Effect of Exhalation Delivery System With Fluticasone for Chronic Rhinosinusitis: A Systematic Review and Meta-Analysis
만성 비부비동염에 대한 플루티카손 흡입 전달 시스템의 효과: 체계적 문헌 고찰 및 메타 분석
Article information

Abstract
An exhalation delivery system for fluticasone (EDS-FLU) is designed to deposit drug into sinonasal regions above the inferior turbinate, particularly sinus drainage pathways not reached by standard nasal steroid sprays. We evaluated the efficacy and safety of EDS-FLU for chronic rhinosinusitis (CRS). We reviewed four independent randomized controlled trials derived from three published articles identified through searches of PubMed, Embase, SCOPUS, Google Scholar, Web of Science, and the Cochrane Library up to April 2024. Outcomes included 22-item Sinonasal Outcome Test (SNOT-22) scores, nasal symptom scores, nasal polyp scores, patient global impression of change (PGIC), responder and surgical indication rates, and adverse events. Compared with EDS-placebo, EDS-FLU produced greater reductions in nasal polyp scores and SNOT-22 scores over 6 months. At 3 months, nasal congestion, facial pain, rhinorrhea, and olfactory dysfunction improved more with EDS-FLU, and PGIC responder and complete response rates were higher at 3 and 6 months. EDS-FLU reduced surgical indication and increased overall responder rates at 3 months but not at 6 months. Epistaxis and nasal septal erosion or ulceration occurred more frequently with EDS-FLU, whereas rates of headache, nasal congestion, nasopharyngitis, and upper respiratory infection were similar between groups. EDS-FLU provides clinically meaningful improvements in subjective and objective outcomes in CRS but is associated with an increased risk of local nasal adverse events, warranting individualized risk-benefit assessment.
Introduction
Chronic rhinosinusitis (CRS) is a prevalent chronic inflammatory disease with a global prevalence of 5%-12% [1,2]. Patients with CRS often experience low quality of life (QoL) and frequent antibiotic prescriptions and surgery [3]. CRS can cause abnormal mucociliary clearance, ventilation, and drainage issues in the paranasal sinuses, leading to nitric oxide level changes [4]. CRS symptoms include persistent nasal obstruction, decreased sense of smell, rhinorrhea, and facial discomfort [5]. CRS has subtypes with and without nasal polyps. These polyps can worsen sinus inflammation by blocking sinus drainage and affecting airflow [6,7].
Maintenance treatment for CRS involves controlling inflammation to improve the QoL and reduce symptoms [6,8]. Shortterm treatment with systemic steroids can improve symptoms and reduce nasal polyp size, but symptoms may recur after discontinuation, and systemic adverse effects may occur from long-term use [9,10]. Therefore, a safer, topical steroid nasal spray is considered the first-line treatment for CRS and recurrence after endoscopic sinus surgery [5,8]. However, this treatment is more effective for CRS with nasal polyps than without nasal polyps, and the efficacy of standard-delivery nasal steroid sprays is minimal and does not yield satisfactory results [8,11].
The standard-delivery nasal steroid sprays do not allow drugs to accumulate in the superior and posterior parts of the nasal cavity, where the osteomeatal complex and sinus drainage tract are located [12-14]. Effective delivery and accumulation of drugs in the distal portion, such as the upper part of the inferior turbinate, is helpful for treating CRS [13]. Nasal irrigation using high-dose steroids has been attempted to approach the paranasal sinus, where steroids cannot reach, but its safety and effectiveness are uncertain [15]. If CRS cannot be treated because steroids cannot reach the paranasal sinus sufficiently, endoscopic sinus surgery may be used to help the drug reach the sinus orifice [8,16]. However, additional surgery may be necessary in cases of recurrence, and local drug treatment is often continued as adjuvant therapy [5,8].
An exhalation delivery system with fluticasone (EDS-FLU) is a new method of closing the soft palate and delivering fluticasone bidirectionally, resulting in much more efficient intranasal steroid deposition than conventional standard-delivery nasal steroid sprays [17]. Fluticasone is a powerful corticosteroid with low bioavailability [17]. EDS-FLU can deliver sufficient fluticasone to the superior and posterior parts of the nasal cavity by passing through the front of the inferior turbinate, allowing the drug to effectively reach the sinus drainage tract [13,18]. Previous studies on the effect of delivering fluticasone via an EDS with other devices also reported effectiveness in improving CRS symptoms [19,20]. Among the conservative care methods for CRS, EDS-FLU is one of the few drug treatments approved by the Food and Drug Administration [8]. Few studies have confirmed the efficacy of EDS-FLU in improving symptoms and inflammatory conditions in patients with CRS [17,21,22]. To the best of our knowledge, this is the first systematic review and meta-analysis analyzing the effect of EDS-FLU on CRS.
Materials and Methods
This review was planned and reported following Preferred Reporting Items Guidelines for Systematic Review and Meta-Analysis (PRISMA). We registered the protocol prospectively on the Open Science Framework (OSF; https://osf.io/gqvpk/).
Literature search and study selection
We prespecified eligibility using a Population, Intervention, Comparison, Outcomes, and Study (PICOS) framework. Adults (≥18 years) with CRS and nasal polyps were included. The intervention was EDS-FLU administered twice daily (186 μg or 372 μg) during the study period, and comparators included device-matched placebo where applicable. Outcomes of interest covered 1) symptom domains (congestion, facial pain/pressure, rhinorrhea/discharge), 2) disease-specific QoL (Sino-Nasal Outcome Test-22, SNOT-22), 3) patient global improvement (PGIC), 4) endoscopic nasal polyp scores, 5) responder-based endpoints, 6) surgery-related eligibility/indication, and 7) adverse events. Where outcome definitions varied across trials, we first extracted the original definitions used by each study (e.g., endoscopic grading anchors, responder thresholds, complete-response criteria, and surgicaleligibility criteria). Harmonization was then performed by pooling only conceptually comparable endpoints at matched follow-up time points. Continuous outcomes were combined only when the same named instrument or symptom scale was used across studies, whereas dichotomous outcomes were synthesized as odds ratios (ORs) after preserving each trial’s original threshold or anchor. Accordingly, responderbased and surgery-related pooled estimates should be interpreted as harmonized cross-trial constructs rather than strictly identical endpoints. We restricted inclusion to randomized controlled trials published in English. We searched PubMed, Embase, SCOPUS, Google Scholar, Web of Science, and the Cochrane Library for studies available through April 2024 using terms related to CRS with nasal polyps, EDS-FLU/fluticasone, symptom/QoL instruments (e.g., SNOT-22, PGIC), and endoscopic outcomes.
An experienced medical librarian conducted the database searches, and we also screened reference lists of relevant articles to identify any additional eligible trials. Two reviewers independently screened titles/abstracts and then assessed full texts when eligibility was unclear from the abstract. Disagreements were resolved by discussion, with a third reviewer arbitrating when needed. We excluded studies with concomitant systemic corticosteroid use during the intervention period and those lacking extractable quantitative outcome data. The screening and selection process is shown in Fig. 1.
Study selection diagram.
Data extraction and risk of bias appraisal
We extracted data using a prespecified template [23], including sample size, dose, follow-up duration, and baseline characteristics, along with all outcomes of interest [17,21,22]. Patient-reported outcomes included symptom domain scores, SNOT-22, and PGIC; clinician-reported outcomes included endoscopic polyp grades. We also collected study-specific definitions for responder status, complete response, and surgery-related eligibility/ indication outcomes, together with EDS-FLU-related adverse events, so that conceptually aligned endpoints could be synthesized while preserving the original trial-level criteria. When studies reported between-group comparisons, we extracted the corresponding effect measures and dispersion statistics to evaluate both efficacy and safety.
Statistical analyses
All quantitative analyses were performed in R (version 4.3.1; R Foundation for Statistical Computing). In the case of quantitative variables, the meta-analysis was conducted using the mean difference (MD). This method was selected to analyze the patients’ grading of symptoms and QoL scores, as well as polyp grades by clinicians, because no single standardized scale was used in all studies. The OR was calculated for the responder and complete responder rates and adverse effects related to EDS-FLU. Heterogeneity was calculated using the I2 test, which describes the rate of variation across studies due to heterogeneity rather than probabilistic chance. The measures ranged from 0 (no heterogeneity) to 100 (maximum heterogeneity). We report effect estimates with 95% confidence intervals (CIs), using two-sided p values throughout. When significant heterogeneity among outcomes was found (defined as I2 >50), the random-effects model, accord-ing to DerSimonian-Laird, was used. Under the random-effects framework, we allowed the underlying true effects to vary across studies and assumed these study-level effects follow an approximately normal distribution.
We performed subgroup analyses where appropriate, including dose-based comparisons (186 μg vs. 372 μg) when data were available. For outcomes with low heterogeneity (I2 <50%), pooled estimates were derived using a fixed-effect inverse-variance method.
Potential small-study effects were examined using funnel plots and Egger’s regression. When asymmetry was suggested, we explored the impact of publication bias using the trimand-fill method. Robustness was further evaluated with leaveone- out influence analyses to determine whether any single study materially altered the pooled estimates.
Results
Three published articles comprising four randomized controlled comparisons and 1201 participants (Palmer et al.’s study included two separate randomized controlled studies [ReOpen1 and ReOpen2]) were included for this meta-analysis. Key study characteristics are summarized in Table 1. All included randomized trials were judged to be at low risk of bias across the assessed domains, including random sequence generation, allocation concealment, blinding of participants and outcome assessors, completeness of outcome data, and selective reporting; detailed domain-level assessments are provided in Supplementary Table 1.
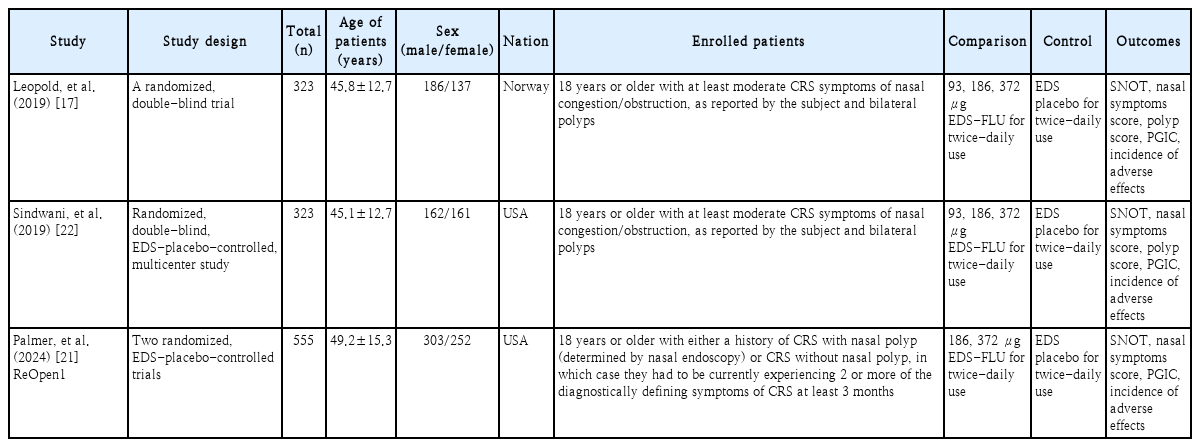
Summary of included studies
Effect of EDS-FLU on subjectively reported outcomes and clinically observed grades compared with the control group
Fig. 2 shows that after 3 months (MD -8.9811, 95% CI [-11.1230; -6.8393], I2=0.0%) and 6 months (MD -5.3347, 95% CI [-7.9059; -2.7635], I2=56.6%) SNOT-22 scores were significantly reduced in the treated group compared to the control group. In individual nasal symptoms, nasal congestion {after 1 month (MD -0.3903, 95% CI [-0.4218; -0.3589], I2=0.0%) and 3 months (MD -0.3657, 95% CI [-0.4652; -0.2662], I2=69.8%)}, facial pain {after 1 month (MD -0.2225, 95% C I [-0.2474; - 0.1975], I 2=0.0%) a nd 3 m onths ( MD -0.1545, 95% CI [-0.2442; -0.0648], I2=73.4%)}, olfactory dysfunction {after 1 month (MD -0.1800, 95% CI [-0.2248; -0.1353], I2=62.8%) and 3 months (MD -0.2660, 95% CI [-0.3214; -0.2107], I2=55.1%)}, and rhinorrhea {after 1 month (MD -0.3429, 95% CI [-0.4008; -0.2851, I2=59.6%) and 3 months (MD -0.2974, 95% CI [-0.3757; -0.2191], I2=58.0%)} in the treated group were significantly improved compared to the control group.
Administration of EDS-FLU vs. EDS-placebo: mean difference of 22-item Sinonasal Outcome Test scores after 3 months (A) and 6 months (B), nasal congestion after 1 month (C) and 3 months (D), facial pain after 1 month (E) and 3 months (F), olfactory dysfunction after 1 month (G) and 3 months (H), and rhinorrhea after 1 month (I) and 3 months (J).
As shown in Fig. 3, EDS-FLU significantly decreased the size of nasal polyps {polyp score after 3 months (MD -0.6543, 95% CI [-0.7906; -0.5179], I2=0.0%) and 6 months (MD -0.4657, 95% CI [-0.6108; -0.3205], I2=0.0%)} compared to the control group. In polyp size, the responder (OR 2.6508, 95% CI [2.0215; 3.4760], I2=0.0%) and complete responder rates after 3 months (OR 2.0843, 95% CI [1.3506; 3.2166], I2=0.0%) and 6 months (OR 1.8881, 95% CI [1.1184; 3.1875], I2=56.8%) also increased and the surgical eligibility rate significantly decreased after 3 months (OR 0.4978, 95% CI [0.3683; 0.6728], I2=0.0%) in the EDS-FLU group versus the control group. However, there were no significant differences in the responder (OR 1.1686, 95% CI [0.8698; 1.5699], I2=0.0%) or surgical eligibility rate (OR 0.8583, 95% CI [0.6076; 1.2123], I2=0.0%) after 6 months between the treated and control groups.
Administration of EDS-FLU vs. EDS-placebo: mean difference of polyp score after 3 months (A) and 6 months (B) and odds ratios of responders after 3 months (C) and 6 months (D), complete responders after 3 months (E) and 6 months (F), and surgical eligibility rate after 3 months (G) and 6 months (H).
As shown in Fig. 4, patients who used EDS-FLU reported positive treatment efficacy during the enrolled periods (much or very much improved status in patient global impression of change (PGIC) scores after 3 months (OR 3.5066, 95% CI [2.6629; 4.6177], I2=0.0%) and 6 months (OR 1.8511, 95% CI [1.1310; 3.0298], I2=77.2%) compared to the control group.
Administration of EDS-FLU vs. EDS-placebo: odds ratio of much or very much improved state in patient global impression of change scores after 3 months (A) and 6 months (B).
The Egger test and Begg funnel plot analyses for all nasal symptoms (p>0.05) revealed no publication bias in the included studies. Begg funnel plots and the Egger linear regression test were not conducted for the other outcomes because of the small number of included studies (<10).
Substantial between-study heterogeneity (I2 >50%) was observed for several outcomes. Because the primary figures present overall pooled effects, dose-stratified estimates for 93 μg, 186 μg, and 372 μg were summarized separately in Supplementary Tables 2-4. Although point estimates numerically tended to favor the higher-dose groups for several endpoints, formal between-dose comparisons were not statistically significant for most outcomes. The only significant subgroup difference was observed for olfactory dysfunction at 3 months (p-value for subgroup difference=0.0221), indicating that the present data do not support a consistent dose-response relationship across efficacy outcomes.
Taken together, the publication-bias assessment and subgroup analysis suggest that EDS-FLU may improve both patient-reported outcomes and clinician-assessed disease severity in CRS.
Effect of EDS-FLU on adverse effects compared with the control group
As shown in Fig. 5, EDS-FLU treatment did not significantly increase the incidence of headache (OR 1.3778, 95% CI [0.7823; 2.4264], I2=0.0%), nasal congestion (OR 1.1698, 95% CI [0.6020; 2.2732], I2=0.0%), nasopharyngitis (OR 0.9152, 95% CI [0.5691; 1.4719], I2=0.0%), or upper respiratory infections (OR 0.5137, 95% CI [0.2299; 1.1477], I2=0.0%) compared with the control group. However, EDS-FLU treatment led to significant epistaxis (OR 4.1646, 95% CI [2.2223; 7.8042], I2=27.7%) and nasal septal mucosal erosion or ulcerative lesions (OR 2.5663, 95% CI [1.2731; 5.1728], I2=0.0%) compared with the control group.
Administration of EDS-FLU vs. EDS-placebo: odds ratio of incidence of headache (A), nasal congestion (B), nasopharyngitis (C), upper respiratory infection (D), epistaxis (E), nasal septal mucosal erosive or ulcerative lesion (F).
Sensitivity analysis
In leave-one-out analyses, the direction and magnitude of the pooled effects were materially unchanged, indicating no single study drove the findings.
Discussion
In this study, we reported that the continuous administration of EDS-FLU for CRS patients significantly reduced polyp scores and nasal symptoms for 6 months compared to the control group. EDS-FLU treatment also improved nasal congestion, facial pain, olfactory dysfunction, and rhinorrhea. The number of patients with improved PGIC scores and complete responders until 6 months increased after using EDSFLU. EDS-FLU treatment significantly improved subjective and objective outcomes compared to the control group but also revealed potential adverse effects, such as epistaxis, nasal septal erosion, and ulcerative lesions.
The standard-delivery nasal steroid sprays are relatively safe, inexpensive, and easy to use, so they are often used as initial treatment in patients with CRS with nasal polyps [21]. However, regardless of the presence or absence of nasal polyps, these sprays often fail to provide adequate symptom relief for CRS patients, and evidence of their effectiveness is insufficient [11]. Standard-delivery nasal steroid sprays are not effective in delivering steroids targeting the osteomeatal complex in the middle meatus [24-26]. In addition, nasal polyps can cause problems with ventilation and drainage of the sinus, block airflow in the nasal cavity, worsen nasal congestion, and make it difficult to deliver drugs using a standard-delivery nasal steroid spray. Nasal polyps also generate inflammatory cytokines, which worsen chronic inflammation in the nasal cavity and make treatment difficult [7]. Even if the nasal polyp grade is improved, the effect of existing steroid sprays is minimal [27,28].
EDS-FLU is a device that can effectively deliver drugs to the deep paranasal sinuses, which are not easily accessible by standard-delivery nasal steroid sprays. EDS is useful because it uses a unique mechanism that stably and consistently delivers steroids bi-directionally to the superior and posterior parts of the nasal cavity [29]. Drug delivery is efficient as less drug is lost to the anterior and posterior areas. Standard-delivery nasal steroid sprays allow the drug to easily reach large polyps exposed at the bottom or front of the nasal cavity. However, it is difficult for the drug to reach nasal polyps when they degenerate into an osteomeatal complex that interferes with sinus drainage and ventilation [27]. EDS-FLU is also easy to use, and more than 80% of patients were reported to recognize it as easy and convenient to use [29]. The EDS device itself may exert a beneficial effect on CRS. When using the EDS device, the inflow of carbon dioxide causes a decrease in the pH of the nasal mucosa, which can have a positive effect on allergic rhinitis [30]. Carbon dioxide can affect inflammatory mediators and neuropeptide activity [31]. The removal of nitric oxide, vibration, and positive air pressure provided by the EDS device may also have an effect [21,22].
Therefore, in patients with CRS who use standard-delivery nasal steroid sprays as initial treatment but are ineffective, EDS-FLU can be considered a stepwise treatment method before endoscopic sinus surgery [21]. While there is insufficient evidence that standard-delivery nasal steroids reduce acute exacerbations of CRS, EDS-FLU has been reported to reduce acute exacerbations of CRS by up to 66% [32,33]. Antibiotics are widely used to prevent acute exacerbations of CRS, but they can adversely affect long-term outcomes due to drug side effects and changes in the microbial community. EDS-FLU, a non-surgical treatment that reduces acute exacerbations of CRS, can reduce the use of antibiotics and improve the QoL of CRS patients. EDS-FLU may be particularly u seful in maximizing the benefits of topical treatment for CRS before endoscopic sinus surgery or other expensive treatment options. Previous studies support the effectiveness of EDSFLU in treating CRS and preventing acute exacerbations of CRS [17,19-22,29].
In dose-stratified analyses, higher doses of EDS-FLU showed numerically larger effect estimates for several outcomes; however, most between-dose comparisons were not statistically significant, and the available evidence was insufficient to establish a consistent dose-response relationship. A significant subgroup difference was observed only for olfactory dysfunction at 3 months, and this isolated finding should be interpreted cautiously. A 372 μg dose of fluticasone is similar to the dose approved in the European Union [29]. At the maximum recommended dosage, EDS-FLU was usually well tolerated and showed a safety profile comparable to earlier intranasal corticosteroids that were investigated for comparable lengths of time in comparable populations [34]. However, considering that the dose is higher than that of standard-delivery nasal steroid sprays, such as mometasone [35], and that there was no significant difference in symptom improvement other than olfactory dysfunction, there is no need to necessarily consider only high doses of EDS-FLU. In CRS patients with no significant improvement in olfactory dysfunction or with low overall symptom scores despite maintaining EDS-FLU for more than 1 month, actively considering a high dose of EDS-FLU of 372 μg is recommended.
Although the adverse effects of EDS-FLU were reported in previous studies [17,21,22,29,31], they are similar to those of standard-delivery nasal steroid sprays, which deliver steroids only to the front and bottom of the nasal cavity and are evaluated to be sufficiently safe [21]. Epistaxis and mucosal erythema or ulceration are local reactions and may also occur when using other nasal sprays [28,36]. I n addition, because patients have a history of sinus surgery prior to EDS-FLU treatment, it may be difficult to reasonably determine the causal relationship between EDS-FLU and local adverse effects.
Several limitations of this review should be acknowledged. Most importantly, the quantitative synthesis was based on only three published articles comprising four randomized comparisons. Although the included trials were methodologically sound overall, internal validity alone cannot offset the limited size of the available evidence base. Therefore, the present findings should be interpreted cautiously and confirmed in additional independent trials. Dose-response inference was also limited because the number of studies contributing to each subgroup was small and the review was not powered to detect modest between-dose differences with confidence.
In addition, the acute exacerbation rate of CRS may be different in the patients who are diagnosed with different upper respiratory tract infections. The effects of EDS-FLU treatment may be reported differently. Moreover, long-term follow-up studies comparing EDS-FLU with existing standard-delivery nasal steroid sprays are needed. Another limitation is that EDS-placebo may not be an appropriate control group. Because the EDS device itself may have positive effects, the symptoms of CRS patients also improved in the control group using a placebo. Since saline irrigation may have a therapeutic effect in CRS, an appropriate control group should be considered. Fourth, other antihistamines or anti-leukotriene agents may have been used previously. Fifth, the length of time the patients with CRS studied previously used steroids or the number of sinus surgeries may have varied. Further studies, such as a standard-delivery nasal steroid spray study in relatively healthy patients with allergic rhinitis, are needed to narrow the study population. Sixth, the included participants were heterogeneous, consisting of an all-inclusive CRS group, CRS with nasal polyps group, and CRS without nasal polyps group. EDS-FLU improved overall symptom scores and nasal polyps in the CRS group with nasal polyps but not in the CRS group without nasal polyps [21]. Standard-delivery nasal steroid sprays also showed mild benefits in CRS patients without nasal polyps, so these should be considered an option or if rhinitis symptoms are present [8,32,37]. However, previous studies reported that CRS patients without nasal polyps showed improvements in individual symptoms, like nasal congestion and facial pain, and improved disease-specific QoL and PGIC scores [21]. Furthermore, responder status, complete response, and surgical indication were not defined identically across trials; although we harmonized only conceptually comparable endpoints, residual definitional heterogeneity may have influenced the pooled dichotomous estimates. Lastly, because the primary goal of CRS treatment is to improve the patient’s symptoms and QoL, it is not necessary to check computed tomography scan. However, in addition to patientreported improvements, it would be helpful to include more studies comparing CT to objectively confirm whether sinus inflammation has decreased.
In conclusion, EDS-FLU, delivered through a novel exhalation delivery system for CRS, significantly reduced polyp scores and improved nasal symptom-related outcomes over 6 months compared with the control group. EDS-FLU treatment also showed improvements in nasal congestion, facial pain, olfactory dysfunction, and rhinorrhea compared to the control group. EDS-FLU treatment also increased the number of patients with improved PGIC scores and the number of complete responders after 3 and 6 months. However, the beneficial effect was not consistently sustained across all responder-based or surgery-related endpoints at 6 months. The study found a higher incidence of epistaxis and nasal septal erosion or ulcerative lesions compared to the control group. Therefore, although EDS-FLU was associated with statistically significant improvements in several subjective and objective outcomes compared with EDS-placebo, these findings should be interpreted with caution given the limited number of available randomized trials, the modest evidence base, and the potential for imprecision in pooled estimates.
Supplementary Materials
Notes
Acknowledgments
None
Institutional Review Board Statement
An ethics statement is not applicable because this study is based exclusively on published literature.
Informed Consent Statement
Informed consents were not required because this study is based exclusively on published literature.
Data Availability Statement
The raw data of individual articles used in this meta-analysis are included in the main text or Supplementary Data. Further enquiries can be directed to the corresponding author.
Author Contribution
Conceptualization: Se Hwan Hwang. Data curation: Se Hwan Hwang, Min Su Kim. Formal analysis: Gulnaz Stybayeva, Yun Jin Kang. Investigation: Se Hwan Hwang. Methodology: Se Hwan Hwang. Project administration: Se Hwan Hwang. Resources: Se Hwan Hwang. Software: Se Hwan Hwang, Min Su Kim. Supervision: Se Hwan Hwang. Validation: Se Hwan Hwang. Visualization: Se Hwan Hwang. Writing—original draft: Se Hwan Hwang, Min Su Kim. Writing—review & editing: Min Su Kim.