비용종을 동반한 만성 비부비동염의 바이오마커: 내재형에 기초한 맞춤의료
Biomarkers in Chronic Rhinosinusitis with Nasal Polyp: Personalized Medicine Based on Endotype
Article information

Trans Abstract
Chronic rhinosinusitis (CRS) is divided into CRS with nasal polyp (CRSwNP) and CRS without nasal polyp (CRSsNP) according to the presence of a nasal polyp. Some of the CRSwNP patients are relatively well managed without recurrences while others are difficult due to recurrence and refractoriness after surgical or medical treatment. Thus CRSwNP is not a single disease but is rather considered as a disease that has a variety of disease spectrum. Various biomarkers have been proposed to distinguish endotypes of CRSwNP. CRSwNP with high tissue eosinophil infiltration with robust type 2 inflammation (e.g., IL-5) is usually associated with comorbid asthma and is likely to recur. This type of CRSwNP is relatively common in Western countries. However, in Asian countries, CRSwNP is often presented as a heterogeneous disease comprising a mixture of type 1 (e.g., IFN-γ), type 2 and type 3 (e.g., IL-17) inflammation. In Asians, up-regulation of IL-8, IFN-γ and associated neutrophilic inflammation is prone to have disease refractoriness. Different underlying inflammatory profile indicates different underlying pathogenesis. Therefore, in the era of precision medicine, treatment should be based upon according to endotype.
서 론
현재의 분류 기준에 의하면 만성 비부비동염(chronic rhinosinusitis, CRS)은 비용종(nasal polyp)의 유무에 따라 비용종을 동반한 만성 비부비동염(CRS with nasal polyp, CRSwNP)과 비용종을 동반하지 않은 만성 비부비동염(CRS without nasal polyp, CRSsNP)으로 나뉜다[1]. 우리나라의 경우 CRS는 전체 인구의 약 8.4% 정도의 빈도로 존재하며, 이 중에서 CRSwNP은 전체 인구의 약 2.6%인 것으로 알려져 있다[2]. 대체적으로 CRSwNP은 CRS의 약 20~50% 정도를 차지하지만, CRSwNP의 경우 치료가 더 어려우며 약물과 수술적 치료를 하더라고 환자들이 느끼는 증상도 더 심하다[3]. 우리나라에서도 CRSwNP은 굉장히 흔한 질병이기 때문에 이에 따른 사회 경제적 손실도 상당한 것으로 알려져 있다.
현재까지의 CRS의 분류는 환자가 가지는 표현형(phenotype), 즉 내시경적 검진을 통해 비강 내 비용종을 동반하는지(CRSwNP) 혹은 동반하지 않는지(CRSsNP)에 따라 이루어지지만, 똑같은 CRSwNP 환자라고 하더라고 어떤 환자에서는 수술 및 약물 치료에 잘 반응을 하는 반면, 다른 어떤 환자에서는 수술적 치료와 약물 치료를 하더라도 반응하지 않거나 재발하는 경우가 있어 CRSwNP 안에서도 여러 가지 다양한 임상양상을 보이고 있다. 이러한 사실을 바탕으로 최근의 개념은 CRSwNP는 하나의 획일된 질환이 아니라 서로 다른 다양한 질병 스펙트럼(disease spectrum)을 가지는 여러 내재형(endotype)으로 구성된 질환으로 보고 있다[4].
표현형에 따른 분류는 “기저 병태생리와 직접적인 연관 없이 유전자형과 환경과의 상호 작용으로 인해 나타나는 임상적으로 관찰이 가능한 특징들에 의한 구분”으로 정의할 수 있으며, 내재형에 따른 분류는 “독특한 병태생리 유전학적 기전에 따른 구분”으로 정의할 수 있다[5].
따라서 여러 내재형으로 이루어진 CRSwNP에 대한 이해를 하기 위해서는 이를 각각 내재형의 독특한 병태생리 유전학적 기전 즉 바이오마커(biomarker)를 알아보아야 한다.
이러한 바이오마커는 영상 소견, 내시경 소견과 같은 임상적으로 나타나는 표현형보다 더 객관적이며, 정량적이어서 실제 내재된 병태생리를 더 잘 반영하는 것으로 알려져 있다[6].
이에 본 종설에서는 CRSwNP의 바이오마커에 대한 최신의 지견에 대해 리뷰하고자 한다.
비용종을 동반한 만성 비부비동염의 바이오마커(Biomarkers in CRSwNP)
바이오마커의 원천(Source of biomarker)
일반적으로 바이오마커는 비분비물, 비강 조직검사, 호기산화질소, 말초혈액 등을 채취하여 얻을 수 있다. 비분비물은 비교적 채취하기가 용이하고, 관찰되는 싸이토카인 수치도 조직 내 발현 정도와 비교적 잘 일치하는 것으로 알려져 있다[7]. 비강 조직검사를 통해서는 조직 내 염증(inflammation)을 나타내는 각각의 구조적 특징, 염증 세포의 구성, 조직 내 싸이토카인의 발현 정도를 비교적 더 구체적이면서 정확하게 측정할 수 있다. 호기 산화질소의 측정은 가장 비침습적이며, 간단하고 빠르게 검사를 시행할 수 있는 방법으로 천식에서 내재형을 구별하는 데에 현재 사용되고 있지만 CRSwNP에서의 활용은 아직은 잘 밝혀지지 않은 상태이다. 말초혈액에서의 싸이토카인 혹은 호산구(eosinophil), 특정 림프구(lymphocyte)와 같은 세포를 측정하는 것은 비강 조직을 대변하는 데에는 한계가 있지만 현재까지 임상적으로 가장 현실적이고, 경제적인 검사 방법이라 할 수 있다.
현재까지 CRSwNP에서 바이오마커의 발굴은 꾸준히 증가하고 있으며 천식, 아토피성 피부염과 같은 질환에서 미리 알려진 바이오마커들도 CRSwNP에서 일부 연관이 있는 것으로 알려져 있다. 최근의 “omics” 기술의 발달로 특정 유전자 및 단백질로 구성된 후보군들은 더욱 증가하고 있는 추세이다. 하지만, 질환의 병태생리는 복잡하기 때문에 바이오마커 후보군들의 각자로 병태생리를 이해하는 것은 어떻게 보면 전체 큰 틀에서 아주 일부 한 조각만 보는 꼴이기 때문에, 궁극적으로는 여러 바이오마커를 한꺼번에 보는 multiplex panel이 필요할 것으로 사료된다.
조직 내 혹은 혈중 호산구(Tissue or blood eosinophil)
조직 내 혹은 혈중 호산구(tissue or blood eosinophil) 수치는 현재까지 가장 잘 알려진 CRSwNP의 바이오마커이다. 서양에서는 80% 이상의 CRSwNP에서 조직 내 호산구 침윤(tissue eosinophilia)을 보이고 있는 반면, 우리나라를 비롯한 중국, 일본 등 동아시아에서의 CRSwNP에서는 약 50% 정도에서만 조직 내 호산구 침윤을 보이는 것으로 알려져 있다[8]. 호산구성 비용종을 동반한 만성 비부비동염, 즉 호산구성 비용종증(eosinophilic CRSwNP)의 경우 glucocorticoid에 잘 반응을 하는 것으로 알려져 있지만 그렇지 않은 경우, 임상적으로 천식이 동반이 잘 된다거나 수술 후 재발이 더 흔하게 일어나기 때문에, 일반적으로 예후가 더 좋지 않다[9]. 반면 조직 내 호산구의 침윤이 많지 않은 비호산구성 비용종증(noneosinophilic CRSwNP), 특히 호중구(neutrophil)의 침윤이 많은 경우에는스테로이드에 대한 반응이 낮은 것으로 알려져 있다[10]. 이러한 특징 때문에 많은 임상의들이 CRSwNP의 분류에 있어서 조직 내 호산구를 사용하고자 하였다.
하지만 아직까지 조직 내 호산구(tissue eosinophilia)에 대해서는 전세계적으로 공감을 이룰 만한 명확한 기준이 없다. 조직 내 침윤된 호산구는 400배율의 현미경에서 직접 숫자를 세는 방법[counts per high power field(HPF)]이 있고, 좀 더 직관적이고 주관적일 수 있으나, 침윤된 염증 세포(inflammatory cell) 중 호산구가 차지하는 비율로 하는 기준이 있다. 또한 조직을 갈아서 조직 내 발현된 eosinophil cationic protein(ECP)/myeloperoxidase(MPO) 비율을 기준으로 하는 경우도 있다. 최근에 일본의 다 기관 연구에서 밝혔듯이 호산구의 수가 >70/HPF 이상일 때 유의한 재발 증가를 보였는데[9], 바이오마커가 질병의 예후를 가장 잘 반영했을 때 가장 의미있는 것이라 생각한다면 이 기준이 좋은 예가 될 것이다. 하지만 조직 내에서 호산구의 침윤이 균일하게 분포되어 있지 않고, 똑같은 질환이라도 시간에 따른 변화가 존재하기 때문에 이들을 항상 감안해야 할 것이다.
제2형 싸이토카인(Type 2 cytokine)
예전에는 CRSwNP에서 Th2 세포에서 발현 및 분비되는 것으로 알려진 IL-4, IL-5, IL-13과 같은 전통적 Th2 싸이토카인의 분비가 증가되어 있기 때문에, CRSwNP는 병태생리적 측면에서 Th2가 중추가 되는 후천적 면역반응(acquired immune response)에 의해 생기는 것으로 여겨져 왔다. 하지만 Th2 세포뿐만 아니라 innate lymphoid cell type 2(ILC2)라는 세포가 CRSwNP에서도 발견이 되었고[11,12], 이 세포에는 상피 세포에서 분비된 싸이토카인(TSLP, IL-25, IL-33) 등에 의해 자극되어 Th2 세포와 매우 동일한 기능을 하는 것으로 알려지면서 IL-4, IL-15, IL-13 등은 Th2 싸이토카인보다는 제2형 싸이토카인(type 2 cytokine)으로 불려지기 시작하였고, 이들이 호산구성 비용종증을 특징짓는 중추적인 바이오마커로 알려져 있다[13].
IL-5는 호산구를 조직 내로 모집하는(recruitment) 가장 중요한 역할을 하는 싸이토카인 중 하나이며[14], 호산구의 침윤을 결정짓는 중요한 역할을 하는 것으로 알려져 있다[15]. IL-5가 높게 발현되는 CRSwNP는 병발하는 천식이 있을 가능성이 높으며, 또한 재발하여 재수술을 해야 하는 확률이 더 높은 것으로 알려져 있다[15-17]. 최근에 시행된 한 연구에 의하면 조직 내 발현되는 특정 싸이토카인의 발현 정도를 가지고 군집 분석(cluster analysis)을 통하여 확인한 결과 IL-5, IFN-r, IL-17a, TNF-a, IL-22, IL-1b, IL-6, IL-8, ECP, MPO, TGF-b1, IgE, Staphylococcus aureus (S. aureus) enterotoxin specific IgE, albumin의 바이오마커의 조합으로 CRS를 10개의 군집으로 내재화(endotyping)를 할 수 있으며, 이 중에서 특히 IL-5가 높게 발현될수록 CRS에서 비용종을 동반하는 경우가 많고, 이와 더불어 병발하는 천식의 비율이 높은 것으로 알려졌다[18]. 이처럼 IL-5는 CRSwNP의 병태생리에 중추적인 역할을 할 것으로 생각되며, 특히 호산구성 비용종증과 가장 연관된 싸이토카인이라 할 수 있다. 이를 타겟으로 하는 항 IL-5 의 치료가 일부 CRSwNP에서 중요한 치료제로 역할을 할 것으로 기대 된다. 현재까지 개발된 항 IL-5 단클론항체로는 reslizumab과 mepolizumab이 있으며, 이를 사용한 몇몇의 임상시험에서 의미있는 용종 크기의 감소와 혈중 호산구 수치의 감소를 보였다[19,20]. 특히 비즙에서 측정된 IL-5는 reslizumab에 대한 반응을 예측 할 수 있는 것으로 알려져 있어[19] 비교적 현실적인 바이오마커로 생각된다.
IL-4와 IL-13도 중추적인 제2형 싸이토카인으로 이 둘은 서로 상승 작용에 의해 B 세포에서의 IgE의 생성을 촉진시키며, 상피 세포에서 점액 분비를 촉진하는 것으로 알려져 있다. Il-4와 IL-13의 수용체(receptor)는 서로 alpha subunit을 공유하는데, 이를 target으로 하는 항 IL-4/IL-5 단클론항체인 dupilumab의 제2상 임상시험에 의하면, 16주 동안 주 1회 피하로 dupilumab을 접종하였을 때 유의하게 내시경, CT 소견과 후각을 비롯하여 증상이 호전되었다[21].
최근 들어서 상피 세포에서 분비되는 것으로 알려진 IL-25, IL-33, TSLP(epithelial derived cytokine)는 Th2 세포, Th2 세포를 활성화시키는 수지상 세포(dendritic cell), 그리고 ILC2를 자극하여 궁극적으로 제2형 염증반응(type 2 inflammation)으로 유도하는 역할을 하는 것으로 알려져 있다[22-25]. 이중 IL-33는 조직 내 호중구(neutrophil)을 모집(recruitment)하는 데에도 역할을 하는 것으로 알려졌다[26]. TSLP는 특히 수지상 세포의 표면에 OX40L의 발현을 증가시키는데, OX40L는 CD4 T 세포의 OX40 수용체(receptor)와 작용하여 naı¨ve T 세포를 Th2 세포로 분화를 촉진시키는 것으로 알려져 있다. 비록 CRSwNP는 아니지만, 천식 환자들을 대상으로 항 TSLP 단클론항체인 AMG 157을 사용한 제2상 임상시험에서 AMG 157을 사용한 군에서 항원(allergen)에 의해 유도되는 기관지수축(broncho-constriction), 객담 및 혈중 호산구 수치를 감소시킨 것으로 나타났다[27]. 비록 아직까지 CRSwNP에 관하여 이들 바이오마커를 대상으로 하는 임상시험은 시행된 바 없지만, IL-25, IL-33, TSLP는 일부 CRSwNP에서 발현이 증가되어 있으며, Lund-Mackay CT score, 혈중 호산구 수치와 유의한 상관관계를 보이고 있고, IL-33의 경우 치료에 잘 반응하지 않는 불응성(recalcitrant) CRS에서 증가되어 있는 것으로 알려져 있다[28-30]. 또한 CRSwNP 동물모델에서 항 IL-33의 효과가 일부 입증되었기 때문에[26], CRSwNP에서도 효과가 있을 것으로 기대된다.
또 하나의 바이오마커인 periostin은 상피 세포, 호산구, 섬유아 세포 등에서 분비하는 물질로, 상피하층(subpithelial layer)의 섬유화(fibrosis)에 중추적인 역할을 하는 것으로 알려져 있는데. 이외에도 periostin은 상피 세포에서의 TSLP 분비를 촉진시키는 것으로 알려져 있다[31]. 이러한 periostin의 분비는 비만세포(mast cell)에서도 이루어지는데, 이는 IgE mediated signaling에 의해 이루어지는 것으로 알려져 있다[32]. 실제로 천식에서의 혈중 periostin의 농도는 항 IgE 단클론항체인 omalizumab에 대한 반응을 예측하게 하는 또 하나의 바이오마커로 알려져 있는데[33], CRSwNP에서도 비슷한 역할을 할 것으로 기대된다.
B 세포 관련 바이오마커
B 세포는 후천 면역에서 중추적인 역할을 하는 면역 세포로 CRSwNP에서 염증을 지속시키는 중요한 역할을 하는 것으로 알려져 있으며, CRSwNP의 조직 내에는 증가된 naïve B세포뿐만 아니라 형질 세포(plasma cell)들이 증가되어 있는 것을 볼 수 있다[34].
CRSwNP 조직 내 많이 발견되는 B 세포와 연관되어 조직 내에서 면역글로블린(immunoglobulin)이 증가되어 있는 것을 확인할 수 있는데, 많은 경우가 다수의 B 세포에서 생성된 다중클론성항체(polyclonal antibody)로 특정 항원이 잘 알려지지 않는 반면, 일부에서는 자가항원특이항체(autoantigen-specificantibody) IgG와 IgA [35], 혹은 staphylococcal enterotoxin 특이 IgE 등이 높게 발견된다[36]. 특이하게도 이러한 면역글로블린은 주로 혈액에서는 높게 측정되지 않고, 비용종 조직 내에서 높게 측정된다. 특히 조직 내 staphylococcal enterotoxin 특이 IgE가 발견되는 경우, 조직 내에서 total IgE의 수치가 높게 나오는데[37], 이는 enterotoxin의 superantigen 작용으로 B 세포의 다클론성 면역글로블린의 합성을 일으켰기 때문일 것으로 생각된다(Fig. 1). 뿐만 아니라 일부에서는 특이 항원이 발견되지 않는 IgG, IgA도 발견이 되기도 한다[38]. 따라서 CRSwNP의 병태생리에 IgE, IgG, IgA가 모두 관여를 할 것으로 생각되며, 비용종 조직 내 많은 세포에서 Fc 수용체(receptor)가 발현되어 있고, 조직에 축적된 면역복합체(immune complex)가 보체에 의한 케스케이드 경로(cascade pathway)를 활성화시킨다[39].

Activation of B cells and T cells by superantigen from S. aureus. Activated B cells produces polyclonal IgE antibodies which accumulates in the polyp tissue. One of the actions of accumulated immune complex is the activation complement cascade pathways. Activated T cells produces IL-5 which further recruits eosinophils. S. aureus: staphylococcus aureus.
Omalizumab은 유리된 IgE에 강하게 달라붙어 IgE가 crosslinking되는 현상을 방지하는 단클론성항체로 주로 중층천식(severe asthma)의 치료제로 사용된다. 한 무작위 임상시험(randomized controlled trial)에 의하면 중증 천식 환자 중 CRSwNP가 있는 환자가 이로 치료받으면 polyp의 크기가 유의하게 줄어들며, CT상에서 부비동의 혼탁도(opacity)를 유의하게 줄이는 것으로 확인되었으며 이러한 효과는 전신 아토피에 상관없이 나타나는 것으로 알려졌다[40].
B cell activating factor of the TNF family(BAFF)는 최근에 발견된 TNF superfamily 중 하나로, B 세포의 생존(survival), 증식(proliferation), 그리고 성숙(maturation)에 중요한 역할을 하는 것으로 알려져 있다. BAFF는 transmembrane activator and CAML interactor(TACI)와 결합하여 B 세포의 class-switch recombination 및 이로 인한 IgA의 생성에 중요한 역할을 한다. 비록 CRSwNP의 병태생리에서 IgA가 어떠한 역할을 하는지 아직 자세히 알려지진 않았지만 호산구에서의 탈과립화(degranulation)를 촉진시키는 것으로 알려져 있다. BAFF는 CRSwNP에서 발현이 높아져 있고, 이와 연관되어 B 세포의 표면 항원인 CD20과 IgA가 증가되었는데[41], 이처럼 BAFF에 의한 B 세포의 활성화와 IgA 생성에 의한 호산구의 탈과립이 CRSwNP의 병태생리에 중요한 역할을 할 것으로 생각된다.
동양형 비용종증에서의 바이오마커
대부분의 바이오마커는 호산구성 비용종증이 대부분인 서양 환자들을 대상으로 시행한 결과이다. 따라서 병태생리가 다르다고 생각되는 동양형 비용종증에 대한 바이오마커를 찾아보려는 노력이 필요하다고 할 수 있다. 동양형 비용종증은 서양 환자들에서 보이는 임상양상이 서로 다른 것으로 알려져 있다. 한 다국적 연구에 의하면 동일한 방법으로 비용종의 면역학적 특징을 분석한 결과 서양의 경우 제2형 염증반응으로 치우쳐진 반면, 동양인의 경우, CRSwNP 환자 개개인에서는 특정 염증 패턴을 볼 수 있지만, 환자들을 전체적으로 본다면 특정 염증 패턴으로 치우쳐 있다기보다는 제1형, 제2형, 제3형 염증반응의 다양한 패턴을 보이고 있다[42]. 제1형 및 제3형 염증반응은 각각 제1형 및 제3형 싸이토카인이 많이 활성화되어 있는 상태로, Th1, Th17 세포뿐만 아니라, 이들 세포들과 비슷한 기능을 하는 ILC인 ILC1(Th1) 및 ILC3(Th17)가 발견됨으로써 T 세포 및 ILC에 의해 IFN-γ(제1형 싸이토카인), IL-17(제3형 싸이토카인) 등이 높아져 있는 상태를 의미한다. 동양에서 비교적 흔하게 발병하는 비호산구성 비용종증에서는 제2형 염증반응이 적은 반면, IL-17의 발현이 상대적으로 많은 것을 확인할 수 있는데, IL-17은 호중구를 조직 내로 끌어들이고 활성화하는 것으로, 이는 동양인의 비호산구성 비용종증에서 비교적 스테로이드의 반응성이 떨어지는 것을 설명할 수 있다. 하지만 동양인에서 IL-17과는 별개로, IL-8, IFN-γ, GM-CSF, 그리고 조직 내 호중구의 침윤이 많은 경우 치료에 불응하는 경우가 많다[43].
하지만 Tomassen 등[18]의 연구에서 처럼 동서양을 떠나서 CRS는 이분법적(dichotomic)인 질환이 아니라 다양한 내재형(endotype)으로 이루어진 복잡한 질환이고, 인종적 차이에 의해(아마도 genetic background) 내재형의 분포가 서양인과 동양인이 차이가 있을 것으로 보이며(Fig. 2), 실제로 인종과는 상관없이 각자의 내재형이 있고, 이와 관련된 표현형(phenotype)이 일관되게 유지되는 것으로 알려져 있다[42]. 따라서 동양형의 특정 바이오마커라고 하기보다는 동양인에서 비교적 흔하게 보이는 비호산구성 비용종증의 경우, 조직 내 염증반응이 제1형 및 제3형 싸이토카인이 높아진 특징을 보이는 경우로 보아야 할 것이며, 이에 대해서는 IL-17a, IL-22와 같은 물질들을 바이오마커로 생각할 수 있으며, 이들에 대한 단클론항체가 치료를 생각해 볼 수 있을 것이다. 지금까지 이들 싸이토카인에 대한 몇몇의 단클론항체들이 있으며 현재 임상시험 중인 것으로 알려져 있지만 아직까지 이들의 효과가 확인되지는 않았다.

Endotype distribution among Western and Asian polyps. Both are mixture of type 2 and 1/17 inflammation. Western polyps are more shifted towards type 2 inflammation, while as Asian polyps are more shifted towards type 1/17 inflammation.
임상적으로 쉽게 얻을 수 있는 바이오마커
지금까지 언급한 바이오마커와 이들은 단클론항체를 Table 1에 정리하였다. 이들 대부분은 혈중, 비즙, 혹은 조직 내에서 직접 측정한 것들이다. 하지만 실질적으로 임상적으로 적용하는 데에 있어 비즙 혹은 조직 내 단백질을 직접 측정하는 데는 한계가 있다. 따라서 조직 내 단백질 단계에서의 바이오마커를 잘 반영하는 임상적인 지표를 찾고자 하는 노력이 있어왔고, 대표적인 것이 Japanese clinical scoring study (JESREC)이다[9]. 이는 비교적 실제 임상 현장에서 많이 평가되는 항목들로 이루어져 있다. JESREC score는 1) CT에서의 ethmoid/maxillary(EM) ratio, 2) 혈중 호산구 비율, 3) 천식 유무, 4) aspirin을 비롯한 NSAID에 대한 과민성 유무에 따라 수술 후 질환의 재발 위험도를 기반으로 하는 scoring system으로 점수에 따라 non-eosinophilic CRS(non-ECRS), mild ECRS, moderate ECRS, severe ECRS로 구분할 수 있다. Severe ECRS일수록 수술 후 재발(recurrence)과 치료에 대한 불응도(refractoriness)가 높은 것으로 알려져 있다. JESREC score는 면역학적으로도 검증이 되었는데, severe, moderate일수록 IL-5, 1L-13과 같은 제2형 싸이토카인이, non-ECRS, mild ECRS일수록 IFN-γ, IL-17a, CXCL1 등 제1형/제3형 싸이토카인이 증가되어 있다[44].
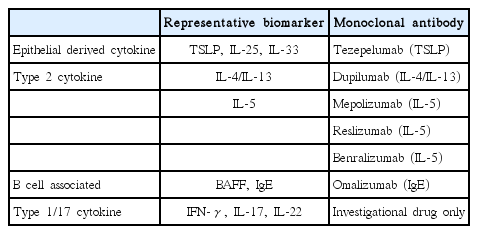
Representative biomarkers in chronic rhinosinusitis with nasal polyp and their targeting monoclonal antibodies
비슷한 연구가 국내에서도 있었는데[45], 이 연구에서는 CRSwNP 환자들의 임상적인 특징 즉 CT에서의 Lund Mackey score, E/M ratio, 조직 내 호산구 침윤 정도, 천식 유무, 그리고 환자의 수술 당시 나이를 기반으로 CRSwNP를 분류하였다(Fig. 3). 조직 내 호산구 침윤 정도는 임상적으로 쉽게 구해지도록 현미경으로 직접 호산구의 개수를 세는 방법보다는 전체 침윤된 염증 세포 중에서 호산구가 20% 이상인 경우로 정의하였는데, 이는 비교적 쉽게 병리과 의사의 직관에 의해 정해진다. 이 연구에 의하면 1) 천식과 동반된 호산구성 비용종증, 2) 천식이 없더라도 E/M ratio가 2.2 이상인 호산구성 비용종증, 3) 나이가 비교적 젊은 비호산구성 비용종증의 경우 재수술의 빈도가 비교적 높다.
Algorithm for classification of polyps by using routinely available clinical markers. Patients are classified into 1 of 6 clusters based on the presence of tissue eosinophilia, presence of asthma, age, and E/M ratio.A1: asthmatic, non-eosinophilic polyp, A2: asthmatic eosinophilic polyp, NA1: non-asthmatic non-eosinophilic polyp with older age, NA2: non-asthmatic non-eosinophilic polyp with younger age, NA3: non-asthmatic eosinophilic polyp with lower E/M ratio, NA4: non-asthmatic eosinophilic polyp with higher E/M ratio. E/M: ethmoid/maxillary.
CRSwNP는 여러 가지 내재형(endotype)으로 구성된 복합적인 질환으로 각각 내재형에 대한 바이오마커에 대하여 알아보았다. 서양형 비용종증에서는 호산구성이 많은 반면 동양형 비용종증에서는 비호산구성이 많은 것으로 알려져 있다. 호산구성 비용종증은 제2형 염증이 많이 발현되어 있지만, 비호산구성 비용종증은 제2형 염증은 적은 반면 상대적 제1형 혹은 제3형 염증반응이 증가되어 있다. 하지만, 각각의 인종에 따라 내재형이 서로 다르다고 표현하기보다는 여러가지 내재형의 분포가 인종마다 다르다고 해석하는 것이 더 합당하다. 각각의 내재형은 이를 특징하는 표현형(e.g., 동반된 천식 유무)을 가지고 있다. 이러한 내재형을 바탕으로 개인맞춤형 치료(targeted therapy)가 가능할 것으로 보인다. 하지만 실제로 일관되고, 임상에서 쉽게 얻어지는 검사 방법을 통해 확인할 수 있는 바이오마커를 찾는 것 또한 중요할 것이다.
Acknowledgements
This work was supported by the National Research Foundation of Korea (NRF) grants funded by the Korea government (MSIP) (no.2019R1C1C1009886).