Cross-Cultural Adaptation and Validation of the Nasal Obstruction Symptom Evaluation Scale in the Korean Language
한국어판 Nasal Obstruction Symptom Evaluation 척도 타당도 및 신뢰도 연구
Article information

Abstract
Background and Objectives
Nasal obstruction is a prevalent symptom that is usually reported subjectively. The Nasal Obstruction Symptom Evaluation (NOSE) scale is a reliable method for evaluating subjective nasal obstruction. This study aimed to evaluate the reliability and validity of the Korean version of the questionnaire (K-NOSE).
Subjects and Method
The cross-cultural adaptation of the K-NOSE followed generally accepted methodologies. The patient group included individuals undergoing surgery for nasal obstruction, and the control group consisted of individuals without nasal obstruction complaints. Patients completed the K-NOSE three times (twice at a 2-week interval preoperatively and once postoperatively) while controls completed it once. To assess criterion-related validity, all participants also completed a visual analog scale (VAS) for nasal obstruction. Reliability, validity, and responsiveness of the K-NOSE were evaluated in 57 patients and 52 controls.
Results
The K-NOSE showed good internal consistency (Cronbach’s α >0.7). Test-retest reliability of the questionnaire in the patient group was found to be statistically significant (p<0.001). The scores were significantly lower for controls than for patients (p<0.001), indicating good discriminant validity of the questionnaire. Postoperative scores significantly decreased compared to preoperative scores (1.15±1.482 vs. 13.85±3.701; p<0.001), indicating good sensitivity to change. Correlation analysis between VAS and K-NOSE showed a statistically significant association in the patient group (p<0.05), supporting criterion-related validity.
Conclusion
The K-NOSE was found to be reliable and valid. It can be used as a practical tool to evaluate patients’ subjective nasal obstruction and surgical outcomes.
Introduction
Patients often report nasal obstruction or congestion as a common symptom, which arises from diverse etiologies. While the terms “nasal congestion” and “nasal obstruction” are frequently used interchangeably in clinical practice, they are not entirely synonymous. Nasal congestion refers to a sensation of fullness, blockage, or obstruction in the nasal cavity, typically indicating a reversible condition. In contrast, nasal obstruction generally denotes an irreversible blockage of the nasal airway [1]. As nasal obstruction or congestion substantially impacts quality of life, physicians should endeavor to objectively define and evaluate patients’ symptoms [1].
Acoustic rhinometry, rhinomanometry, and peak nasal inspiratory flow are commonly used objective tests for evaluating nasal obstruction [2]. However, the results of these tests often show weak or no significant correlation with patients’ subjective experiences of nasal obstruction [3,4]. To address this gap, the Nasal Obstruction Symptom Evaluation (NOSE) scale was developed as a standardized tool to assess patients’ subjective perceptions of nasal obstruction, particularly for evaluating symptom improvement after septoplasty [5]. Since its development, the NOSE scale has been widely utilized across the globe, with translations and validations conducted in numerous languages. According to a review of the English-language literature, it has been translated into 17 different languages to date [6-22]. In addition, a Chinese version of the NOSE scale exists, although it has not been published in English-language literature. The Standardized Cosmesis and Health Nasal Outcomes Survey has been translated and validated in Korean, and is currently in clinical use in Korea [23]. However, to the best of our knowledge, a Korean version of the NOSE (KNOSE) scale has not yet been developed. This study aims to translate and validate the K-NOSE scale.
Subjects and Methods
Study design & study population
We conducted a prospective, multicenter study. Each participating institution began participant recruitment following approval from its respective Institutional Review Boards (2024-03-007). Informed consent was obtained from all participants prior to enrollment. The study was conducted from May 1, 2022, to April 10, 2025.
This was a prospective study in which participants were recruited and divided into a patient group and a control group. Referring to previous NOSE translation studies, the required sample size was calculated to be 46, using a power of 0.80, an alpha level of 0.05, and a correlation coefficient of 0.40 for construct validity [5,11,17]. In consideration of a 10% dropout rate, the target sample size was set at more than 50 participants in each of the patient and control groups.
The inclusion criteria of the patient group were as follows: adults aged 19 years or older who had experienced nasal obstruction for more than 3 months and had not shown improvement after at least 4 weeks of other treatments, such as medications or intranasal sprays. Participants were required to be native Korean speakers who could read and speak Korean. The patient group underwent septoplasty to improve nasal obstruction symptoms. Patients who additionally underwent inferior turbinoplasty or nasal valve surgery during septoplasty were also included. Exclusion criteria for the patient group included patients younger than 19 years, those with a history of prior surgical interventions for nasal obstruction (e.g., septoplasty, rhinoplasty, or inferior turbinoplasty), and those with nasal obstruction due to facial deformities, intranasal tumors, rhinosinusitis, septal perforation, or adenoid hypertrophy. Computed tomography and nasal endoscopy were performed to rule out other possible causes of nasal obstruction. The control group consisted of otologic outpatients who visited the clinic for tinnitus or hearing loss but did not report nasal obstruction. Participants were also native Korean speakers aged 19 years or older who were literate in Korean, had no history of nasal obstruction, and were not candidates for nasal surgery. All participants were informed of the purpose of the study and provided written informed consent prior to the initiation of the research.
Translation of the K-NOSE
The K-NOSE was translated and culturally adapted into Korean following a standardized cross-cultural adaptation process [24,25]. For the forward translation, two professional translators whose native language was Korean and who had no medical background independently translated the original NOSE into Korean. The two independently translated questionnaires were combined into a single joint questionnaire, with minor differences resolved through discussion. The backward translation was then performed by two professional translators who were native English speakers without a medical background. Each translator independently translated the single provisional K-NOSE into English. The resulting English versions were compared to the original NOSE scale to ensure consistency and accuracy. Based on this comparison, the final K-NOSE scale was established (Fig. 1). NOSE items followed the original version NOSE order: 1) nasal congestion or stuffiness (nasal congestion); 2) nasal blockage or obstruction (nasal blockage); 3) trouble breathing through my nose (trouble breathing); 4) trouble sleeping (trouble sleeping); and 5) unable to get enough air through my nose during exercise or exertion (exercise or exertion).
The final Korean version of the Nasal Obstruction Symptom Evaluation scale.
Data acquisition & validation of the K-NOSE
In the absence of an objective and quantitative test for subjective nasal obstruction, the original study by Stewart, et al., along with many subsequent studies, used the visual analog scale (VAS) to assess the criterion validity of the NOSE scale [5,9,12-14,17,20]. VAS was used to subjectively assess the degree of nasal obstruction. It is a numeric scale ranging from 0 (no obstruction) to 10 (complete obstruction), where patients were asked to select a single number that best represents their perceived level of nasal obstruction. To assess test-retest reliability, patients completed the K-NOSE and VAS questionnaires at 2-week intervals before surgery. Patients who reported any changes in their nasal obstruction symptoms over the course of this period were excluded from the study. Two months after surgery, patients were asked to complete the K-NOSE and VAS questionnaires again to assess postoperative outcomes. In contrast, the control group completed the K-NOSE and VAS questionnaires once at their enrollment visit.
Statistical analysis
Reliability was assessed by evaluating internal consistency through Cronbach’s α and test-retest reliability using Pearson’s correlation coefficient and the intraclass correlation coefficient (ICC). Validity was assessed by examining discriminant validity with Student’s t-test and criterion-related validity through Spearman’s correlation analysis with the VAS questionnaire for nasal obstruction. Construct validity was assessed using item-item and item-total correlations. Responsiveness was evaluated by comparing preoperative and postoperative K-NOSE scores within the patient group using a paired t-test. Statistical analyses were conducted using SPSS version 20.0 software (IBM Corp.), with a significance level set at p<0.05 for all tests.
Results
A total of 110 participants were included in the study, consisting of 58 patients (36 men and 22 women; mean age, 42.9 years; age range, 20 to 80 years) and 52 controls (22 men and 30 women; mean age, 38.9 years; age range, 22 to 58 years). Fifty-seven of 58 enrolled patients completed all assessments (one dropout at 1-month postoperative follow-up).
Internal consistency was assessed using Cronbach’s α, which yielded a coefficient of 0.813, indicating high internal consistency (α>0.7 is considered acceptable [26]). The K-NOSE scale comprises 5 items, and the corrected item-total correlation values for all items exceeded 0.3, demonstrating adequate inter-item correlation. The Cronbach’s α values for each item when removed are shown in Table 1.
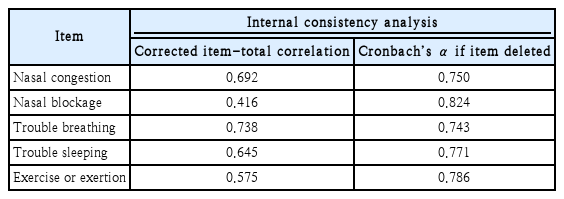
Internal consistency analysis of the K-NOSE scale
The test-retest reliability (reproducibility) analysis of the K-NOSE assessment, conducted at a 2-week interval before surgery in the patient group, is summarized in Table 2. Pearson’s correlation analysis demonstrated significant associations, with coefficients (r) ranging from 0.687 to 0.850 (all p<0.001). Furthermore, the overall ICC values for the K-NOSE ranged from 0.688 to 0.846, indicating acceptable reproducibility of the scale.
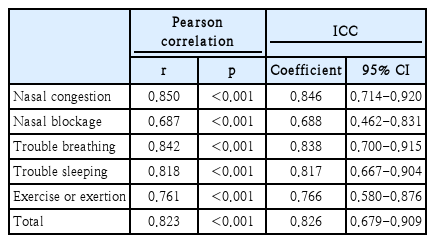
Test-retest reliability of the K-NOSE
Item-item and item-total correlations used to assess construct validity are summarized in Table 3. Each item demonstrated a significant correlation with the total score. However, the “trouble sleeping” and “during exercise or exertion” items showed weak or absent correlations with the “nasal congestion” and “nasal blockage” items.
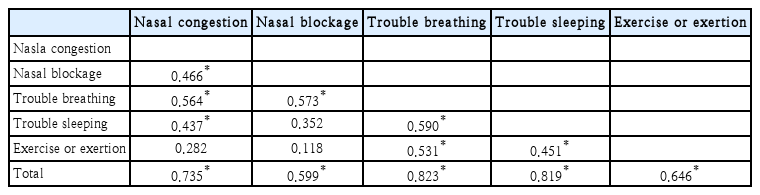
Item-item and item-total correlations of K-NOSE
Table 4 presents the results of the discriminant validity analysis. The K-NOSE scores for the preoperative patient group and the control group were compared using Student’s t-test for each of the five items and the total score. The analysis revealed statistically significant distinctions between the patient and control group for every assessed domain (all five items: p<0.001; total score p<0.001), robustly demonstrating excellent discriminant validity of the instrument.
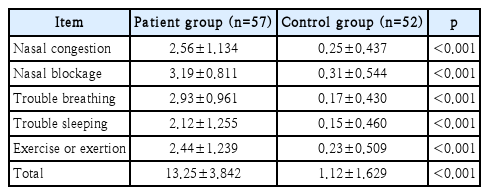
Comparison of the K-NOSE scores between the patient group and the control group
Criterion-related validity was assessed by performing Spearman’s correlation analysis between the K-NOSE and the VAS scores for nasal obstruction. The patient group completed the questionnaires a total of three times: twice preoperatively and once postoperatively. In the patient group, all items and the total score correlated well with the VAS score both preoperatively and postoperatively (all p<0.05). The results are summarized in Table 5.
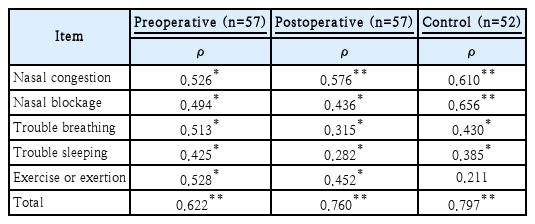
Spearman correlation coefficients between K-NOSE and the VAS
Lastly, responsiveness was evaluated in the patient group by comparing preoperative and postoperative K-NOSE scores using a paired-sample t-test. Statistically significant responsiveness was observed in all items and the total score of the K-NOSE, demonstrating high sensitivity to change (all p<0.001) (Table 6).
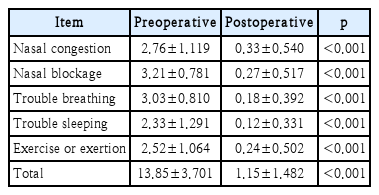
Comparison of preoperative and postoperative K-NOSE scores
Discussion
Nasal obstruction is a symptom that causes significant discomfort to patients and negatively affects their quality of life. The subjective nature and varying severity of nasal obstruction reported by patients make it challenging for physicians to accurately assess. Moreover, evaluating the degree of symptom improvement after surgery is crucial for both the patient and the otorhinolaryngologists.
The NOSE questionnaire enables patients to effectively describe the severity of their nasal obstruction in different situations. This questionnaire is simple and quick to complete, placing minimal burden on patients [5]. Additionally, the NOSE questionnaire has the advantage of assessing postoperative improvement using the same set of items. This study examined the psychometric properties of the K-NOSE questionnaire, developed for Korean-speaking patients.
The internal consistency of the K-NOSE demonstrated an overall Cronbach’s α value of 0.813. According to Stewart, et al. [5], the overall Cronbach’s α coefficient of the original NOSE was 0.785. Various NOSE validation studies in different languages have reported Cronbach’s α values ranging from 0.71 to 0.955 [6-10,12-14,21]. The Cronbach’s α values if each item was deleted are summarized in Table 1. Many previous studies on the NOSE questionnaire have reported only the overall Cronbach’s α, without conducting or presenting analyses of corrected item-total correlations or Cronbach’s α if an item is deleted [7,9-11,15,18,21,22]. This study conducted analyses of corrected item-total correlations and “alpha if item deleted” to enhance the reliability of the questionnaire and to examine the internal consistency among items [27].
Test-retest reliability is determined by administering the same test to the same individuals at two separate times and evaluating the correlation or degree of association between the resulting scores [28]. In this study, the ICC was calculated using a two-way mixed-effects model with absolute agreement and single measurement. Although ICC analyses have been conducted for several language versions of the NOSE questionnaire, the Italian versions demonstrated results comparable to those of this study (ICCs ranged from 0.73 to 0.76) [9,13,16,17,22]. Although Pearson correlation is commonly used, the ICC evaluates both the degree of correlation and agreement between measurements, making it a more suitable metric for assessing test-retest reliability [29].
The original NOSE showed poor correlations with sleep-related items (nasal congestion: r=0.321; nasal obstruction: r=0.386) [5]. Similarly, the Dutch version of the NOSE demonstrated a weak correlation between “trouble sleeping” and “nasal obstruction” items (r=0.36) [9]. Similar findings were observed in this study (Table 3). Given the findings from other language versions, the relatively low correlation between trouble sleeping and nasal obstruction/congestion may be attributed to the multifactorial etiology of sleep disturbances. Sleep problems (trouble sleeping) can arise from various causes, including insomnia, obstructive sleep apnea, and others, which likely weakens their correlation with nasal symptoms. The “Exercise or exertion” item also exhibited no significant correlation with nasal symptoms (Dutch version NOSE nasal congestion: r=0.327; Bahasa Malaysia version NOSE nasal congestion: r=0.39; Malay version NOSE nasal blockage: r=0.31) [9,20]. Consistent with these findings, our study demonstrated a similar pattern (Table 3). Oral breathing during exercise offers enhanced ventilation and CO2 elimination compared to nasal breathing [30]. Therefore, the use of mouth breathing during exercise likely explains the weak correlation with nasal obstruction symptoms.
The discriminant validity of the K-NOSE, as assessed by comparing the patient and control groups, was also excellent (Table 4), consistent with findings from studies conducted in other countries. The responsiveness of the K-NOSE, which measures the ability of the tool to detect changes over time in the construct of interest, also demonstrated excellent statistical significance (all p<0.001) (Table 6).
Criterion-related validity provides evidence of how strongly scores on a new measure correlate with other measures of the same construct or closely related constructs that are theoretically expected to be associated [28]. To evaluate the criterion-related validity of the NOSE, studies in other languages have also examined its correlation with VAS scores for nasal obstruction [5,9,12-14]. In addition to VAS, Mozzanica, et al. [13] used anterior nasal rhinomanometry, while Balsevicius, et al. [8] utilized the SNOT-22 questionnaire to analyze the correlation with the NOSE. In the original, Italian, and Dutch versions of the NOSE, only item four, “trouble sleeping,” showed no statistically significant correlation with the VAS [5,9,13]. Rhinomanometric results also showed a low or non-significant correlation with item four of the Italian NOSE, “trouble sleeping.” [13] In contrast, the Spanish version of the NOSE showed statistically significant correlations with the VAS for all items [14]. Although the Spearman correlation coefficients were lower than those of the Spanish NOSE, this study still exhibited statistically significant correlations with the VAS for all items in the patient group, further supporting its strong criterion-related validity (Table 5).
A limitation of this study is consecutive convenience sampling, which may not fully represent Korean-speaking patients with nasal obstruction. Unlike the original NOSE study, our cohort—similar to other validation studies—included septoplasty and/or inferior turbinoplasty, and septoplasty with nasal valve surgery [9,11,19,21]. This surgical heterogeneity may have affected symptom changes. Additionally, hospital-based controls, despite lacking nasal symptoms, may introduce selection bias by not representing the healthy general population. Finally, age (42.9 years vs. 38.9 years) and sex differences between groups represent another limitation. While Shastri, et al. [31] reported no influence of gender, race, or geography on NOSE scores, age influences symptom severity. Further studies incorporating age-matching may strengthen these findings.
In conclusion, the K-NOSE, like the original NOSE and its versions in other languages, demonstrated reliability, validity, and sensitivity to change. The K-NOSE is a valuable tool for evaluating nasal obstruction symptoms in Korean-speaking patients and for assessing their responses both before and after treatment.
Notes
Acknowledgments
This study was conducted as part of a research project led by the Korean Academy of Facial Plastic and Reconstructive Surgery during 2023-2024.
Author Contribution
Conceptualization: Su Jin Kim, Yeon-Hee Joo. Data curation: Jeon Gang Doo, Su Jin Kim, Yeon-Hee Joo, Woo Ri Choi, So Jeong Kim. Formal analysis: Do Hyun Kim, Shin Hyuk Yoo. Investigation: Su Jin Kim, Hahn Jin Jung. Methodology: Yeon-Hee Joo, Woo Ri Choi. Project administration: Su Jin Kim, Kyu-Sup Cho. Software: So Jeong Kim, Do Hyun Kim. Supervision: Kyu-Sup Cho, Hyo Yeol Kim. Validation: Jeon Gang Doo, Su Jin Kim. Visualization: Shin Hyuk Yoo, Hahn Jin Jung. Writing—original draft: Jeon Gang Doo. Writing—reviwe&editing: Jeon Gang Doo, Kyu-Sup Cho, Hyo Yeol Kim.