium(1 g/day) ņ╣śļŻī Ēøä ĒÖśņ×É ņ”ØņāüņØ┤ ņØ╝ļČĆ ĒśĖņĀäļÉśņŚłļŗż.
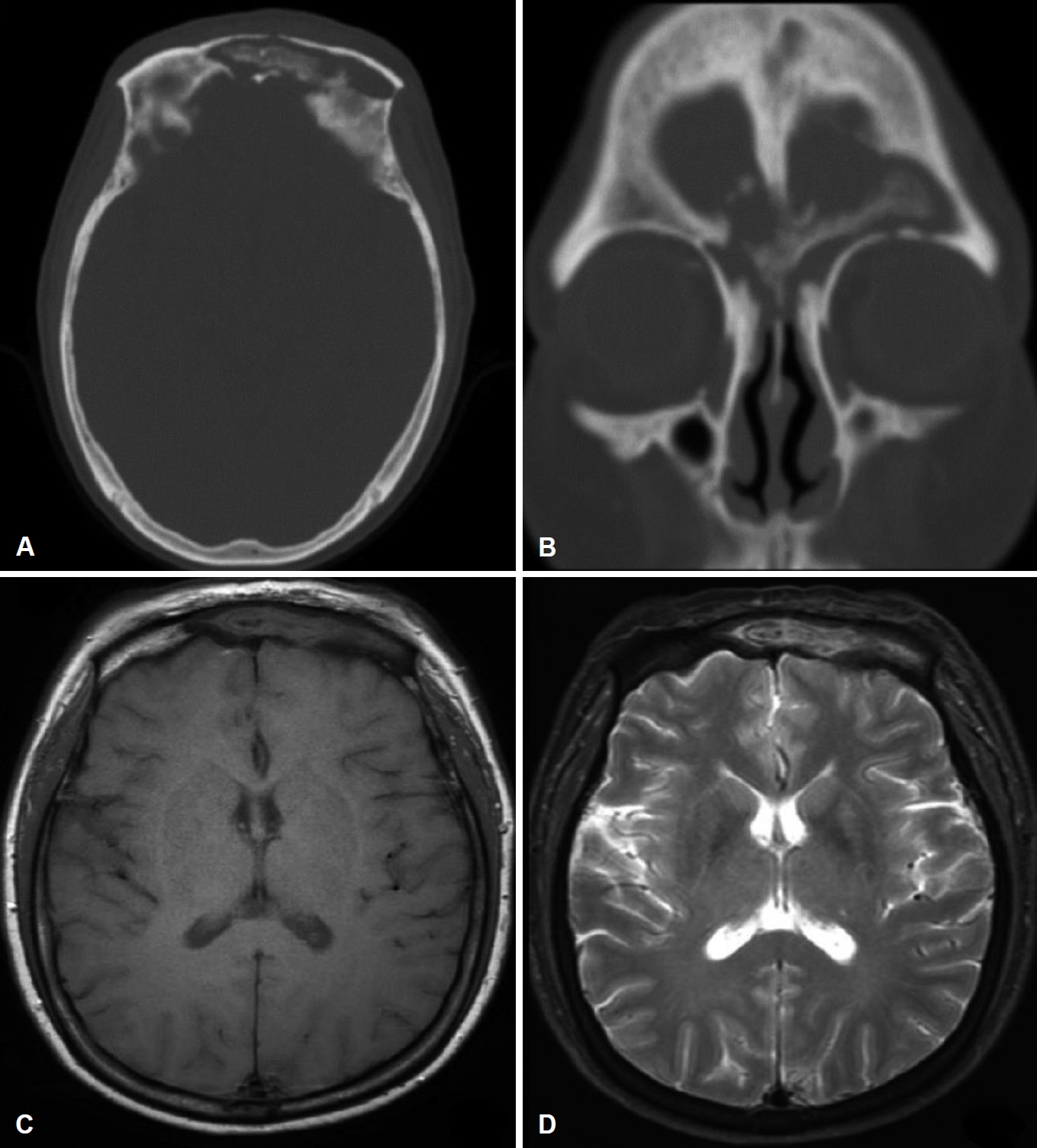
ņĀłĻ░£ ļ░Å ļ░░ļåŹ ņŗ£Ē¢ē 3Ļ░£ņøö Ēøä, ņÖĖļל ļ╣äļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņāü ņżæļ╣äĻ░æĻ░£ļĪ£ ņČöņĀĢļÉśļŖö Ļ│© ņĀłĒÄĖņØ┤ ļ╣äĻ░Ģ ļé┤ņŚÉ ļģĖņČ£ļÉśņ¢┤ ņĪ░ņ¦üĻ▓Ćņé¼ļź╝ ņ¦äĒ¢ēĒĢ£ Ļ▓░Ļ│╝ ļŗżņłśņØś ņ╣©ņŖĄņĀü ņ¢æņāüņØś ĻĘĀņé¼ ņåīĻ▓¼ņØä ļ│┤ņŚ¼ ļ¬©ĻĘĀņ”Ø ļśÉļŖö ņ╣©ņŖĄņĀü ņĢäņŖżĒÄśļź┤ĻĖĖļŻ©ņŖżņ”Ø(aspergillosis)ņØ┤ ņØśņŗ¼ļÉśņŚłļŗż. CTņŚÉņä£ ņĀäļæÉ-ņĢłļ®┤ļČĆņØś ņŚ░ņĪ░ņ¦ü ļČĆņóģ, ņĀäļæÉļÅÖ Ļ│©ĒīīĻ┤┤ņÖĆ ĒĢ©Ļ╗ś ļé┤ļČĆ ļé┤ņÜ®ļ¼╝ņØś ņäØĒÜīĒÖö ņåīĻ▓¼ņØä ļ│┤ņśĆļŗż. ļśÉĒĢ£ MRI T1 Ļ░ĢņĪ░ņśüņāüņŚÉņä£ ņĀĆņŗĀĒśĖ Ļ░ĢļÅä, T2ņŚÉņä£ ļČłĻĘĀņ¦łĒĢ£ Ļ░ĢļÅäņØś fungal ballļĪ£ ņØśņŗ¼ļÉśļŖö ļé┤ņÜ®ļ¼╝ņØ┤ Ļ┤Ćņ░░ļÉśņŚłņ£╝ļ®░ ņ¦üņĀæņĀüņØĖ ļīĆļćī ņ╣©ņŖĄņØĆ ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśņ£╝ļéś ņŻ╝ļ│ĆļČĆļĪ£ Ļ│Āļ░ĆļÅä ņŚ╝ņ”Ø ņåīĻ▓¼ņØ┤ ĒÖĢņØĖļÉśņŚłļŗż. ĒĢ┤ļ®┤ņĀĢļ¦źļÅÖ ļ░Å ļé┤Ļ▓ĮļÅÖļ¦ź ĒśłņĀäņ”ØņØĆ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż (Fig. 3).
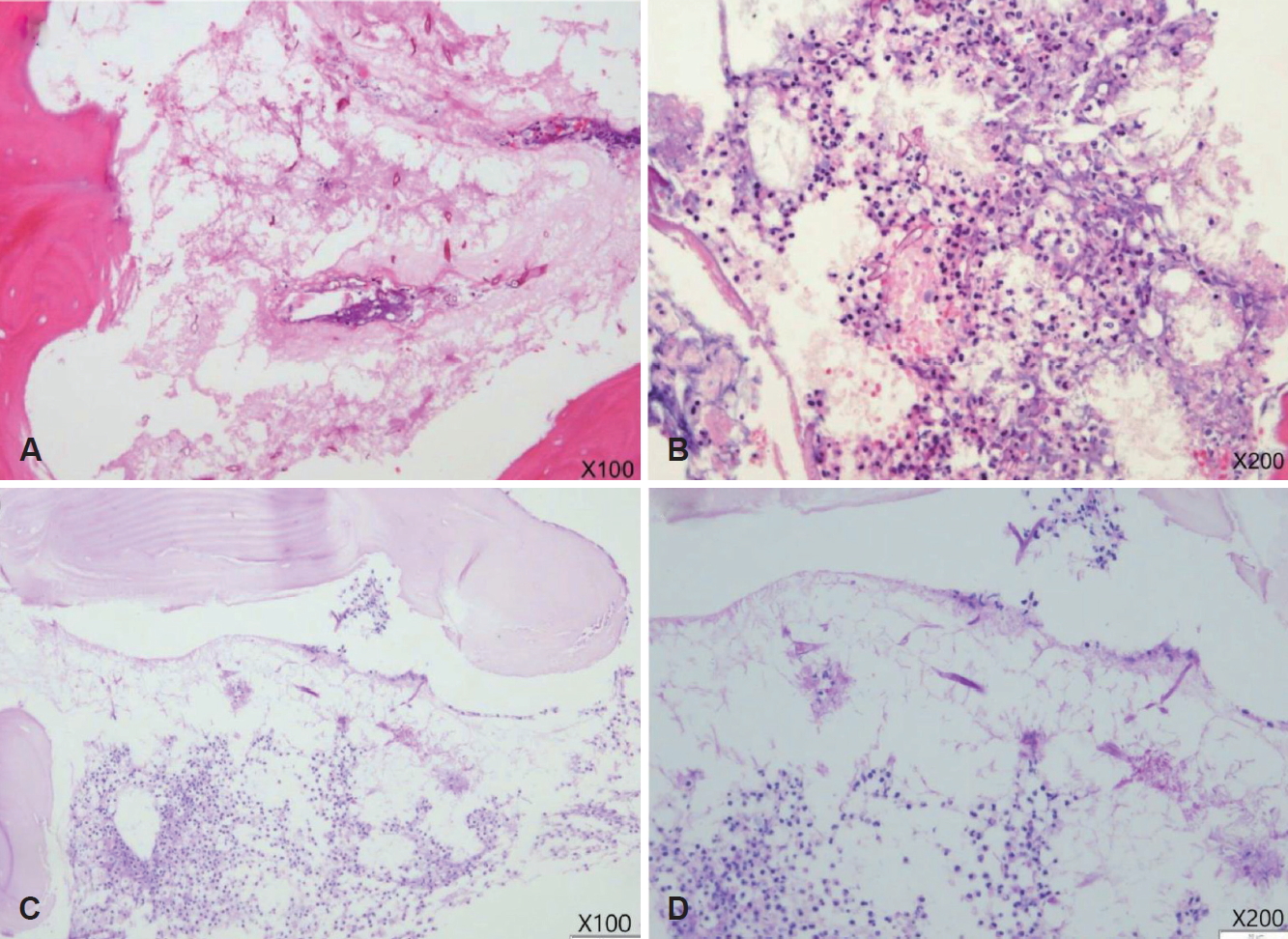
ņ╣©ņŖĄņä▒ ņ¦äĻĘĀņä▒ ļČĆļ╣äļÅÖņŚ╝ ņ¦äļŗ©ĒĢśņŚÉ ņłśņłĀņØä Ļ│äĒÜŹĒĢśņśĆņ£╝ļéś ĻĖ░ņĀĆņ¦łĒÖśņØ┤ ļ¦ÄĻ│Ā ļ¦īņä▒ņĀüņØĖ ņ¢æņāüņ£╝ļĪ£ ĒÖśņ×É ļ░Å ļ│┤ĒśĖņ×ÉĻ░Ć Ļ▒░ļČĆĒĢśņśĆļŗż. ņØ┤ņŚÉ liposomal formņØś IV amphotericin B(250 mg/day) ņ╣śļŻī ņŗ£Ē¢ē ņżæ 3ņŻ╝ņ¦Ė ņ”Øņāü ņĢģĒÖö ļ░Å headacheļź╝ ĒśĖņåīĒĢśņŚ¼ ļŗżņŗ£ ņäżļōØ Ēøä ņłśņłĀņØä Ļ│äĒÜŹĒĢśņśĆļŗż. ņłśņłĀ ņŗ£ ļæÉĻ░£ņĀĆ Ļ▓░ņåÉ, ļćīņ▓ÖņłśņĢĪ ņ£ĀņČ£ņØä ņÜ░ļĀżĒĢśņŚ¼ ņĀĆņ×ÉļōżņØĆ ņÜ░ņäĀ ļæÉĻ░£ņĢłļ®┤ņĀłņĀ£ņłĀņØä ĒåĄĒĢ£ Ļ┤æļ▓öņ£ä ņĀ£Ļ▒░ļź╝ Ļ│ĀļĀżĒĢśņśĆļŗż. ĻĘĖļ¤¼ļéś ĒÖśņ×ÉņØś ņĀäņŗĀ ņāüĒā£ļĪ£ ņØĖĒĢ┤ ĒÜīļ│ĄņØ┤ ņ¢┤ļĀżņÜĖ Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ĒĢśņŚ¼ ļäżļ╣äĻ▓īņØ┤ņģś ļ│┤ņĪ░ĒĢś draf IIb ņłĀĻĖ░ļź╝ ĒåĄĒĢ┤ ļ╣äņĀäļæÉĻ┤ĆņØä Ļ░£ļ░®ĒĢśĻ│Ā Ļ┤Ćņ░░ļÉśļŖö Ļ┤┤ņé¼ņĪ░ņ¦üņØä microdebriderņÖĆ ļō£ļ”┤ņØä ņØ┤ņÜ®ĒĢśņŚ¼ ļ¬©ļæÉ ņĀ£Ļ▒░ĒĢśņśĆņ£╝ļ®░ ļ│æļ”¼ņĪ░ņ¦üĻ▓Ćņé¼ņāü ļ¬©ĻĘĀņ”Øņ£╝ļĪ£ ņ¦äļŗ©ļÉśņŚłļŗż(Fig. 4).
ĒÖśņ×ÉļŖö ņłśņłĀ Ēøä ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ ņĪ░ņĀłņØä ņ£äĒĢ┤ ĒśĖĒØĪĻĖ░ ļé┤Ļ│╝ļĪ£ ņĀäĻ│╝ Ēøä liposomal formņØś IV amphotericin B(250 mg/day)ļź╝ ņłśņłĀ Ēøä 5ņŻ╝Ļ░ä Ēł¼ņŚ¼ĒĢśņśĆņ£╝ļ®░ Ēć┤ņøÉ Ēøä Ļ▓ĮĻĄ¼ ĒĢŁņ¦äĻĘĀņĀ£ļ¦ī(posaconazole 300 mg/day) 10ņØ╝Ļ░ä ņé¼ņÜ®ĒĢśņśĆļŗż.
ņłśņłĀ Ēøä ĒĢ£ ļŗ¼ņ¦Ė ņŗ£Ē¢ēĒĢ£ CT ļ░Å ļ╣äļé┤ņŗ£Ļ▓ĮĻ▓Ćņé¼ņāü ņŻ╝ņ£ä ņĀÉļ¦ēņĪ░ņ¦üņØ┤ ĒÜīļ│ĄļÉśĻ│Ā ņ׳ļŖö Ļ▓āņØä ĒÖĢņØĖĒĢśņśĆļŗż(Fig. 5A). ņłśņłĀ 1ļģä ĒøäļČĆĒä░ ļ╣äņ╣©ņŖĄņĀü ĒśĢĒā£ņØś Ļ│░ĒīĪņØ┤ ļŹ®ņ¢┤ļ”¼Ļ░Ć Ļ┤Ćņ░░ļÉśņŚłņ£╝ļéś ļō£ļĀłņŗ▒ņ£╝ļĪ£ ņēĮĻ▓ī ņĀ£Ļ▒░ļÉśņŚłļŗż(Fig. 5B). Ēśäņ×¼ ņłśņłĀ Ēøä 18Ļ░£ņøöĻ╣īņ¦Ć ņ╣©ņŖĄņĀüņØĖ Ļ│░ĒīĪņØ┤ Ļ░ÉņŚ╝ņ”ØņØĆ ļŹö ņ¦äĒ¢ēļÉśņ¦Ć ņĢŖļŖö ņāüĒā£ļĪ£ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ ņżæņØ┤ļŗż(Fig. 5C and D).
Ļ│Ā ņ░░
ļ¬©ĻĘĀņ”ØņØĆ ņŗØĻĘĀņ×æņÜ®ņØ┤ Ļ░ÉņåīĒĢ£ ļ®┤ņŚŁņĀĆĒĢś ņāüĒā£ļéś ļŗ╣ļć© ĒÖśņ×ÉļōżņŚÉĻ▓ī ļéśĒāĆļéśļŖö ĻĖ░ĒÜīĻ░ÉņŚ╝ņØ┤ļŗż. ĻĖēņä▒ĒśĢņØĆ ļ®┤ņŚŁņĀĆĒĢś ņāüĒā£ņØś ĒÖśņ×ÉļōżņŚÉĻ▓īņä£ ļéśĒāĆļéś 10ņØ╝ ņØ┤ļé┤ņØś ļ╣ĀļźĖ ņĀäĻ░£ ļ░Å ļåÆņØĆ ņé¼ļ¦ØļźĀņØä ļ│┤ņØ┤ļ®░ ļ¦īņä▒ĒśĢņØĆ ļé«ņØĆ ļĀłļ▓©ņØś ļ®┤ņŚŁņĀĆĒĢś ņāüĒā£ņŚÉņä£ ĒśĖļ░£ĒĢśļ®░ Ļ│ĀņĀäņĀüņ£╝ļĪ£ļŖö 4ņŻ╝ ņØ┤ņāü, ņØ╝ļČĆ ņŚ░ĻĄ¼ņŚÉņä£ļŖö 7Ļ░£ņøö ņØ┤ņāü ņ¦ĆņåŹļÉśļŖö Ļ▓Įņ”ØĻ│╝ ļ¼┤ĒåĄņä▒ Ēś╣ņØĆ ņ£ĪņĢäņóģņä▒ ļ│æļ│ĆņØä ņØ┤ļŻ©Ļ│Ā ņäØĒÜīĒÖöļź╝ ĒŖ╣ņ¦Ģņ£╝ļĪ£ ĒĢ£ļŗż[6]. ļśÉĒĢ£ ļ¬©ĻĘĀņ”ØņØĆ ļ░£ņāØ ņןņåīņŚÉ ļö░ļØ╝ņä£ļÅä ļ│Ė ņ”ØļĪĆņÖĆ Ļ░ÖņØ┤ ļŹö ņ╣śļ¬ģņĀüņØĖ Ļ▓░Ļ│╝ļź╝ ļ│┤ņØ╝ ņłś ņ׳ļŖö ļ╣ä-ņĢłņÖĆļīĆļćīĒśĢ Ēś╣ņØĆ ļ╣äļćīĒśĢ(rhino-orbito-cerebral)Ļ│╝ ļ╣äĻĄÉņĀü ņóŗņØĆ ņśłĒøäļź╝ ļ│┤ņØ┤ļŖö ļ╣äļČĆļ╣äļÅÖĒśĢ(sinonasal)ņ£╝ļĪ£ ļéśļłī ņłś ņ׳ļŗż[7]. ļ¦īņä▒ ļ╣äļćīļ¬©ĻĘĀņ”ØņØĆ 1960ļģäļīĆ ņØ┤ĒøäļĪ£ PubMedņŚÉ ņĢĮ 22ņśłļ¦īņØ┤ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŖö ĒؼĻĘĆĒĢ£ ņ¦łĒÖśņØ┤ļ®░ ĻĄŁļé┤ņŚÉņä£ļÅä 2016ļģäņŚÉ ĒĢ£ ņ”ØļĪĆĻ░Ć ļ│┤Ļ│ĀļÉ£ ļ░ö ņ׳ņ£╝ļéś ļ│Ė ņ”ØļĪĆņÖĆļŖö ļŗżļź┤Ļ▓ī ņןĻĖ░ ņØ┤ņŗØ ļ░Å ļ®┤ņŚŁ ņ¢ĄņĀ£ņĀ£ ļ│ĄņÜ®ļĀźņØ┤ ņŚåņŚłņ£╝ļ®░ ļé┤ņŗ£Ļ▓ĮņĀü ņłśņłĀņØ┤ ņĢäļŗī Ļ┤æļ▓öņ£ä ņłśņłĀņĀü ņĀłņĀ£ļź╝ ĒĢśņśĆļŗż[6,8].
ļ¬©ĻĘĀņ”ØņØĆ ĒŖ╣Ē׳ ņĪ░ņĀłļÉśņ¦Ć ņĢŖļŖö ļŗ╣ļć©ņÖĆ ņ╝ĆĒåĀņé░Ēśłņ”ØņØś ņ£Āļ¼┤Ļ░Ć ņżæņÜöĒĢ£ļŹ░ ņØ┤ļĪ£ ņØĖĒĢ┤ ņżæņä▒ĻĄ¼ Ļ░Éņåī ļ░Å ĒÖöĒĢÖņŻ╝ņä▒(chemotaxis)ņØś ņĀĆĒĢ┤Ļ░Ć ļéśĒāĆļéś ņŗØĻĘĀņ×æņÜ®ņØä ņĢĮĒÖöņŗ£Ēéżļ®░ ļŹö ļéśņĢäĻ░Ć ņ╝ĆĒåĀņé░Ēśłņ”ØņØĆ Ēśłņ▓Ł ņ▓ĀņØä ņ”ØĻ░Ćņŗ£ņ╝£ ļ¬©ĻĘĀņ”ØņØś ņ¦äĒ¢ēņØä Ļ░ĆņåŹĒÖöņŗ£ĒéżĻĖ░ ļĢīļ¼ĖņØ┤ļŗż[9]. ļ│Ė ņ”ØļĪĆņØś Ļ▓ĮņÜ░ ņĪ░ņĀłļÉśņ¦Ć ņĢŖļŖö ļŗ╣ļć©ņØś Ļ│╝Ļ▒░ļĀźņØĆ ņ׳ņŚłņ£╝ļéś ļ¬ģĒÖĢĒĢ£ ņ╝ĆĒåĀņé░Ēśłņ”ØņØĆ ņŚåņŚłļŗż.
ņ×äņāü ņ¢æņāüņØĆ ļīĆĻ░£ ņØ╝ļ░śņĀüņØĖ ļČĆļ╣äļÅÖņŚ╝ ņ”Øņāü ļ░Å ņĢłļ®┤ĒåĄ, ņĢłņÖĆļČĆņóģ, ļ░£ņŚ┤, Ēśłņä▒ ļ╣äļŻ© ļō▒ņØ┤ ļ©╝ņĀĆ ļéśĒāĆļéśļ®░, ņ▓½ ņ”Øņāüņ£╝ļĪ£ ņĢłĻ│╝ņĀü ņ”ØņāüņØä ĒśĖņåīĒĢśļŖö Ļ▓ĮņÜ░Ļ░Ć Ļ░Ćņן ļ¦Äļŗż[10]. ļ│æņØ┤ ņ¦äĒ¢ēļÉ©ņŚÉ ļö░ļØ╝ ņĢłĻĘ╝ļ¦łļ╣ä, ņĢłĻ▓ĆĒĢśņłś, ņĢłļ®┤ņŗĀĻ▓Įļ¦łļ╣ä ļō▒ņØ┤ ļ░£ņāØĒĢĀ ņłś ņ׳ņ£╝ļ®░ ļ¦īņä▒ņØś Ļ▓ĮņÜ░ ĒĢ┤ļ®┤ņĀĢļ¦źļÅÖ ļ░Å ļé┤Ļ▓ĮļÅÖļ¦ź ĒśłņĀäņ”ØņØ┤ ļŹö ņל ņØ╝ņ¢┤ļé£ļŗż[11]. ĻĘĖļ¤¼ļéś ļ╣äļćīļ¬©ĻĘĀņ”ØņØ┤ ņĀäļæÉĻ│©ņØś Ļ│©ļ¦ēĒĢś ļåŹņ¢æņØä ņØ╝ņ£╝ĒéżļŖö Ļ▓ĮņÜ░ļŖö ļ¦żņÜ░ ļō£ļ¼╝ļ®░ ĻĄŁļé┤ņŚÉņä£ļŖö ļæÉ ļ▓łņ¦Ė ņ”ØļĪĆņŚÉ ĒĢ┤ļŗ╣ĒĢ£ļŗż[12].
ļ¦īņä▒ ļ╣äļćīļ¬©ĻĘĀņ”ØņØś ņøÉņØĖ ĻĘĀņØĆ ņ”ØļĪĆĻ░Ć ņĀüņ¢┤ Mucor ramosissimus, Rhizopus nigricans, Mucor irregularis ņĀĢļÅäļ¦īņØ┤ ĒÖĢņØĖļÉśņŚłņ£╝ļ®░, ļ¬©ļæÉ ņĢĮ 36┬░C ņØ┤ņāüņØś ņ▓┤ņś©Ļ│╝ ņ£Āņé¼ĒĢ£ ņś©ļÅäņŚÉņä£ ņä▒ņןņØ┤ ļæöĒÖöļÉśĻ▒░ļéś ļ®łņČöļŖö Ļ▓ĮĒ¢źņØä ļ│┤ņŚ¼ ņØ┤ļĪ£ ņØĖĒĢ┤ ļ╣äĻĄÉņĀü ļŖÉļ”░ ņ¦äĒ¢ē ņ¢æņāüņØä ļéśĒāĆļé┤ļŖö Ļ▓āņ£╝ļĪ£ ņ£ĀņČöĒĢĀ ņłś ņ׳ļŗż[10,13].
ņØ┤ĒĢÖņĀü Ļ▓Ćņé¼ņāüņŚÉņä£ļŖö ļ╣äĻ░Ģ ļ░Å ļČĆļ╣äļÅÖņØś Ļ▓ĆņØĆņāē Ļ░ĆĒö╝, Ļ┤┤ņé¼ņä▒ ņĪ░ņ¦ü ņåīĻ▓¼ ļō▒ņØ┤ ĒÖĢņØĖļÉ£ļŗż[14]. CT ņåīĻ▓¼ņāü Ļ│©ļ»Ėļ×ĆĻ│╝ Ļ│©ĒīīĻ┤┤ ļ░Å ņäØĒÜīĒÖö ņåīĻ▓¼ņØ┤ ļéśĒāĆļéĀ ņłś ņ׳ņ£╝ļ®░, MRI T1, T2 Ļ░ĢņĪ░ņśüņāü ļ¬©ļæÉņŚÉņä£ ņĀĆņŗĀĒśĖ Ļ░ĢļÅäņØś ļ│æļ│ĆņØ┤ ļéśĒāĆļéśļŖö Ļ▓ĮņÜ░Ļ░Ć ļ¦Äļŗż. ļö░ļØ╝ņä£ ļ╣äĒŖ╣ņØ┤ņĀüņØĖ ņśüņāü ņåīĻ▓¼ļ¦īņ£╝ļĪ£ ļ¦īņä▒ ņ╣©ņŖĄņĀü ļ¬©ĻĘĀņ”ØĻ│╝ ņĢģņä▒ ļ│æļ│ĆņØä ļ¬ģĒÖĢĒ׳ Ļ░Éļ│äĒĢśļŖö Ļ▓āņØĆ ņ¢┤ļĀżņÜ░ļ»ĆļĪ£ ļ│æļ”¼ ņ¦äļŗ©ņØ┤ ĒÖĢņ¦äņŚÉ ĒĢäņłśņĀüņØ┤ļ®░ GrocottŌĆÖs methenamine silver-periodic acid Schiff, hematoxylin and eosin ņŚ╝ņāēņØä ĒåĄĒĢ┤ ņ¦üĻ░üņ£╝ļĪ£ Ļ░Ćņ¦Ćļź╝ ļé┤ļŖö Ļ▓®ļ▓Į ņŚåļŖö ĻĘĀņé¼ļź╝ Ļ┤Ćņ░░ĒĢĀ ņłś ņ׳ļŗż[3].
PPTļŖö ņĀäļæÉĻ│©ņØś Ļ│©ļ¦ēĒĢśļåŹņ¢æņØä ņØśļ»ĖĒĢśļ®░ ņĀäļæÉļÅÖņØś ņŚ╝ņ”ØņØ┤ ļłäĻ│ĄņŚÉ ņØśĒĢ┤ ĒīīĻĖēļÉśņ¢┤ Ļ│©ņłśņŚ╝ ļ░Å ļåŹņ¢æņØś ĒśĢņä▒ņ£╝ļĪ£ ņØ┤ņ¢┤ņ¦äļŗż. 1768ļģä Percivall PottņŚÉ ņØśĒĢ┤ ņÖĖņāüņŚÉ ņØśĒĢ£ Ļ▓āņ£╝ļĪ£ ņ▓śņØī ņĀĢņØśļÉśņŚłņ£╝ļéś ņØ┤Ēøä ņĀäļæÉļÅÖ ļČĆļ╣äļÅÖņŚ╝ņ£╝ļĪ£ ņØĖĒĢ£ ņ”ØļĪĆļōżļÅä ļ│┤Ļ│ĀļÉśņŚłļŗż. ņÖäņĀäĒ׳ ļ░£ļŗ¼ļÉśņ¦Ć ņĢŖņØĆ ņĀäļæÉļÅÖņØś ĒĢ┤ļČĆĒĢÖņĀü ĻĄ¼ņĪ░ļéś ņĢäņØ┤ļōżņŚÉĻ▓ī ĒØöĒĢ£ ĒīÉņé¼ņØ┤ņĀĢļ¦źņØś Ēśłļźś ņ”ØĻ░ĆļĪ£ ņØĖĒĢ┤ ĒØöĒĢśĻ▓ī ļ░£ļ│æĒĢśņŚ¼ ņä▒ņØĖņŚÉĻ▓īņä£ļŖö ļō£ļ¼╝ļ®░ ņŻ╝ļĪ£ 10~20ņäĖņŚÉ ĒØöĒĢśĻ▓ī ļ░£ļ│æĒĢ£ļŗż. ņĀäļæÉĻ│© ĒåĄņ”Ø, ļæÉĒåĄ, ņĢłņÖĆ ļČĆņóģ, ļ░£ņŚ┤ ļō▒ņØś ņ×äņāü ņ”ØņāüņØ┤ ņ׳ņ£╝ļ®░ Ļ░ÉņŚ╝ņØ┤ ļīĆļćīĻ╣īņ¦Ć ĒīīĻĖēļÉĀ ņŗ£ ļćīņłśļ¦ēņŚ╝, Ļ▓Įļ¦ēņÖĖ ļåŹņ¢æ, ļćīļåŹņ¢æņ£╝ļĪ£ ņĢģĒÖöļÉĀ ņłś ņ׳ļŗż. ĒĢŁņāØņĀ£ ņ╣śļŻīļ¦īņ£╝ļĪ£ļŖö ļ│┤ĒåĄ ļČĆņĀüĒĢ®ĒĢśļ®░ ļīĆļČĆļČäņØś ĒÖśņ×ÉļōżņØĆ ņłśņłĀņĀü ļ░░ļåŹņØä Ļ░ÖņØ┤ ĒĢäņÜöļĪ£ ĒĢ£ļŗż[15]. ļ│Ė ņ”ØļĪĆļŖö ļ¬©ĻĘĀņ”ØņŚÉ ņØśĒĢ£ PPTņØś Ļ▓ĮņÜ░ļĪ£ ļé┤ņŗ£Ļ▓ĮņØä ņØ┤ņÜ®ĒĢ£ Ļ┤┤ņé¼ ņĪ░ņ¦üņØś ņĀłņĀ£, amphotericin BņØś Ēł¼ņŚ¼, ĻĖ░ņĀĆņ¦łĒÖśņØś ĻĄÉņĀĢ ļ░Å ņ╣śļŻīļź╝ Ļ░ÖņØ┤ ņŗżņŗ£ĒĢśņśĆļŗż[4,14].
ļ│Ė ņ”ØļĪĆņŚÉņä£ļŖö ņØ┤ļ¦łņŚÉ ļÅīņČ£ļÉ£ ĒśĢĒā£ņØś ļ░£ņĀüĻ│╝ ņĢĢĒåĄņØ┤ ļÅÖļ░śļÉ£ ņóģņ░ĮĻ│╝ ņĢłņÖĆļČĆņóģņØä ņ▓½ ņ”Øņāüņ£╝ļĪ£ ļé┤ņøÉĒĢ£ ĒÖśņ×ÉĻ░Ć ĒÅÉņØ┤ņŗØ Ēøä ļ®┤ņŚŁņ¢ĄņĀ£ņĀ£ ļ│ĄņÜ® ļ░Å ņĪ░ņĀłļÉśņ¦Ć ņĢŖļŖö ļŗ╣ļć© ļ│æļĀźņØ┤ ļÅÖļ░śļÉśņŚłņ£╝ļ®░, PPTĻ░Ć ļÅÖļ░śļÉśņŚłļŗżļŖö ņĀÉņŚÉņä£ ĻĖ░ņĪ┤ņØś ņ”ØļĪĆļōżĻ│╝ ļ╣äĻĄÉ ņŗ£ ņØśļ»ĖĻ░Ć ņ׳ļŗż. ņ╣śļŻī ļ░®ļ▓ĢļÅä ņØ╝ļ░śņĀüņØĖ ļæÉĻ░£ņĢłļ®┤ņĀłņĀ£ņłĀņØ┤ ņĢäļŗī ņĄ£ĻĘ╝ ļīĆļæÉļÉśļŖö ļé┤ņŗ£Ļ▓ĮņØä ņØ┤ņÜ®ĒĢ£ draf IIb ļ░®ļ▓ĢĻ│╝ ĒĢŁņ¦äĻĘĀņĀ£ ņé¼ņÜ®ņØä ļ│æņÜ®ĒĢśņśĆļŗż.