ņä£ ļĪĀ
ļæÉĻ▓ĮļČĆ ĒÄĖĒÅēņāüĒö╝ņäĖĒż ņĢöņóģ(head and neck squamous cell carcinoma, HNSCC)ņØĆ ņØ╝Ļ│▒ ļ▓łņ¦Ė Ļ░Ćņן ĒØöĒĢ£ ņĢöņ£╝ļĪ£ ņŚ░Ļ░ä ņĀäņäĖĻ│äņĀüņ£╝ļĪ£ 60ļ¦ī Ļ▒┤ ņØ┤ņāüņØś ļ░£ņāØļźĀņØä ļ│┤ņØĖļŗż[1]. ļæÉĻ▓ĮļČĆņĢöņØĆ ņĪ░ĻĖ░ņĢöņØ┤ļéś ĻĄŁņåī ņ¦äĒ¢ēņĢöņØś Ļ▓ĮņÜ░ ņ╣śļŻī ņä▒ņĀüņŚÉ ņ׳ņ¢┤ Ļ┤äļ¬®ĒĢĀļ¦īĒĢ£ ļ░£ņĀäņØ┤ ņ׳ņŚłņ¦Ćļ¦ī ņ×¼ļ░£ĒĢśņśĆĻ▒░ļéś ņøÉĻ▓®ņĀäņØ┤ļź╝ ļÅÖļ░śĒĢ£ Ļ▓ĮņÜ░ņŚÉļŖö ņ╣śļŻī ņä▒ņĀüņØ┤ Ļ│╝Ļ▒░ņŚÉ ļ╣äĒĢ┤ ĒśäņĀĆĒ׳ Ļ░£ņäĀļÉśņŚłļŗżĻ│Ā ļ¦ÉĒĢśĻĖ░ ņ¢┤ļĀĄļŗż. ņĄ£ĻĘ╝ ļČäņ×ÉņāØļ¼╝ĒĢÖņĀü ĻĖ░ļ▓ĢĻ│╝ ņ¦ĆņŗØņØ┤ ļłłļČĆņŗ£Ļ▓ī ļ░£ņĀäĒĢśļ®┤ņä£ ņĢöņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ļÅä ĒŖ╣ņĀĢ ļČäņ×Éļź╝ Ēæ£ņĀüņ£╝ļĪ£ ĒĢśļŖö ņ╣śļŻī, ņØ┤ļźĖļ░ö ļČäņ×É Ēæ£ņĀü ņĢöņ╣śļŻī(molecular targeted cancer therapy)ņŚÉ ļīĆĒĢ£ ĻĖ░ļīĆĻ░Ć ļåÆņĢäņ¦ĆĻ│Ā ņ׳ļŗż.
Ēæ£Ēö╝ ņä▒ņןņØĖņ×É ņłśņÜ®ņ▓┤(epidermal growth factor receptor, EGFR)ļŖö ļæÉĻ▓ĮļČĆņĢöņØä ĒżĒĢ©ĒĢ£ ņŚ¼ļ¤¼ ņĢöņóģņŚÉņä£ Ļ░Ćņן ņŚ░ĻĄ¼Ļ░Ć ļ¦ÄņØ┤ ņ¦äĒ¢ēļÉ£ Ēæ£ņĀüņØĖņ×É ņżæņŚÉ ĒĢśļéśļĪ£ ļæÉĻ▓ĮļČĆņĢöņŚÉņä£ļŖö 90% ņØ┤ņāüņŚÉņä£ Ļ│╝ļ░£ĒśäļÉ£ļŗżļŖö ņĀÉņŚÉņä£ ņ×äņāüņĀüņ£╝ļĪ£ ņżæņÜöĒĢśĻ▓ī ņŚ¼Ļ▓©ņĀĖ ņÖöļŗż[2,3].
EGFR Ļ│╝ļ░£ĒśäņØĆ ļéśņü£ ņśłĒøä, ņóģņ¢æ ņä▒ņןņØś ņ”ØĻ░Ć, ņĀäņØ┤, ĒÖöĒĢÖņÜöļ▓Ģ ļ░Å ļ░®ņé¼ņäĀ ņÜöļ▓ĢņŚÉ ļīĆĒĢ£ ļé┤ņä▒Ļ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŖöļŹ░ ņĢäņ¦üĻ╣īņ¦Ć ņåīļČäņ×É Ēŗ░ļĪ£ņŗĀ ĒéżļéśņĢäņĀ£ ņ¢ĄņĀ£ņĀ£ļéś EGFRņŚÉ ļīĆĒĢ£ ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤, cetuximab ļ░Å panitumumabņŚÉ ņØśĒĢ£ ļŗ©ļÅģ ņÜöļ▓ĢņØĆ ļæÉĻ▓ĮļČĆņĢöņŚÉņä£ ĒÜ©Ļ│╝Ļ░Ć ņĀ£ĒĢ£ņĀüņØ┤ļŗż[4-7]. ļö░ļØ╝ņä£ ļæÉĻ▓ĮļČĆņĢö ĒÖśņ×ÉņŚÉņä£ ņĢĮļ¼╝ ņĀĆĒĢŁņä▒Ļ│╝ ņĀ£ĒĢ£ļÉ£ ļ░śņØæļźĀņØä ĻĘ╣ļ│ĄĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ļīĆņ▓┤ ņ╣śļŻīļ▓ĢņØ┤ ĒĢäņÜöĒĢśļŗż. ĻĘĖņżæ ĒĢśļéśĻ░Ć ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻī(radioimmunotherapy, RIT)Ļ░Ć ļÉĀ ņłś ņ׳ļŗż.
ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīņØś ĒĢŁņĢö ĻĖ░ņĀä
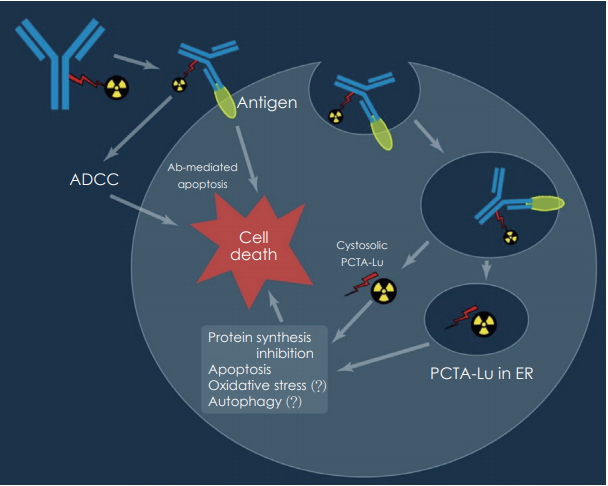
ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīļŖö ĒĢŁņ▓┤ ņØśņĪ┤ņä▒ ņäĖĒżļÅģņä▒(antibody dependent cellular cytotoxicity) ļ░Å ļ│┤ņ▓┤ ņØśņĪ┤ņä▒ ņäĖĒżļÅģņä▒(complement dependent cytotoxicity) ĻĖ░ņĀäņØä ņØ┤ņÜ®ĒĢ£ ĻĖ░ņĪ┤ņØś ļŗ©ļ░▒ļ®┤ņŚŁĒĢŁņ▓┤ņŚÉ ņØśĒĢ£ ļ®┤ņŚŁņ╣śļŻīĒÜ©Ļ│╝ņŚÉ ĒĢŁņ▓┤ņŚÉ ņĀæĒĢ®ļÉ£ ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīņŚÉņä£ ļ░®ņČ£ļÉśļŖö ļ░®ņé¼ņäĀņŚÉ ņØśĒĢ£ ŌĆ£cross-fireŌĆØ ĒÜ©Ļ│╝ļź╝ ņØ┤ņÜ®ĒĢśļŖö ņ╣śļŻīļ▓ĢņØ┤ļŗż. ļ¦ÄņØĆ ņĀäņ×äņāü ļ░Å ņ×äņāüņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ņä£ ļ░®ņé¼ņä▒ ļ®┤ņŚŁ ņĀæĒĢ®ņ▓┤(radioimmunoconjugate)(ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīļĪ£ Ēæ£ņ¦ĆļÉ£ ĒĢŁņ▓┤)ļź╝ ņØ┤ņÜ®ĒĢ£ ļ®┤ņŚŁņ╣śļŻīĻ░Ć ļ╣äņĀæĒĢ® ĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ ļŗ©ļÅģ ļ®┤ņŚŁņ╣śļŻī ņÜöļ▓Ģļ│┤ļŗż ņ×äņāüņĀüņ£╝ļĪ£ ņ£ĀņØśĒĢśĻ▓ī ļø░ņ¢┤ļé£ ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļ│┤ņØ┤ļŖö Ļ▓āņØ┤ ļ│┤Ļ│ĀļÉśņ¢┤ņĀĖ ņÖöļŗż[8-10].
ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīļŖö ļ®┤ņŚŁ ļŗ©ļ░▒ņ¦łņØä ļ░®ņé¼ļŖźņØś ņÜ┤ļ░śņ×É, ņČöņĀüņ×É ļśÉļŖö Ēæ£ņĀü ņ╣śļŻīņĀ£ļĪ£ ņØ┤ņÜ®ĒĢ£ļŗż. ļ░®ņé¼ņäĀ ļ®┤ņŚŁ ņĀæĒĢ®ņ▓┤ļŖö ņóģņ¢æ, ĒØēļ¦ē ņŻ╝ņ£ä ļśÉļŖö ĒØēļ¦ēĻ░ĢĻ│╝ Ļ░ÖņØĆ ņ▓┤Ļ░Ģ ļé┤ļĪ£ ņ¦üņĀæ ņŻ╝ņé¼ļÉśĻ▒░ļéś ņĀĢļ¦ź ļé┤ļĪ£ ņŻ╝ņ×ģļÉśĻ│Ā, ņØ╝ļŗ© ņŻ╝ņ×ģļÉśļ®┤ ļ░®ņé¼ņä▒ ĒĢŁņ▓┤ļŖö Ēśłļźś, ĒÖĢņé░ ļśÉļŖö ļīĆļźśņŚÉ ņØśĒĢ┤ ņóģņ¢æņäĖĒż ņāüņØś ĒĢŁņøÉ-Ļ▓░ĒĢ® ļČĆņ£äņŚÉ ļČäĒżĒĢśĻ▓ī ļÉśļ®┤ņä£ ļ░®ņé¼ņä▒ ĒĢĄņóģņØś ļČĢĻ┤┤ ņżæņŚÉ ļ░£ņāØĒĢśļŖö ņŚäņ▓Łļé£ ņŚÉļäłņ¦Ć ļ░®ņČ£ļĪ£ ņØĖĒĢ£ ļ░®ņé¼ņäĀ ĒÜ©Ļ│╝ļĪ£ ņóģņ¢æņŚÉ ļīĆļ¤ēņØś ņé┤ĻĘĀ ņäĀļ¤ēņØä ņĀäļŗ¼ĒĢ┤ņä£ ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļéśĒāĆļéśĻ▓ī ļÉ£ļŗż(Fig. 1).
ņ×äņāüņĀüņ£╝ļĪ£ RITļŖö ĻĘĖļÅÖņĢł ļ░®ņé¼ņäĀ ļ»╝Ļ░Éņä▒ ņóģņ¢æ, ĒŖ╣Ē׳ ļ╣äĒśĖņ¦ĆĒé© ļ”╝Ēöäņóģ(Non HodgkinŌĆÖs lymphoma, NHL) ņ╣śļŻīņŚÉ ņ׳ņ¢┤ ņŚäņ▓Łļé£ ņä▒Ļ│ĄņØä Ļ▒░ļæÉņ¢┤ ņÖöĻ│Ā, ĻĘĖ Ļ▓░Ļ│╝ CD-20 ļ░£Ēśä B ņäĖĒż ļ”╝ĒöäņóģņŚÉņä£ 90Yttrium(90Y) Ēæ£ņ¦Ć ibritumomab tiuxetan(ZevalinŌōć)Ļ│╝ 131iodine(131I) Ēæ£ņ¦Ć tositumomab(BexxarŌōć)Ļ░Ć Ēśäņ×¼ FDA ņŖ╣ņØĖņØä ļ░øņĢäņä£ ņ×äņāü ņĀüņÜ®ņØ┤ ļÉśĻ│Ā ņ׳ļŗż.
Ļ│ĀĒśĢņĢöņŚÉņä£ņØś ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻī
ĒśłņĢĪņĢö ļ░Å ļ”╝ĒöäņóģņŚÉņä£ ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīņØś ļø░ņ¢┤ļé£ ņ╣śļŻī ĒÜ©Ļ│╝ļĪ£ ņØĖĒĢ┤ņä£ ņ×äņāü ņĀüņÜ®ņØ┤ ĒÖ£ļ░£ĒĢ£ ļ░śļ®┤ņŚÉ ĻĘĖļÅÖņĢł Ļ│ĀĒśĢņĢöņŚÉņä£ņØś RITņØś ņ╣śļŻī ĒÜ©Ļ│╝ļŖö ņ×äņāüņĀüņ£╝ļĪ£ ņĀ£ĒĢ£ņĀüņØ┤ņŚłļŗż[11].
ļæÉĻ▓ĮļČĆņĢö, ņ£Āļ░®ņĢö, ļé£ņåīņĢö, ļīĆņןņĢö, ņĀäļ”ĮņäĀņĢö, ņŗĀņןņĢö ļ░Å ļćīņĢöņØä ļ╣äļĪ»ĒĢ£ ļŗżņ¢æĒĢ£ ņóģļźśņØś Ļ│ĀĒśĢ ņóģņ¢æņØä ņ╣śļŻīĒĢśĻĖ░ ņ£äĒĢ┤ ņłśļ¦ÄņØĆ ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤Ļ░Ć Ļ░£ļ░£ ņżæņŚÉ ņ׳ļŗż(Table 1). ņØ┤ļ¤¼ĒĢ£ ļ¬©ļōĀ ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤ļŖö ļæÉ Ļ░Ćņ¦Ć ņ╣śļŻī ņÜöņåī, ņ”ē ļ░®ņé¼ņäĀņŚÉ ņØśĒĢ£ ņ╣śļŻī ĒÜ©Ļ│╝ ļ░Å ĒĢŁņøÉ ĒĢŁņ▓┤ Ļ▓░ĒĢ® ņŗ£ ĒĢŁņ▓┤ņŚÉ ņØśĒĢ£ ņ×æņÜ®ņØä ĒåĄĒĢ┤ ņĢöņäĖĒżļź╝ ņŻĮņØ╝ ņ×Āņ×¼ļĀźņØä Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗż. ļ░®ņé¼ņäĀņŚÉ ņØśĒĢ£ ņĢöņäĖĒż ņé¼ļ®ĖņØĆ ņŻ╝ļĪ£ DNA ņåÉņāüņŚÉ ņØśĒĢ£ Ļ▓āņ£╝ļĪ£ ņĢöņäĖĒżņŚÉ ļ░®ņé¼ņäĀņØ┤ ņĪ░ņé¼ļÉśļ®┤ DNA ļŗ©ņØ╝ Ļ░Ćļŗź ņĀłļŗ©(single-strand break)Ļ│╝ ņØ┤ņżæĻ░Ćļŗź ņĀłļŗ©(double-strand break)ņØ┤ ļ░£ņāØļÉ£ļŗż. ļ░®ņé¼ņäĀņŚÉ ņØśĒĢ£ ņäĖĒż ņé¼ļ®ĖņØ┤ ņÜ░ņäĖĒĢ£ ļ░®ņé¼ņäĀ Ļ░Éņłśņä▒ NHLĻ│╝ ļ╣äĻĄÉĒĢĀ ļĢī, ļīĆļČĆļČäņØś Ļ│ĀĒśĢ ņóģņ¢æņØĆ ļ░®ņé¼ņäĀ ņĪ░ņé¼ ĒøäņŚÉ ņäĖĒżņ×Éļ®Ėņé¼ļź╝ Ļ▒░ņØś ļ│┤ņØ┤ņ¦Ć ņĢŖļŖöļŗż. Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£ ļ░®ņé¼ņäĀ ļ»╝Ļ░Éņä▒ NHLņŚÉ ļ╣äĒĢ┤ Ļ│ĀĒśĢ ņóģņ¢æņØä ņŻĮņØ┤ĻĖ░ ņ£äĒĢ┤ņä£ļŖö Ēø©ņö¼ ļåÆņØĆ ļ░®ņé¼ņäĀļ¤ēņØ┤ ĒĢäņÜöĒĢśļŗż. ņØ┤ļŖö Ļ│ĀĒśĢņĢö ļ░£ņāØņØś ĻĖ░ņøÉ ņäĖĒżĻ░Ć ņāüļīĆņĀüņ£╝ļĪ£ ĒśłņĢĪņĢöņŚÉ ļ╣äĒĢ┤ņä£ ļ░®ņé¼ņäĀ ņĀĆĒĢŁņä▒ņØ┤ ļåÆņØĆ ĒŖ╣ņä▒ņŚÉ ĻĖ░ņØĖĒĢ£ļŗż. ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ ļ│┤Ļ│Āļź╝ ĒåĄĒĢ┤ ņĀäļ”ĮņäĀņĢö(64.8~81 Gy) [12], ĒÅÉņĢö(40~65 Gy) [13], ņŗĀĻ▓ĮņĢäĻĄÉņóģ(60 Gy) [14], ļīĆņןņĢö(70 Gy) [15]Ļ│╝ Ļ░ÖņØĆ Ļ│ĀĒśĢ ņóģņ¢æņŚÉņä£ ņ×äņāü ļ░śņØæņØä ņ¢╗ĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņĄ£ņåīĒĢ£ ļ░®ņé¼ņäĀļ¤ēņØ┤ 50 GyņŚÉ ļÅäļŗ¼ĒĢ┤ņĢ╝ ĒĢśļŖöļŹ░ Ļ│ĀĒśĢ ņóģņ¢æņŚÉņä£ ļ│┤Ļ│ĀļÉ£ ļīĆļČĆļČäņØś ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ ņóģņ¢æņŚÉ ļÅäļŗ¼ĒĢ£ ļ░®ņé¼ņäĀļ¤ēņØĆ 50 Gy ņØ┤ĒĢśļĪ£ ļ│┤Ļ│ĀļÉ£ļŗż. ņØ┤ļ¤░ ņ╣śļŻī ĒÜ©Ļ│╝ņØś ņĀ£ĒĢ£ņĀÉņØä ĻĘ╣ļ│ĄĒĢśĻ│Ā ņĪ░ņ¦üņØś Ļ│Āņ£Ā ļ░®ņé¼ņäĀ ļ»╝Ļ░ÉļÅäņŚÉ Ļ┤ĆĻ│äņŚåņØ┤ RITņØś ņ╣śļŻī ĒÜ©Ļ│╝ļź╝ ļåÆņØ┤ļŖö ļ░®ļ▓ĢņØĆ ļåÆņØĆ ļ░®ņé¼ņäĀļ¤ēņØä ņóģņ¢æņŚÉ ņĢłņĀäĒĢśĻ▓ī ņĀäļŗ¼ĒĢśļŖö Ļ░Ćņן ĒÜ©ņ£©ņĀüņØĖ ļ░®ļ▓ĢņØä Ļ░£ļ░£ĒĢśļŖö Ļ▓āņØ┤Ļ│Ā ļśÉĒĢ£ ņĢöņäĖĒż ņä▒ņן ļ░Å ņāØņĪ┤ņŚÉ ņżæņÜöĒĢ£ ņóģņ¢æ ĒĢŁņøÉņØä ļ░£ĻĄ┤ĒĢśĻ│Ā Ēæ£ņĀüņ£╝ļĪ£ ĒĢśļŖö Ļ▓āņØ┤ļŗż.
ļśÉĒĢ£ ņØśļ»Ė ņ׳ļŖö ņóģņ¢æ ĒØĪņłśņäĀļ¤ēņØä ņ¢╗ĻĖ░ ņ£äĒĢ┤ ļåÆņØĆ ĻĄŁņåī ļ░®ņé¼ļŖź ļåŹļÅäļź╝ ņĀäļŗ¼ĒĢĀ ņłś ņ׳ļŖö ļīĆņĢłņ£╝ļĪ£ ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤ļź╝ ņóģņ¢æ ņŻ╝ņ£äņŚÉ ĻĄŁņ¦ĆņĀüņ£╝ļĪ£ ņŻ╝ņé¼ĒĢśļŖö ļ░®ļ▓ĢņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼Ļ░Ć ņ¦äĒ¢ēļÉśņ¢┤ņĀĖ ņÖöĻ│Ā ļśÉ ļŗżļźĖ ņĀæĻĘ╝ļ▓Ģņ£╝ļĪ£ļŖö ņĢīĒīī ņ×ģņ×ÉņÖĆ Ļ░ÖņØ┤ ļ╣äĻĄÉņĀü ļåÆņØĆ ņāØļ¼╝ĒĢÖņĀü ĒÜ©Ļ│╝(relative biological effectiveness)ļź╝ Ļ░¢ļŖö ņ×ģņ×É ļ░®ņČ£(particle emission)ņØä ņé¼ņÜ®ĒĢśļŖö ļ░®ļ▓ĢņØ┤ ņŚ░ĻĄ¼ļÉśņ¢┤ņÖöļŗż. ņĢīĒīī ņ×ģņ×ÉļŖö ņ¦¦ņØĆ Ļ▓ĮļĪ£ļź╝ ļö░ļØ╝ ļ¦żņÜ░ ļåÆņØĆ ņŚÉļäłņ¦Ćļź╝ ņČĢņĀüĒĢĀ ņłś ņ׳ņ¢┤ņä£ ĻĖ░ņĪ┤ņŚÉ ļ¦ÄņØĆ ņŚ░ĻĄ¼Ļ░Ć ļÉ£ ļ▓ĀĒāĆ ņ×ģņ×Éļ│┤ļŗż ņäĀĒśĢ ņŚÉļäłņ¦Ć ņĀäļŗ¼ņØ┤ 2~3ļ░░ ļŹö ļåÆņØĆ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[16].
ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ RITņŚÉņä£ļŖö ņØ╝ļ░śņĀüņ£╝ļĪ£ ņĀüņāē Ļ│©ņłśņŚÉ ļīĆĒĢ£ ļÅģņä▒ ļĢīļ¼ĖņŚÉ ļŗ©ļÅģ ĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ ļ®┤ņŚŁņ╣śļŻī ļĢī ļ│┤ļŗż ĒĢŁņ▓┤ņØś ņ¢æņØä ļŗ©ņØ╝ ļśÉļŖö ļČäĒÜŹ Ēł¼ņŚ¼ Ļ│äĒÜŹņ£╝ļĪ£ ņåīļ¤ēņØä ņé¼ņÜ®ĒĢśņŚ¼ Ēł¼ņŚ¼ĒĢśĻ▓ī ļÉ£ļŗż. ļīĆņןņĢöņŚÉņä£ ĒĢŁ EGFR ĒĢŁņ▓┤ cetuximabņØä ņØ┤ņÜ®ĒĢ£ ļŗ©ļÅģ ĒĢŁņ▓┤ļ®┤ņŚŁņ╣śļŻīņŚÉņä£ ņ╣śļŻī ĻĖ░Ļ░ä ļÅÖņĢł ņ┤łĻĖ░ņŚÉ ņ▓┤Ēæ£ļ®┤ņĀüļŗ╣ 400 mg/m2(ļé©ņä▒ņØś Ļ▓ĮņÜ░ ĒÅēĻĘĀ 1.9 m2)ņØś ĒĢŁņ▓┤ļź╝ ņŻ╝ņé¼ĒĢśĻ│Ā ņØ┤ĒøäņŚÉ ļ¦żņŻ╝ 250 mg/m2ļĪ£ ņŻ╝ņé¼ĒĢ£ ļ░śļ®┤ņŚÉ[18], ĒĢŁ EGFR ĒĢŁņ▓┤ ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīņŚÉ ļīĆĒĢ£ ņ×äņāü ņŚ░ĻĄ¼ņŚÉņä£ļŖö 3.2~3.4 mgņØś ĒĢŁņ▓┤ļź╝ 3ĒÜī ļČäĒÜŹ ņŻ╝ņé¼ĒĢśņŚ¼ ļŗ©ļÅģ ĒĢŁņ▓┤ļ®┤ņŚŁņ╣śļŻīņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ 100ļ░░ ņØ┤ņāü ņĀüņØĆ ņ¢æņØä ņØ┤ņÜ®ĒĢśņśĆļŗż[19]. RITņŚÉ ņé¼ņÜ®ļÉśļŖö ĒĢŁņ▓┤ņØś ņ¢æņØ┤ ņĀüĻ▓ī ļÉśļ®┤ ĒśłļźśņØś Ļ░Éņåī, Ļ░äņ¦ł ņĢĢļĀźņØś ņ”ØĻ░Ć ļ░Å ņØ┤ņóģ ĒĢŁņøÉ ļ░£Ēśä ļō▒ņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ņ╣śļŻī ĒÜ©Ļ│╝Ļ░Ć ļ¢©ņ¢┤ņ¦ł ņłś ņ׳ļŖö ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ņ¢┤ņä£ ņØ┤ļź╝ ĻĘ╣ļ│ĄĒĢśĻĖ░ ņ£äĒĢśņŚ¼ ļīĆļ¤ēņØś ĒĢŁņ▓┤ļź╝ ļ©╝ņĀĆ Ēł¼ņŚ¼ĒĢśĻ│Ā ņØ┤ļ»Ė Ļ▓░ĒĢ®ļÉ£ ĒĢŁņ▓┤ņŚÉ Ļ▓░ĒĢ®ĒĢĀ ņłś ņ׳ļŖö ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ņåīļČäņ×É ņ╣śļŻīņĀ£ļź╝ Ēł¼ņŚ¼ĒĢśļŖö ļ░®ļ▓ĢļÅä ņŚ░ĻĄ¼Ļ░Ć ļÉśņ¢┤ņ¦ĆĻ│Ā ņ׳ļŗż[20].
EGFR ļ░£Ēśä ļæÉĻ▓ĮļČĆņĢöņŚÉņä£ 177Lu Ēæ£ņ¦Ć ĒĢŁ EGFR ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻī
CetuximabņØĆ chimeric anti-EGFR IgG1ņ£╝ļĪ£ ļåÆņØĆ ņ╣£ĒÖöļĀźņ£╝ļĪ£ EGFRņŚÉ Ļ▓░ĒĢ®ĒĢśĻ│Ā, ļŗżņÜ┤ ņŖżĒŖĖļ”╝ ņŗĀĒśĖ ņĀäļŗ¼ Ļ▓ĮļĪ£ņØś ĒÖ£ņä▒ĒÖöļź╝ ļ░®ņ¦ĆĒĢśļ®░ ĒĢŁņ▓┤ ņØśņĪ┤ņä▒ ņäĖĒż ļÅģņä▒ņØä ņ£ĀļÅäĒĢśļŖö ņ×æņÜ®ņ£╝ļĪ£ HNSCC ĒÖśņ×É ņ╣śļŻīļź╝ ņ£äĒĢ┤ FDAņŚÉ ņØśĒĢ┤ ņŖ╣ņØĖļÉśņŚłļŗż. ĒĢśņ¦Ćļ¦ī cetuximabņØä ļŗ©ņØ╝ ņĢĮņĀ£ļĪ£ ņé¼ņÜ®ĒĢśļŖö Ļ▓ĮņÜ░ ļé┤ņØĖņä▒ ļ░Å Ēøäņ▓£ņä▒ ņĢĮļ¼╝ ļé┤ņä▒ņ£╝ļĪ£ ņØĖĒĢśņŚ¼ EGFR Ēæ£ņĀü ņ╣śļŻīļ▓ĢņŚÉ ļīĆĒĢ£ Ļ▓░Ļ│╝Ļ░Ć ņśłņāüĻ│╝ļŖö ļŗ¼ļ”¼ ņóŗņ¦Ć ņĢŖņØĆ Ļ▓āņØ┤ ĒśäņŗżņØ┤ļŗż. ļö░ļØ╝ņä£ HNSCC ĒÖśņ×ÉņŚÉņä£ ņĢĮļ¼╝ ņĀĆĒĢŁņä▒Ļ│╝ ņĀ£ĒĢ£ļÉ£ ļ░śņØæļźĀņØä ĻĘ╣ļ│ĄĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ļīĆņ▓┤ ņ╣śļŻīļ▓ĢņØ┤ ĒĢäņÜöĒĢśļŗż. ļ╣äļĪØ ļŗżņ¢æĒĢ£ ņ¢ĄņĀ£ņĀ£ņŚÉ ņØśĒĢ£ EGFR ņ¢ĄņĀ£Ļ░Ć Ļ│ĀĒśĢ ņóģņ¢æņŚÉņä£ ņ╣śņ£ĀļÉśņ¦ĆļŖö ņĢŖņØäņ¦ĆļØ╝ļÅä, ļ░®ņé¼ņäĀ ņÜöļ▓ĢĻ│╝ņØś ļ│æņÜ® ņĀæĻĘ╝ņØĆ ĻĄŁņåī ņóģņ¢æ ņĪ░ņĀłņØä ņĀüļŗ╣Ē׳ Ļ░£ņäĀĒĢĀ ņłś ņ׳ļŖö Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż[21,22].
ņĄ£ĻĘ╝ ņŚ¼ļ¤¼ ņŚ░ĻĄ¼ņŚÉņä£ ļ®┤ņŚŁ ņ¢æņĀäņ×Éļ░®ņČ£ļŗ©ņĖĄņ┤¼ņśü(immuno-PET) ņĀ£ņĀ£ļĪ£ ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁ EGFR ĒĢŁņ▓┤ļź╝ ņé¼ņÜ®ĒĢśņŚ¼ Ēæ£ņĀü ļ░£ĒśäņØś ņĀĢĒÖĢĒĢ£ ņĀĢļ¤ēĒÖö ļ░Å ļ░®ņé¼ļ®┤ņŚŁņÜöļ▓ĢņĀ£ļĪ£ņä£ņØś ņ╣śļŻī ĒÜ©ļŖźņØä ņ”ØļīĆĒĢĀ ņłś ņ׳ņØīņØä ļ│┤ņŚ¼ ņŻ╝ņŚłļŗż[8].
Ēśäņ×¼Ļ╣īņ¦Ć HNSCC ļ¬©ļŹĖņØś RITņŚÉ ņé¼ņÜ®ļÉśļŖö Ļ░Ćņן ņØ╝ļ░śņĀüņØĖ ļ░®ņé¼ņä▒ ĒĢĄņóģņØĆ 90YņÖĆ 177Lutetium(177Lu)ņØ┤ļŗż(Table 2). ņØ┤ ļæÉ Ļ░Ćņ¦Ć ļ░®ņé¼ņä▒ ĒĢĄņóģņØĆ RITņØś ĒÜ©Ļ│╝ņŚÉ ĻĖ░ņŚ¼ĒĢśļŖö ņżæņÜöĒĢ£ ņÜöņåīņØĖ ļ░®ņČ£ ĒŖ╣ņä▒Ļ│╝ ĒÖöĒĢÖņĀü ņĢłņĀĢņä▒ņØś ņ░©ņØ┤ ļĢīļ¼ĖņŚÉ Ļ░üĻ░üņØś ņןļŗ©ņĀÉņØ┤ ņ׳ļŗż. 90YņØś ņØ┤ņĀÉņØĆ ņóģņ¢æņŚÉ ļŹö ļåÆņØĆ ļ▓ĀĒāĆ ņŚÉļäłņ¦Ćļź╝ ņĀäļŗ¼ĒĢ£ļŗżļŖö Ļ▓ā(2.3 MeV vs. 177LuņØś Ļ▓ĮņÜ░ 0.61 MeV)Ļ│╝ ļ░®ņČ£ļÉ£ ņŚÉļäłņ¦ĆņØś 90% ņØ┤ņāüņØ┤ ĒØĪņłśļÉśļŖö ĒÅēĻĘĀ Ļ╣ŖņØ┤Ļ░Ć ļŹö Ļ╣Ŗļŗż(5.3 mm vs. 177LuņØś Ļ▓ĮņÜ░ 0.8 mm). ņØ┤ļ¤¼ĒĢ£ ĒŖ╣ņä▒ņØĆ Ēæ£ņĀü ņäĖĒżņÖĆ ņØ┤ņøā ņäĖĒż ļ¬©ļæÉļź╝ ņŻĮņØ┤ļŖö ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤ņØś ļŖźļĀźņØä Ē¢źņāüņŗ£Ēéżļ®░, ņØ┤Ļ▓āņØĆ ļČĆĒö╝Ļ░Ć Ēü¼Ļ▒░ļéś ĒśłĻ┤ĆņØ┤ ĒśĢņä▒ļÉśņ¦Ć ņĢŖņØĆ ņóģņ¢æņØ┤ ņ׳ņØä ļĢī ĒŖ╣Ē׳ ņżæņÜöĒĢ£ Ļ▓āņ£╝ļĪ£ ņĢīļĀżņĀĖ ņ׳ļŗż. ļśÉĒĢ£ 90YļŖö ņł£ņłś ļ▓ĀĒāĆ ļ░®ņČ£ ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ ņ×ģņøÉ, Ļ▓®ļ”¼ ļśÉļŖö ņ░©ĒÅÉĻ░Ć ĒĢäņÜöĒĢśņ¦Ć ņĢŖņ£╝ļ®░ ĒÖśņ×ÉļŖö ņÖĖļל ĒÖśņ×ÉļĪ£ ņ╣śļŻīļ░øņØä ņłś ņ׳ļŖö ņןņĀÉņØ┤ ņ׳ļŗż. ĒĢśņ¦Ćļ¦ī ļ¦żņÜ░ ļ╣äņŗĖĻ│Ā Ļ░Éļ¦łņäĀņØä ļ░®ņČ£ĒĢśņ¦Ć ņĢŖņ£╝ļ»ĆļĪ£ ņØ┤ļ»Ėņ¦ĆņŚÉ ņé¼ņÜ®ĒĢĀ ņłś ņŚåļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŗż[23].
177LuņØś ņןņĀÉņØĆ 90YņÖĆ ļ╣äĻĄÉĒĢśņŚ¼ ņāüņŚģņĀüņ£╝ļĪ£ ņØ┤ņÜ® Ļ░ĆļŖźĒĢśĻ│Ā ĒĢŁņ▓┤ņŚÉ ņēĮĻ▓ī ņĀæĒĢ®ļÉśļ®░ ņśżļ×£ ņŚŁņé¼ļź╝ Ļ░Ćņ¦ĆĻ│Ā ņ׳ļŗżļŖö ņĀÉņØ┤Ļ│Ā ņØśļŻīņĀü ņé¼ņÜ®ņŚÉ ņĢłņĀäĒĢśĻ│Ā ļśÉĒĢ£ Ļ░Éļ¦ł ņŚÉļäłņ¦Ćļź╝ ļ░®ņČ£ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ ņØ┤ļ»Ėņ¦ĆņŚÉ ņé¼ņÜ®ĒĢĀ ņłś ņ׳ļŗżļŖö ņĀÉņØ┤ ņ£Āļ”¼ĒĢśļŗż. ĒĢśņ¦Ćļ¦ī 177LuņØś ņé¼ņÜ®ņØĆ ņ░©ĒÅÉļź╝ ĒåĄĒĢ£ ņ×ģņøÉņØ┤ ĒĢäņÜöĒĢśĻ│Ā ņøÉĻ▒░ļ”¼ ĻĖ░Ļ┤ĆņŚÉ ļ░®ņé¼ņäĀņØ┤ ņĪ░ņé¼ļÉĀ ņłś ņ׳ļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŗż. Ēæ£ņĀüĒÖöļÉ£ ļČäņ×ÉņŚÉ ĻĖłņåŹ ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīļź╝ ļČĆņ░®ņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņØ╝ļ░śņĀüņ£╝ļĪ£ ņØ┤ņøÉņä▒ Ēé¼ļĀłņØ┤ĒŖĖ(bifunctional chelate, BFC)Ļ░Ć ĒĢäņÜöĒĢśļŗż. Ēśäņ×¼ ņØ┤ņÜ® Ļ░ĆļŖźĒĢ£ BFCļŖö ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒÖöĒĢÖ ļśÉļŖö ņāØļ”¼ĒĢÖņĀü ņĢłņĀĢņä▒ņŚÉ ņØśĒĢ┤ ņĀ£ĒĢ£ņĀÉņØ┤ ņ׳ļŖöļŹ░ 3, 6, 9, 15-tetraazabicyclo [9.3.1] pentadeca-1(15), 11, 13 triene 3, 5, 9-triacetic acid(PCTA)ļŖö 1, 4, 7, 10-tetraazacyclododecane-1, 4, 7, 10-tetraacetic acid(DOTA)ņŚÉ ļ╣äĒĢ┤ņä£ ņāüļīĆņĀüņ£╝ļĪ£ ņÜ░ņłśĒĢ£ ļ░śņØæņåŹļÅäļź╝ ļ│┤ņØ┤ļ®░ 177LuĻ│╝ņØś ņĀæĒĢ®ņ▓┤ ĒśĢņä▒ņŚÉ ņ׳ņ¢┤ņä£ļÅä ņŗżņś©ņŚÉņä£ 5ļČä ļ»Ėļ¦īņŚÉņä£ 98%ņØ┤ņāüņØś ļ░®ņé¼ĒÖöĒĢÖņĀü purityļź╝ ļ│┤ņśĆļŗż. ļśÉĒĢ£ PCTAļŖö pH 2~9 ļ▓öņ£äņŚÉņä£ ĒÜ©ņ£©ņĀü ņĀæĒĢ®ņØ┤ ļÉśļ®░ ļÅÖļ¼╝ņØś ņŗĀņןņŚÉņä£ņØś Ēü┤ļ”¼ņ¢┤ļ¤░ņŖżļÅä 64Cu-DOTAļ│┤ļŗż 64Cu-PCTAĻ░Ć ļ╣Āļź┤ĻĖ░ ļĢīļ¼ĖņŚÉ, ņØ┤ļ¤░ ņŚ¼ļ¤¼ ņןņĀÉ ļō▒ņ£╝ļĪ£ 177Lu-PCTA-cetuximabņØ┤ ļæÉĻ▓ĮļČĆņĢö RITņŚÉ Ļ░Ćņן ņĀüĒĢ®ĒĢ£ ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤ ņżæņŚÉ ĒĢśļéśĻ░Ć ļÉĀ ņłś ņ׳ļŗż[25].
Ļ░£ņØĖ ļ¦×ņČżĒśĢ ņ╣śļŻīļĪ£ņä£ ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻī ļ░Å Immune-PETņØś ņŚŁĒĢĀ
ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīņŚÉ ņé¼ņÜ®ļÉśļŖö ļ░®ņé¼ņä▒ Ēæ£ņ¦Ć ĒĢŁņ▓┤ņŚÉņä£ ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīļź╝ ņśüņāü ĒÜŹļōØņØ┤ Ļ░ĆļŖźĒĢ£ Ļ░Éļ¦łņäĀ ļ░®ņČ£ ļÅÖņ£äņøÉņåīļĪ£ ņ╣śĒÖśĒĢ┤ņä£ ņĀæĒĢ®ņØä ĒĢśĻ▓ī ļÉśļ®┤ ļ®┤ņŚŁ ņ¢æņĀäņ×Éļ░®ņČ£ļŗ©ņĖĄņ┤¼ņśü(immuno-PET)ņØä ņØ┤ņÜ®ĒĢĀ ņłś ņ׳Ļ▓ī ļÉ£ļŗż. Immuno-PETņØä ņØ┤ņÜ®ĒĢśĻ▓ī ļÉśļ®┤ ņĀäņŗĀņŚÉņä£ ņóģņ¢æņŚÉņä£ ļ░£ĒśäļÉśļŖö Ēæ£ņĀü ĒĢŁņøÉļōżņØś ļ░£ĒśäņØä ņŗ£Ļ░üĒÖöĒĢĀ ņłś ņ׳ĻĖ░ ļĢīļ¼ĖņŚÉ ņ╣©ņŖĄņĀüņØĖ ļŗ©ņØ╝ ņāØĻ▓ĆņØä ĒåĄĒĢ£ ļ®┤ņŚŁņĪ░ņ¦üĒÖöĒĢÖĻ▓Ćņé¼ņÖĆļŖö ļŗ¼ļ”¼ Ēæ£ņĀü ļČäņ×ÉņŚÉ ļ╣äņ╣©ņŖĄņĀüņØ┤ļ®░ ņĀĢļ¤ēņĀüņØĖ ņĀäņŗĀ ņØ┤ļ»Ėņ¦Ćļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņ¦äļŗ© ļ░Å ļ│æĻĖ░ ņäżņĀĢņØä ĒĢĀ ļĢī ļŹö ĒżĻ┤äņĀüņØĖ ņĀĢļ│┤ļź╝ ņ¢╗ņØä ņłś ņ׳ļŗż. ļ│æļ│ĆņŚÉņä£ņØś ļ░£Ēśä ņ¢æņāüņØä ļČäņäØĒĢśņŚ¼ ņĪ░ņ¦üņØś ņØ┤ņ¦łņä▒(heterogeneity) ņŚ¼ļČĆļÅä ĒÅēĻ░ĆĒĢĀ ņłś ņ׳ļŗż. ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīņÖĆ Ļ░ÖņØĆ Ēæ£ņĀü ņ╣śļŻīņŚÉ ņ׳ņ¢┤ņä£ Ēæ£ņĀü ĒĢŁņøÉ ļ░£ĒśäņØś ņĀĢĒÖĢĒĢ£ ņĀĢļ¤ēĒÖöĻ░Ć Ļ░ĆļŖźĒĢśņŚ¼ ĒÖśņ×ÉņØś ņ╣śļŻī ņĀüĒĢ®ņä▒ņØä ĒīÉļŗ©ĒĢśņŚ¼ ņ╣śļŻī ĒÜ©ļŖźņØä ņ”ØļīĆņŗ£Ēé¼ ņłś ņ׳ļŗż. ņĀüņĀłĒĢ£ ĒÖśņ×ÉĻ░Ć ņäĀĒāØļÉ£ļŗżļ®┤ ņĢĮļ¼╝ Ēł¼ņŚ¼ļ¤ē ļ░Å ņØ╝ņĀĢņØä ņĄ£ņĀüĒÖöĒĢśļŖöļŹ░ ļÅäņøĆņØä ļ░øņØä ņłś ņ׳ļŗż. ņĢĮļ¼╝ĒĢÖņĀüņØĖ ĒÅēĻ░ĆļĪ£ņŹ© Ēæ£ņĀüņ╣śļŻīņĀ£ņØś ļ░śņØæ ļ░Å Ēæ£ņĀü ņ¢ĄņĀ£(off-target) ļ░śņØæņŚÉ ļīĆĒĢ£ ļ¬©ļŗłĒä░ļ¦üņØä ĒĢĀ ņłś ņ׳ļŗż.
ņłśļ¬ģņØ┤ ĻĖ┤ ņ¢æņĀäņ×É ļ░®ņČ£ ļ¼╝ņ¦łņØĖ 124IņÖĆ 89zirconium(89Zr)ņØĆ ņåÉņāüļÉśņ¦Ć ņĢŖņØĆ ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ņÖĆ ĒĢ©Ļ╗ś ņé¼ņÜ®ĒĢĀ ļĢī immune-PETņŚÉ ĒŖ╣Ē׳ ņĀüĒĢ®ĒĢśļŗż[26].
ļŗżņ¢æĒĢ£ ņØ┤ņóģ ņØ┤ņŗØ ļ¬©ļŹĖ[27-30]ņŚÉņä£ ņŚ¼ļ¤¼ Ļ░Ćņ¦Ć 124I Ēæ£ņ¦Ć ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ ĻĄ¼ņĪ░ļź╝ ņé¼ņÜ®ĒĢśņŚ¼ ļø░ņ¢┤ļé£ ņŗ£Ļ░üĒÖö ļ░Å ņĀĢļ¤ēĒÖö Ļ▓░Ļ│╝ļź╝ ņ¢╗ņŚłļŗż. 124I Ēæ£ņ¦ĆļÉ£ ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ņØś PET ņśüņāüņØĆ 131Iļź╝ ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīļĪ£ ņØ┤ņÜ®ĒĢśļŖö RIT ņØ┤ņĀäņØś ņ╣śļŻī ņĀüĒĢ®ņä▒ ĒÅēĻ░ĆņŚÉ ņ£ĀņÜ®ĒĢ£ļŹ░ 124I ļ░Å 131IņØ┤ Ēæ£ņ¦ĆļÉ£ ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤Ļ░Ć ņä£ļĪ£ ņל ņØ╝ņ╣śļÉ£ ņāØņ▓┤ ļČäĒżļź╝ ļéśĒāĆļé┤ņĢ╝ Ļ░ĆļŖźĒĢśļ®░, ņØ┤ļŖö ņל Ēæ£ņżĆĒÖöļÉ£ ņÜöņśżļō£ĒÖö ļ░®ļ▓Ģ[31]ņØä ĒåĄĒĢ┤ ļŗ¼ņä▒ļÉĀ ņłś ņ׳ļŗż.
ņĄ£ĻĘ╝ ļæÉ Ļ░Ćņ¦Ć ņ×äņāüņĀü ņĀüņÜ®ņØ┤ ņŻ╝ļ¬®ņØä ļüīĻ│Ā ņ׳ļŗż. Jayson ļō▒[32]ņØĆ ļŗżņ¢æĒĢ£ ņ¦äĒ¢ēņä▒ Ļ│ĀĒśĢ ņóģņ¢æņØ┤ ņ׳ļŖö 12ļ¬ģņØś ĒÖśņ×ÉņŚÉņä£ PET ņśüņāü Ļ▓Ćņé¼ļź╝ ņłśĒ¢ēĒĢśĻĖ░ ņ£äĒĢ┤ vascular endothelial growth factor(VEGF)121Ļ│╝ VEGF165ņŚÉ Ļ▓░ĒĢ®ĒĢśļŖö ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ņØĖ 124IHuMV833ņØä ļŗżņ¢æĒĢśĻ▓ī ņé¼ņÜ®Ē¢łļŗż. ĒĢŁņ▓┤ ļČäĒżņÖĆ Ēü┤ļ”¼ņ¢┤ļ¤░ņŖżļŖö ĒÖśņ×É Ļ░ä ļ░Å Ļ░£ņ▓┤ Ļ░ä, ņóģņ¢æ ļé┤ņÖĖņŚÉņä£ ĒśäņĀĆĒ׳ ņØ┤ņ¦łņĀüņØ┤ņŚłļŗż. ņØ┤ļ¤¼ĒĢ£ ņ░©ņØ┤ļź╝ ĒåĄĒĢ┤ņä£ ĒĢŁ VEGF ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ ņ╣śļŻī ņŗ£ņŚÉ Ēæ£ņĀüņØś ļŗżņ¢æņä▒ņØ┤ ņ׳ņØīņØä ļ»Ėļ”¼ ĒÅēĻ░ĆĒĢĀ ņłś ņ׳ļŗżļŖö ņØśļ»Ėņ׳ļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ņŚłļŗż.
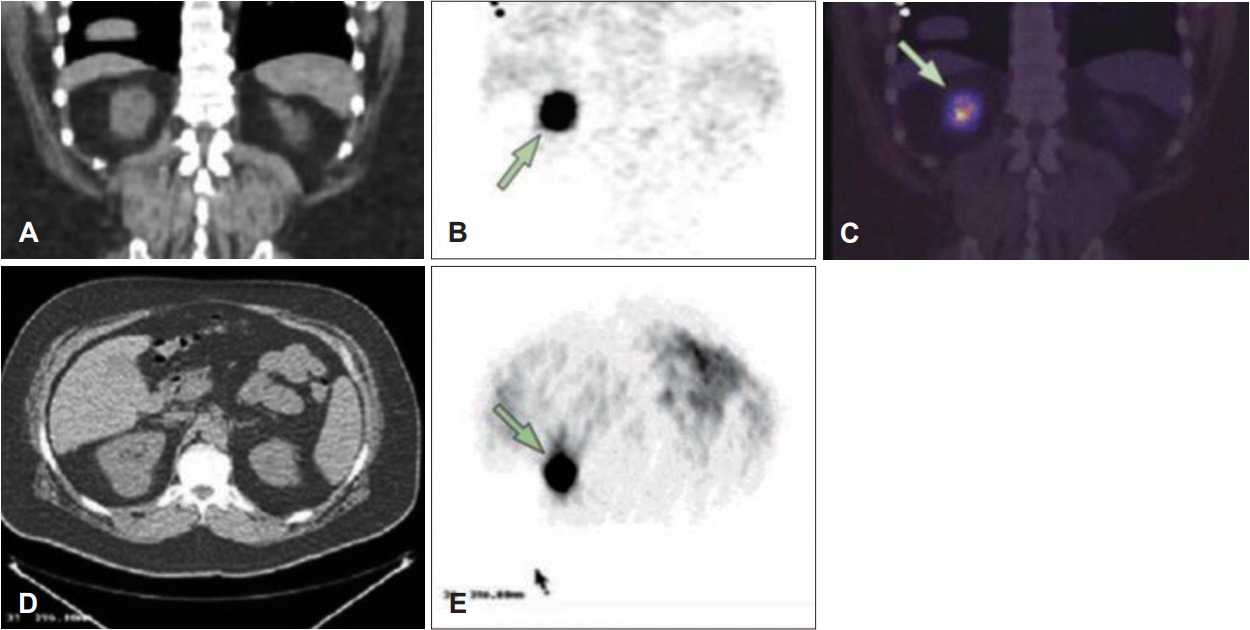
ļŗżļźĖ ņ×äņāü ņĀüņÜ®ņŚÉņä£, 124I Ēæ£ņ¦Ć immuno-PETļŖö ņŗĀņןņĢöņØś ņāØņ▓┤ ļé┤ ĒöäļĪ£ĒīīņØ╝ļ¦üņŚÉ ņé¼ņÜ®ļÉśņŚłļŗż. Divgi ļō▒[33]ņØĆ 124I Ēæ£ņ¦Ć c-monoclonal antibodies(mAb) G250ņØä ņé¼ņÜ®ĒĢśņŚ¼ ņÖĖĻ│╝ņĀü ņóģņ¢æ ņĀłņĀ£ņłĀņØä ļ░øņØä ņśłņĀĢņØĖ 25ļ¬ģņØś ĒÖśņ×ÉņŚÉņä£ Ēł¼ļ¬ģņäĖĒż ņŗĀņןņĢö(clear cell renal cell carcinoma)ņØś ņĪ┤ņ×¼ļź╝ ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż. G250ņØĆ carbonic anhydrase-IXņŚÉ ļīĆĒĢŁĒĢśņŚ¼ Ēł¼ļ¬ģņäĖĒż ņŗĀņןņĢöņŚÉņä£ Ļ│╝ļ░£ĒśäļÉ£ļŗż(Fig. 2). 16Ļ░£ņØś Ēł¼ļ¬ģņäĖĒżņĢö ņżæ 15Ļ░£Ļ░Ć immuno-PETņŚÉ ņØśĒĢ┤ ņĀĢĒÖĢĒ׳ ĒÖĢņØĖļÉśņŚłĻ│Ā, ļéśļ©Ėņ¦Ć 9Ļ░£ļŖö ļ╣äĒł¼ļ¬ģņäĖĒżņĢöņ£╝ļĪ£ immuno-PET Ļ▓Ćņé¼ņŚÉņä£ ņØīņä▒ņØ┤ņŚłļŗż. ņØ┤ ņŚ░ĻĄ¼ļŖö ĒŖ╣ņĀĢ ĒöäļĪ£ļĖīļź╝ ņØ┤ņÜ®ĒĢ£ ļČäņ×É ņØ┤ļ»Ėņ¦ĢņØ┤ ņ¢┤ļ¢╗Ļ▓ī Ļ░£ņØĖ ļ¦×ņČżņØśĒĢÖņŚÉ ĻĖ░ņŚ¼ĒĢĀ ņłś ņ׳ļŖöņ¦Ćļź╝ ļ│┤ņŚ¼ņŻ╝ņŚłļŗż.
ļśÉ ļŗżļźĖ ņłśļ¬ģņØ┤ ĻĖ┤ ņ¢æņĀäņ×É ļ░®ņé¼ņ▓┤ 89ZrņØ┤ immuno-PETņŚÉ ņĀüņÜ®ļÉ£ ņØ┤ĒøäļĪ£, cetuximab [34], ibritumomab tiuxetan [35], rituximab, bevacizumab [36], trastuzumab [37] ļō▒ņØś ļŗżņ¢æĒĢ£ ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ņŚÉ Ēæ£ņ¦ĆļÉśņ¢┤ Ļ░üĻ░üņØś ĒĢŁņ▓┤ņŚÉ ļ»╝Ļ░ÉĒĢ£ ņóģņ¢æ Ļ▓ĆņČ£ ļ░Å immuno-PETļź╝ ĒåĄĒĢ£ ņĀĢĒÖĢĒĢ£ ņĀĢļ¤ēĒÖöĻ░Ć Ļ░ĆļŖźĒĢ©ņØ┤ ņ×ģņ”ØļÉśņŚłĻ│Ā, 89Zr Ēæ£ņ¦Ć ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢśļŖö immuno-PETļŖö 90Y ļśÉļŖö 177Lu Ēæ£ņ¦Ć ļŗ©ņØ╝Ēü┤ļĪĀĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ RIT ņ╣śļŻī ņĀäņŚÉ ņāØņ▓┤ļČäĒżļź╝ ņśłņĖĪĒĢśļŖö ļŹ░ ņ£ĀņÜ®ĒĢ£ Ļ▓āņ£╝ļĪ£ ļ░ØĒśĆņĪīļŗż[34,37,38]. ņĄ£ĻĘ╝ņŚÉ VEGF [32,39] ļ░Å VEGF receptor(VEGFR) [40]ņØä Ēæ£ņĀüņ£╝ļĪ£ ĒĢśļŖö immuno-PET ņØ┤ļ»Ėņ¦Ģ ĒöäļĪ£ļĖīĻ░Ć Ļ░£ļ░£ļÉśņ¢┤ņä£ ļŗżņ¢æĒĢśĻ▓ī ņ×äņāüņĀüņ£╝ļĪ£ ņĀüņÜ®ņØ┤ ļÉśĻ│Ā ņ׳ļŗż.
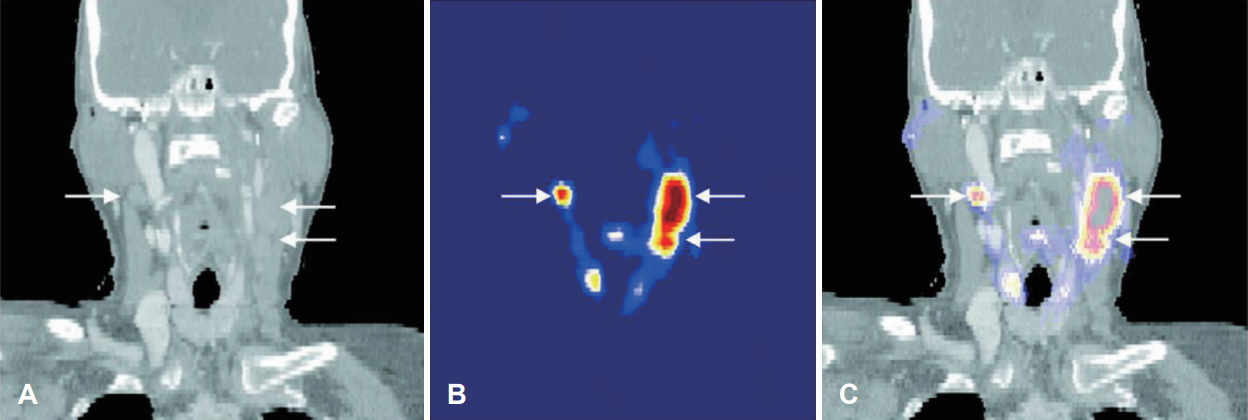
ļæÉĻ▓ĮļČĆ ĒÄĖĒÅēņāüĒö╝ņäĖĒżņĢö(HNSCC) ĒÖśņ×ÉņŚÉņä£ 89Zr Ēæ£ņ¦Ć c-mAb U36ņØä ņØ┤ņÜ®ĒĢ£ immuno-PETņØś ņ¦äļŗ©ņĀü Ļ░Ćņ╣śļź╝ ĒÅēĻ░ĆĒĢśļŖö ņĄ£ĻĘ╝ ņŚ░ĻĄ¼ņŚÉņä£[41,42] 20ļ¬ģņØś ĒÖśņ×ÉļŖö ņøÉļ░£ ņóģņ¢æ ļ░Å ļŗ©ņĖĪ ļśÉļŖö ņ¢æņĖĪ ļ¬® ņĀłņĀ£ņłĀņØä ņŗ£Ē¢ē ņĀäņŚÉ CT, MRIņÖĆ 89Zr Ēæ£ņ¦Ćc-mAb U36 immuno-PETĻ▓Ćņé¼ļź╝ ņŗ£Ē¢ē ļ░øņĢśļŗż. Immuno-PETņŚÉņä£ļŖö ļ¬©ļōĀ ņøÉļ░£ ļČĆņ£ä ņóģņ¢æ(n=17)Ļ│╝ 25Ļ░£ņØś ļ”╝ĒöäņĀł ņĀäņØ┤ ņżæ 18Ļ░£ņŚÉņä£ ņ¢æņä▒ņ£╝ļĪ£ ļ░£ĒśäļÉśņŚłļŗż(Fig. 3). ļłäļØĮļÉ£ ļ”╝ĒöäņĀłņØĖ Ļ▓ĮņÜ░ļŖö Ēü¼ĻĖ░Ļ░Ć ļ╣äĻĄÉņĀü ņ×æĻ▒░ļéś ņĀäņØ┤ļÉ£ ļ”╝ĒöäņĀł ļé┤ņŚÉņä£ ņĢöņäĖĒżņØś ļ╣äņ£©ņØ┤ ņĀüņØĆ Ļ▓ĮņÜ░ņśĆļŗż. Ļ▓ĮļČĆ ļĀłļ▓© ļ│äļĪ£ ļČäņäØĒĢśņśĆņØä ļĢī, ņ┤ēņ¦ä, CT/MRI, FDG PET Ļ▓Ćņé¼ņØś ļ»╝Ļ░ÉļÅä(sensitivity)ļŖö Ļ░üĻ░ü 54%, 77%, 62%ņśĆĻ│Ā 89Zr-immuno PETļŖö 85%ņśĆļŗż. ĒŖ╣ņØ┤ļÅä(specificity)ņŚÉņä£ļŖö ļ¬©ļæÉ 100%ļź╝ ļ│┤ņśĆļŗż. Ļ▓Ćņé¼ņØś ņĀĢĒÖĢļÅä(accuracy)ļŖö Ļ░üĻ░ü 85%, 93%, 88%, 95%ļź╝ ļ│┤ņśĆļŗż. ņØ┤ Ļ▓░Ļ│╝ļź╝ ĒåĄĒĢ┤ņä£ 89Zr Ēæ£ņ¦Ć c-mAb U36 immuno-PETņØ┤ HNSCCņŚÉņä£ ļ”╝ĒöäņĀł ņĀäņØ┤ļź╝ ņ¦äļŗ©ĒĢśļŖöļŹ░ ņ׳ņ¢┤ņä£ CT, MRIļ┐Éļ¦ī ņĢäļŗłļØ╝ PET-CT Ļ▓Ćņé¼ļź╝ ļ│┤ņÖäĒĢ┤ņżä ņłś ņ׳ļŖö Ļ▓Ćņé¼Ļ░Ć ļÉĀ ņłś ņ׳ņØīņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż.
Ļ▓░ ļĪĀ
ļæÉĻ▓ĮļČĆņĢöņØä ĒżĒĢ©ĒĢ£ Ļ│ĀĒśĢ ņóģņ¢æņŚÉņä£ņØś ļ░®ņé¼ļ®┤ņŚŁņÜöļ▓ĢņØĆ ĒśłņĢĪĒĢÖņĀü ņĢģņä▒ ņóģņ¢æņØś ņ╣śļŻīņŚÉņä£ ņØśļ»Ė ņ׳ļŖö ņä▒Ļ│ĄļźĀņØä ļ│┤ņśĆņØīņŚÉļÅä ļČłĻĄ¼ĒĢśĻ│Ā ņŚ¼ņĀäĒ׳ ļÅäņĀä Ļ│╝ņĀ£ļĪ£ ļé©ņĢä ņ׳ļŗż. ļ░®ņé¼ņä▒ ļÅÖņ£äņøÉņåīĻ░Ć Ēæ£ņ¦ĆļÉśņ¦Ć ņĢŖņØĆ ņŚ¼ļ¤¼ ĒĢŁņ▓┤ļź╝ ņØ┤ņÜ®ĒĢ£ ļŗ©ļÅģļ®┤ņŚŁņ╣śļŻīļŖö ņóģņ¢æ ņä▒ņן ņŗĀĒśĖ ņĀäļŗ¼ Ļ▓ĮļĪ£ļź╝ ņĪ░ņĀłĒĢśļŖö ņóģņ¢æ ņäĖĒż ĒĢŁņøÉņØä Ēæ£ņĀüņ£╝ļĪ£ ĒĢśņŚ¼ ņØ╝ļČĆ ņä▒Ļ│ĄņĀüņØĖ Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝Ļ│Ā ņ׳ņ¦Ćļ¦ī ņ╣śļŻī Ļ▓░Ļ│╝ņŚÉ ņ׳ņ¢┤ņä£ļŖö ņŚ¼ņĀäĒ׳ ņĀ£ĒĢ£ņĀÉņØ┤ ņĪ┤ņ×¼ĒĢ£ļŗż. ņØ┤ļ¤░ ņĀÉņŚÉņä£ ļ░®ņé¼ļ®┤ņŚŁņ╣śļŻīĻ░Ć ļŗ©ļÅģļ®┤ņŚŁņ╣śļŻīņØś ĒĢ£Ļ│äļź╝ ĻĘ╣ļ│ĄĒĢśĻĖ░ ņ£äĒĢ£ ņ╣śļŻīņĀü ļīĆņĢłņØ┤ ļÉĀ ņłś ņ׳ņØä Ļ▓āņ£╝ļĪ£ ĻĖ░ļīĆļÉśļ®░ ļśÉĒĢ£ immuno-PETņØś ņØ┤ņÜ®ņ£╝ļĪ£ Ļ░£ņØĖ ļ¦×ņČżĒśĢ ņ╣śļŻīņØś ĒÜ©Ļ│╝ļź╝ ņ”ØļīĆņŗ£Ēé¼ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.