Tailored Palatal Surgery in Obstructive Sleep Apnea: The Role of Drug-Induced Sleep Endoscopy in Surgical Decision-Making
폐쇄성 수면 무호흡증 환자들에게 시도되는 Palatal Surgery: 수술방법 선택에서의 약물 유도성 수면내시경의 역할
Article information

Abstract
The surgical treatment of obstructive sleep apnea (OSA) has evolved beyond traditional uvulopalatopharyngoplasty, which often yields inconsistent success reports. This article presents a systematic surgical protocol that tailors the type of pharyngoplasty to fit specific airway collapse patterns identified by drug-induced sleep endoscopy (DISE). In this protocol, all surgical candidates undergo DISE to evaluate the collapse pattern, with a focus on retropalatal circumferential collapse. Based on these findings, patients are selected for one of three procedures: uvuloplasty with soft palatal webbing flap pharyngoplasty for mild cases, relocation pharyngoplasty for moderate cases, or expansion sphincter pharyngoplasty for severe cases. This personalized strategy has been reported with notable improvements in surgical outcomes in appropriately selected patients. This highlights that a one-size-fits-all approach is insufficient and that a surgical strategy guided by a thorough DISE assessment is essential to select the appropriate technique and maximize success in OSA surgery.
Introduction
Obstructive sleep apnea (OSA) involves recurrent upper airway collapse during sleep, which leads to repeated exposure to intermittent hypoxic events, arousals, and sleep fragmentation, thereby worsening sleep quality. Over the long term, these disturbances can also affect mortality through chronic diseases such as cardiovascular disease and disorders of glucose metabolism. OSA is highly prevalent, with mild or worse sleep apnea reported in 38% of the general population, and societal attention to this disease is also increasing [1]. In addition to the organic problems associated with chronic disease, the societal burden is substantial because excessive daytime sleepiness and related symptoms can impair work performance and reduce quality of life. In one study of the US population, the direct costs of diagnosis and treatment and the indirect socioeconomic losses attributable to OSA were reported to reach 1150 billion dollars per year [2]. Positive airway pressure therapy is established as the standard treatment for moderate and severe OSA and benefits many patients, but the need to wear a facial mask continuously during sleep can cause discomfort, and adherence is recognized as a major determinant of success [3]. In outpatient practice, clinicians commonly encounter patients who cannot adapt to positive airway pressure therapy and therefore seek consultation regarding surgical treatment. Multiple surgical options have been reported for such patients, and preferred techniques vary among clinicians. Among these approaches, palatoplasty is one of the most frequently performed procedures by otorhinolaryngologists, yet its efficacy has remained controversial due to conflicting reports in the literature. In particular, uvulopalatopharyngoplasty (UPPP), the most widely performed technique, elevates the soft palate and expands the shape of the pharyngeal arches and has been reported to mainly enlarge the anteroposterior dimension of the oropharyngeal airway, but its reported success rates are inconsistent, and its effectiveness remains a persistent subject of debate [4].
Over the past 20 years, the introduction of drug-induced sleep endoscopy (DISE) has led to major changes in the surgical management of OSA. In patients with relatively severe OSA, airway obstruction due to collapse of the lateral pharyngeal wall has been reported as an important predictor, and when DISE confirms the collapse pattern as lateral pharyngeal wall collapse, effective outcomes require addressing both lateral pharyngeal wall collapse and thickness.
Here, the author aims to share the surgical approaches applied in clinical practice for patients with OSA, along with the protocol guiding procedure selection and the resulting treatment outcomes.
Methods
For preoperative evaluation, the author mandates DISE. Intravenous sedatives are administered, typically midazolam or propofol, to reproduce a sleep state, and upper airway obstruction is assessed endoscopically. This approach allows a detailed assessment according to the site, pattern and degree of obstruction. The velum, oropharynx, tongue base, epiglottis classification reported by Kezirian is the most widely used DISE scoring system, and the author evaluates and reports disease findings using this tool [5-7].
In the author’s prior work, collapse of the lateral pharyngeal wall at the level of the retropharynx, with circular collapse when anteroposterior collapse coexisted, showed a strong association with moderate or worse OSA [8]. Considering that traditional UPPP mainly enlarges the anteroposterior dimension [9], patients with lateral pharyngeal wall collapse may require individualized surgical approaches that address lateral obstruction. The author therefore considers DISE, which enables confirmation of the obstruction pattern, to be a key determinant in selecting surgical procedures.
Uvuloplasty with soft palatal webbing flap pharyngoplasty
In a previous study of 174 patients (mean age 45.1 years, range 15.0-73.0 years; mean body mass index 25.4 kg/m², range 19.1-35.6 kg/m²), the author applied uvuloplasty with soft palatal webbing flap pharyngoplasty in patients who met all of the following criteria: 1) an apnea hypopnea index (AHI) of at least 5 per hour, 2) circular collapse of the retropharynx of grade 1 or lower on DISE, 3) lateral wall collapse attributable to soft-tissue volume around the palatopharyngeal arch, and 4) bilateral tonsillar hypertrophy of grade 2 or lower. In that report, postoperative polysomnography (PSG) metrics improved in 71% of patients, and the reported surgical success rate was 42% [10].
Because this procedure is relatively simple and less invasive, the author also applies it selectively, even in patients with severe OSA who avoid oropharyngeal surgery due to pain or fear, when positive airway pressure therapy is planned (Table 1).
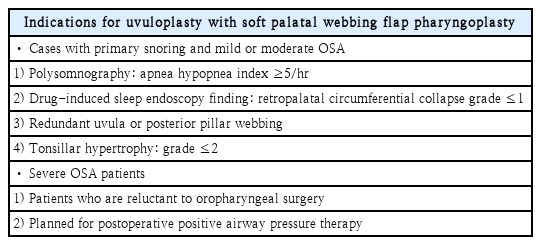
Indications for uvuloplasty with soft palatal webbing flap pharyngoplasty
The operative technique is based on the study reported by Elbassiouny [11]. Mucosa associated with pharyngeal webbing is dissected starting from the most superior aspect and continuing to the superior tonsillar level to expose the muscle fibers of the palatopharyngeus (PP). Incisions are made from the uvula and the palatopharyngeal arch to create a single mucosal flap, which is then trimmed to a size of 4-5 mm. The medially and laterally created flaps are sutured with Vicryl 3.0 to the lateral aspect of the oropharynx while maintaining appropriate tension. The shortened mucosal flap is also sutured to cover the exposed soft palate. To minimize postoperative foreign-body sensation, the knot is oriented toward the nasopharyngeal direction. This procedure is repeated bilaterally, and the operation is completed with uvulopharyngoplasty (Fig. 1) [11].
Main surgical steps in soft-palate webbing flap pharyngoplasty. A: Incision line for dissection of soft-palate webbing layers was determined. B: Dissection of soft-palate webbing layers with removal of the oropharyngeal layer and creation of two flaps. C and D: The dissected nasopharyngeal layer of palate webbing (asterisk) and the posterior pillar flap (arrow) turned up to cover the free edge of the newly formed soft palate with Vicryl #3.0. E: The same procedure is performed on the other side. F: Uvulopalatal flap was carried out as the last step of the soft-palate webbing flap pharyngoplasty procedure and mucosal closure was performed. Pre- (G) and postoperative (H) findings of soft-palate webbing flap pharyngoplasty. Adapted from Park, et al. Sleep Breath 2022;26(4):1963-71 [10].
In previously published data, this technique showed the greatest effectiveness in patients with primary snoring with an AHI of less than 5 per hour and in patients with mild or moderate OSA who showed circular collapse of grade 1 or lower on DISE [10]. The author applies this approach selectively in such patients.
Relocation pharyngoplasty
In the author’s previously published data, 62.6% of patients with moderate or worse OSA demonstrated circular collapse at the level of the retropharynx. Lateral pharyngeal wall collapse was also associated with relatively higher AHI and a higher number of respiratory disturbance index events [8]. Without addressing the lateral wall, applying UPPP alone in such patients could be expected to yield unfavorable outcomes. The author therefore stratifies severity according to DISE and PSG findings and applies relocation pharyngoplasty and expansion sphincter pharyngoplasty (ESP).
Relocation pharyngoplasty is applied when tonsillar hypertrophy is grade 2 or higher, when a low lying soft palate and a large soft-tissue volume around the palatopharyngeal arch are present and when DISE shows circular collapse of grade 1 or higher (Table 2). This procedure is based on the surgical technique developed by Li and Lee [12]. Tonsillectomy and uvulopalatal flap are performed first. An incision line is determined on the mucosa above the uvula using a marking pen, and only the mucosa is removed with a Bovie or sharp pointed scissors to minimize injury to the uvular muscle. Excess residual uvular tissue is excised, then folded upward onto the soft palate and sutured.
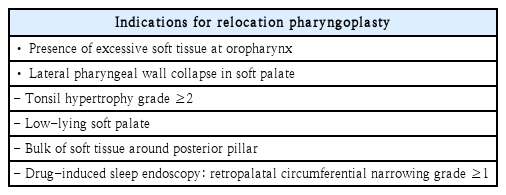
Indications for relocation pharyngoplasty
The PP muscle is separated from the superior pharyngeal constrictor muscle (SPC) and the palatopharyngeal arch so that the palatopharyngeal arch can be elevated without additional tension. Using Vicryl 2.0, the PP muscle is elevated toward the cephalic and lateral directions to the palatal flap, and the SPC muscle is elevated to the ipsilateral palatoglossus (palatoglossus) with mattress sutures in a cephalic to caudal direction. The mucosa of the palatopharyngeal arch and the palatoglossal arch is closed with Vicryl 3.0 (Fig. 2) [13].
Main surgical steps of the relocation pharyngoplasty. A: After completion of tonsillectomy, the palatopharyngeus (PP) muscle (red arrow) is identified. B: PP muscle is dissected from posterior pillar including mucosa and submucosal adipose tissue. C: The PP muscle is rotated cephalad and laterally to approach the anterior pillar. Absorbable suture is used to fix the PP muscle at the anterior pillar and two-point sutures are performed with Vicryl #2.0. D: View of the PP muscle anchored to the anterior pillar. E: Mucosal closure with Vicryl #3.0 and the same procedure performed on the contralateral side. F: Final appearance of the pharynx after completion of the surgery. Adapted from Oh, et al. Sci Rep 2020;10(1):2101 [13].
In a prior study of 133 patients (mean age 43.4 years, range 21-56 years; mean body mass index 26.6 kg/m², range 16.0-34.2 kg/m²), PSG performed 6 months after surgery showed that the mean preoperative AHI decreased from 35.0±20.7 per hour to 21.4±17.6 per hour. When “success” was defined as a postoperative AHI of less than 20% with a reduction of at least 50%, the success rate was 52.9%. When “improved” was defined as a reduction of at least 50% regardless of the postoperative value, the proportion classified as improved and success was 69.1%. In particular, among patients with circular collapse at the level of the retropharynx, success was 69.1% in those with moderate OSA [13].
Expansion sphincter pharyngoplasty
ESP includes transection of the PP muscle, which makes it more invasive than the prior procedure, but it can provide greater lateral expansion for the lateral pharyngeal wall. Accordingly, the author applies ESP in patients with tonsillar hypertrophy of grade 2 or higher and a large soft-tissue volume of the palatopharyngeal arch and the lateral pharyngeal wall, and particularly when DISE shows grade 2 obstruction due to circular collapse at the retropharyngeal level (>75% obstruction) (Table 3).
Indications for expansion sphincter pharyngoplasty
This procedure is based on the paper published by Pang and Woodson [14]. As described above, tonsillectomy is performed and UPPP is performed. The PP muscle is identified and resected horizontally at the midportion, and the superior half is dissected from the SPC muscle and separated. The separated segment is rotated superolaterally and fixed to the pterygomandibular raphe with mattress sutures using Vicryl 2.0. The mucosal flaps are closed using Vicryl 3-0, and the procedure is performed (Fig. 3) [15].

Main surgical steps of the expansion sphincter pharyngoplasty (ESP). A: After completion of tonsillectomy, the palatopharyngeus (PP) muscle (white asterisk) is identified. B: A horizontal incision is made to divide the inferior end of the PP muscle (white asterisk), with care taken to leave its fascia attachments to the deeper horizontal constrictor muscle. C: Absorbable suture is used to fix the PP muscle to the pterygomandibular raphe (white arrowhead) through a mucosal tunnel (yellow arrowhead) at the anterior pillar. D: Mucosal closure is performed, and ESP creates tension in the lateral pharyngeal wall. Adapted form Hong, et al. JAMA Otolaryngol Head Neck Surg 2019;145(5):405-12 [15].
In the author’s prior study of 63 patients (mean age 42.1 years, range 20-54 years; mean body mass index 27.6 kg/m², range 19.0-32.1 kg/m²), patients who underwent ESP showed a decrease in mean preoperative AHI from 35.5 to 17.3 after surgery (mean difference 18.1; 95% confidence interval, 16.3-20.0). Mean lowest oxygen saturation during sleep also improved from 78.2% to 86.4%. When patients were classified into the Success group as described above, the surgical success rate was 68.2% [15].
Discussion
Since Ikematsu first introduced UPPP [16], upper airway surgery for patients with OSA has undergone substantial changes over the past 50 years. Skepticism toward surgical treatment represented by UPPP have persisted and reported surgical success rates for UPPP vary from 36%-78%. This variability has, in turn, required sleep surgeons to re-examine indications for surgery and to pursue additional understanding and research on upper airway collapse [17-19].
Following the introduction of DISE, understanding of sleep-related upper airway collapse in OSA has changed considerably over the past 20 years, and attempts to incorporate DISE into the process of developing treatment strategies to improve outcomes have been reported. In a meta-analysis reported by Qi, et al. [5], persistently high failure rates in DISE-guided treatment planning were attributed not only to patient-related factors and disease complexity but also to examiner subjectivity, which may prevent assurance of inter-observer reliability, and to the absence of guidelines for selecting procedures based on DISE findings.
In response to these limitations, the author considers it essential to include DISE performed according to a shared protocol among examiners when selecting surgical strategies for patients with OSA and further considers standardizing treatment plans into a protocol according to the principles described above to be an important factor that can increase surgical success rates. Because many reports present circular collapse that includes lateral pharyngeal wall collapse as a major predictor of surgical failure, the author considers it necessary to confirm the obstruction pattern through DISE before establishing a surgical plan and, when lateral wall collapse is present, to include procedures that improve lateral wall collapse.
Criticisms of surgical treatment for OSA in earlier eras may largely reflect the limitation that real-time upper airway collapse during sleep could not be assessed, as is possible with DISE. In the current setting, where DISE is available as a diagnostic approach for clinicians, the author proposes that active use of DISE to implement individualized treatment can clarify and reinforce the role of surgery in the management of OSA.
Supplementary Materials
Korean translation of this article is available with the Online-only Data Supplement at https://doi.org/10.3342/kjorl-hns.2025.00458.
Notes
Acknowledgments
None
Author Contribution
Conceptualization: Hyun Jik Kim. Writing—original draft: Dongyoung Kim. Writing—review & editing: Hyun Jik Kim.