고삭신경 신경초종 1예
A Case of Schwannoma of the Chorda Tympani Nerve
Article information
Trans Abstract
Schwannoma is a benign nerve sheath tumor composed of schwann cells. Most schwannoma arising in the middle ear are facial nerve schwannoma. In very rare occasions, schwannoma of the middle ear can arise from chorda tympani nerve. Hearing loss and tinnitus are the most common symptoms of patients with schwannoma of chorda tympani nerve and it can be treated by surgical excision. Recently, we treated a male patient with schwannoma of the chorda tympani nerve. This is the first case of schwannoma of the chorda tympani nerve reported in Korea. Herein, we present the case in detail with a review of the related literature.
서 론
신경초종(schwannoma)은 신경초세포(schwann cell)에서 기원하는 양성 종양으로 인체의 말초신경이 있는 모든 부위에서 발생할 수 있다[1]. 인체에서 발생하는 전체 신경초종의 약 25%가 두경부에서 발생하며 중이에서도 드물게 발생한다. 중이에서 발생하는 신경초종은 주로 안면신경에서 기원하며 고삭신경에서 기원하는 신경초종은 매우 드문 것으로 알려져 있다[1,2]. 고삭신경 기원의 신경초종은 현재까지 해외에서 드물게 보고되었고[3-5]. 국내에서는 보고된 적이 없다. 고삭신경은 미각의 전달 통로이지만, 지금까지 보고된 고삭신경 기원의 신경초종 증례 중에서 미각 이상을 증상으로 호소한 증례는 없었고[2,3] 대부분의 증례는 전도성 난청과 이명이 주 증상으로 나타났다(Table 1).
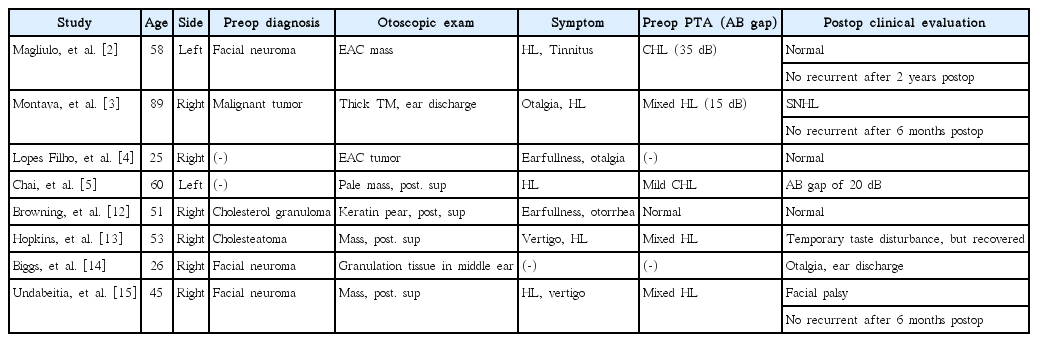
Characteristic of schwannoma of chorda tympanic nerve
저자들은 최근 고삭신경에서 기원한 신경초종을 경험하였다. 국내에서 첫 발견이라는 의의뿐 아니라, 본 질환에 대한 진단 과정 및 수술방법, 감별 진단을 위한 술전 제반 검사의 정보를 알리고자 본 증례를 보고하는 바이다.
증 례
52세 남자 환자가 내원 1개월 전부터 발생한 우측의 청력 저하 및 이명으로 동아대학교병원 이비인후과 외래를 방문하였다. 어지럼, 이루, 이통의 이과적 증상은 없었고 미각 이상은 호소하지 않았다. 이내시경검사에서 우측 고막의 후상방에 전체 고막 면적의 약 1/4을 차지하는 타원 모양의 백색 종물이 발견되었다(Fig. 1). 순음청력검사에서 우측 기도청력 20 dB HL(6분법 평균), 골도청력 5 dB HL(6분법 평균)의 전도성 난청 소견을 보였다.
Otoscopic finding that shows a middle ear mass at posterosuperior quadrant of right tympanic membrane.
측두골 전산화단층촬영에서 우측 프루사키 공간(prussak’s space)을 침범하고 침골의 장돌기를 파괴한 연조직 음영의 병변이 관찰되었다(Fig. 2). 이 병변은 내이도 자기공명영상의 T1강조영상과 T2강조영상에서 뇌실질과 같은 신호강도를 보였고, 확산 강조영상에서 높은 신호강도를 보였으며, 조영증강영상에서 조영 증강이 되었다(Fig. 3). 이러한 영상 소견을 바탕으로 이 병변을 비진주종성 신생물로 예상하고 시험적 고실 개방술을 시행하였다.

Axial (A) and coronal (B) images of temporal bone computed tomography showing a mass lesion(arrow) that occupies right prussak’s space. Long process of incus is destroyed by the mass.

Magnetic resonance images. The lesion demonstrates isosignal intensity on T1WI and T2WI, and shows high signal intensity on DWI and contrast enhanced image. T1WI: T1-weighted image, T2WI: T2-weighted image, DWI: diffusion weighted image.
후이개 피부 절개를 가한 후 고실외이도 피판을 거상하였다. 이때 중이강 후상부에서 고삭신경 기원의 종물이 발견되었다(Fig. 4A). 추골은 정상이었고 침골은 장돌기가 종물에 의해 파괴되어 있었다. 종물이 등골을 완전히 덮고 있어서 등골의 상태는 확인할 수 없었다. 이 상태에서 종물 제거를 시도할 경우 등골 탈구의 위험성이 있을 것으로 판단하여, 후고실 개방술을 크게 시행하여 등골을 향한 시야를 확보하였다. 종물은 등골 상부 구조의 반을 덮고 있었으나 어렵지 않게 종물을 등골로부터 분리할 수 있었다. 최종적으로 종물 양단의 고삭신경을 절단하여 종물을 제거하였다(Fig. 4B). 청력 개선을 위해 2 mm 높이의 티타늄 인조 이소골을 이용하여 부분 이소골 치환술을 시행하였다. 수술 후 안면마비, 어지럼 등 합병증은 없었고, 미각의 변화도 호소하지 않았다. 제거한 종물에 대한 병리조직검사에서 종물은 방추 형태의 세포들로 구성되어 있었고 면역형광염색에 방추세포들이 S-100 단백에 양성 반응을 보여 신경초종으로 최종 확진하였다(Fig. 5). 수술 6개월 후 시행한 순음청력검사에서 기도청력이 16 dB HL(6분법 평균)로 정상 청력으로 회복되었으며, 재발 소견없이 경과관찰 중이다.
The tumor arising from chorda tympani nerve is identified at the posterosuperior area of middle ear (arrow). Both ends of the mass are connected with chorda tympani nerve (A). A excised tumor sizing 8 mm in long-length (B).

The microscopic image of the tumor. H&E stain (A) shows that the mass is well demarcated and composed of bland-looking spindle cells with fascicular arrangement (×400). Immunohistochemistry for S-100 (B) demonstrates that the tumor cells show immunoreactivity for S-100, which is consistent feature of schwannoma (×400).
고 찰
신경초종은 말초신경의 신경초세포에서 기원하는 양성 종양으로 성장 속도가 느리며 인체의 말초신경이 있는 모든 부위에서 발생할 수 있다[1]. 신경초종은 발생하는 위치에 따라 다양한 증상이 나타난다. 중이에서 신경초종이 발생한 경우에는 청력 감소, 이명, 이통, 어지럼증, 안면마비 등의 증상이 발생할 수 있으며[3,4,6] 안면신경에서 발생하는 신경초종의 경우 안면마비가 동반된 난청 증상이 주로 보고되었다[7].
고삭신경에서 기원하는 신경초종은 이내시경검사 시 고막 내부에 비쳐 보이는 중이 종물로 발견될 수 있다[3]. 중이 내 종물로 발현될 수 있는 질환에는 선천성 진주종, 신경초종, 그리고 혈관성 종양 등이 있다. 이들 질환은 치료방법과 예후가 서로 다르기 때문에 이내시경검사와 영상검사를 통해 수술 전 원인 질환에 대한 감별이 필요하다. 선천성 진주종의 경우 이경 검사상 고막 내부의 백색의 종물로 보인다. 자기공명영상에서는 T1강조영상에서 저신호강도, T2강조영상에서 고신호강도를 보이고, 특징적으로 확산강조영상에서 고신호강도를 보이면서 조영 증강이 되지 않는다[8,9]. Glomus 종양과 같은 혈관성 종양은 T1강조영상과 T2강조영상에서 뇌실질과 비슷한 신호강도를 보이고 확산 강조영상에서 저신호강도를 보인다. 혈관이 풍부하기 때문에 조영 증강을 보이고 특징적으로 아급성 출혈과 혈류로 인한 무신호를 의미하는 “salt and pepper” 소견을 확인할 수 있다. 신경초종의 경우에는 자기공명영상의 T1강조영상에서는 뇌실질과 같은 신호강도로 나타나고 T2강조영상에서는 뇌실질과 같거나 높은 신호강도로 관찰된다. 확산 강조영상에서는 종물의 성상에 따라 낮은 신호강도에서 높은 신호강도까지 다양한 양상을 보이며 신생물이므로 조영 증강되는 특징을 가진다[9-11]. 자기공명영상이 이러한 중이 중물의 감별점을 제공하기는 하지만, 확진은 수술적 제거 후 병리검사를 통해 이루어진다[7].
신경초종은 조직병리학적으로 종물의 피막화가 잘 이루어져 있으며, 종물 내 방추세포들이 울타리 배열을 하고 있다. 베로케이 소체(verocay body)를 구성하는 안토니 A(antoni A)배열이나, 세포 충실도가 낮고 느슨한 기질 조직 부위인 안토니 B를 가지는 조직학적 특징 및 면역 조직화학 염색에서 S-100 단백에 양성 소견을 보인다[10]. 본 증례도 방추세포들의 안토니 A 배열과 S-100 단백에 대한 양성 반응을 통해 신경초종으로 최종 진단할 수 있었다.
신경초종의 치료는 수술을 통한 종물의 제거이다. 고삭신경이 미각을 담당하는 감각신경이지만 고삭신경에서 기원한 신경초종을 제거하는 경우 미각 저하는 발생하지 않는다고 보고되고 있다. 이는 고삭신경에서 기원한 신경초종이 매우 느리게 성장함에 따라 그 기간 동안 미각에 대한 보상작용이 일어나기 때문으로 추정된다[11]. 본 증례도 수술 전과 수술 후 미각 변화를 호소하지 않았다.
고삭신경은 해부학적 위치상 이소골과 근접해 있기 때문에 신경초종에 의해 이소골이 파괴될 수 있고 수술 시 종물의 완전 제거를 위해 이소골 일부의 제거가 필요할 수 있으며, 이 경우 이소골 재건술을 시행하여야 한다. 본 증례에서도 종물에 의해 침골의 장돌기가 파괴되어 있었기 때문에 종물 제거 후 부분 이소골 치환술을 시행하여 청력을 회복할 수 있었다.
고삭신경 신경초종의 제거 수술 후 2년 이상 경과관찰을 시행한 해외의 세 개의 증례 보고 중에서 재발은 없었다[2,3]. 본 증례의 경우에도 수술 후 10개월 동안 경과관찰을 시행하고 있으며 현재까지 재발의 소견은 보이지 않고 있다.