Current Outcomes and Implications of Transoral Robotic or Endoscopic Thyroidectomy Versus Open Thyroidectomy
Article information

Abstract
Robotic and endoscopic thyroidectomy, including transoral vestibular approaches, has emerged as an alternative to conventional open thyroidectomy for patients who prioritize avoidance of a visible cervical scar. This review summarizes contemporary evidence comparing minimally invasive robotic and endoscopic thyroidectomy with the transcervical approach, focusing on clinical outcomes, safety, and complication profiles. Across large series, comparative cohorts, and recent meta-analyses, major postoperative outcomes appear broadly comparable between approaches for appropriately selected diseases, including rates of transient and permanent recurrent laryngeal nerve dysfunction, transient hypocalcemia, permanent hypoparathyroidism, postoperative hematoma, and surgical site infection. Minimally invasive approaches consistently deliver superior cosmetic satisfaction and may improve early postoperative quality-oflife measures, while typically requiring longer operative times and a dedicated learning curve. Approach-specific events include transient lower lip or chin sensory changes related to mental nerve irritation in transoral techniques, which most often improve over weeks to months when vestibular incisions and flap elevation remain within established safety zones. Rare but serious complications, including carbon dioxide embolism, have been reported, underscoring the importance of strict insufflation protocols and vigilant intraoperative monitoring. Overall, robotic and endoscopic thyroidectomy can provide a safe and effective option with strong patient-centered benefits when performed by experienced teams and applied to well-defined indications.
Introduction
Conventional open thyroidectomy via a neck incision has long been the standard surgical treatment for thyroid diseases [1]. While effective, the transcervical approach inevitably leaves a visible neck scar that many patients find cosmetically undesirable. In response, surgeons have developed “remote access” techniques to avoid neck scarring, such as endoscopic thyroidectomy via transaxillary or retroauricular (postauricular) approaches [2,3]. These alternative routes relocate incisions to less conspicuous areas (e.g. under the arm or behind the ear), offering improved cosmetic outcomes at the cost of more extensive dissection and limited visualization of contralateral structures.
Robotic/endoscopic thyroidectomy has emerged in the last decade as a truly scarless thyroidectomy technique, entering through the oral vestibule (inner lower lip) and leaving no cutaneous scar [4]. First reported by Anuwong and colleagues [5], the transoral approach gained rapid popularity for its superior cosmetic result and direct midline access to the thyroid gland. Patients motivated to avoid a neck scar, especially younger individuals or those prone to keloids, have driven increased adoption of robotic/endoscopic thyroidectomy. Initially, concerns were raised about the safety of this approach, given the need to create subplatysmal tunnels from the mouth to the neck and the use of carbon dioxide insufflation to maintain working space [6]. Unique potential complications such as mental nerve injury (resulting in chin/lip numbness) and CO2 gas embolism were not encountered in open surgery and became topics of interest. Over the past several years, a growing body of literature including large series, meta-analyses, and systematic reviews has examined robotic/endoscopic thyroidectomy outcomes and complications [7-10].
This review synthesizes the current evidence on the clinical outcomes, safety profile, and patient-centered advantages of transoral endoscopic thyroidectomy compared to the conventional transcervical approach. We performed a comprehensive literature search (PubMed, Scopus, Google Scholar) for English-language studies and reviews published through late 2025 on robotic/endoscopic thyroidectomy, focusing on operative outcomes, complication rates, and patient satisfaction. Key findings from high-volume series, comparative studies, and relevant meta-analyses are integrated to provide an updated narrative on the efficacy and risks of the transoral approach. In doing so, we aim to highlight how robotic/endoscopic thyroidectomy measures up against the traditional technique and to outline best practices that mitigate its unique complications.
Clinical Comparison of Robotic/ Transoral Endoscopic Thyroidectomy and Conventional Surgery
Early experiences with robotic/endoscopic thyroidectomy, in properly selected patients, demonstrated that clinical outcomes are largely comparable to conventional open thyroidectomy. Several studies and reviews have reported equivalent surgical success rates and endocrine outcomes between the transoral vestibular approach and the standard transcervical approach. In patients with low-risk differentiated thyroid carcinoma or benign nodules meeting criteria (generally nodule <5 cm, thyroid lobe <8-10 cm, no gross extrathyroidal extension or bulky nodal metastases), robotic/endoscopic thyroidectomy can achieve complete thyroid resection and lymph node dissection yields similar to open surgery [11]. Short-term oncologic outcomes have been promising; for example, lymph node harvest numbers, stimulated thyroglobulin levels, and early recurrence rates did not significantly differ between robotic/endoscopic thyroidectomy and open thyroidectomy in comparative analyses [12]. These findings suggest that, when applied to appropriate candidates, the transoral route does not compromise the fundamental efficacy of thyroid cancer surgery.
Critically, the safety profile of robotic/endoscopic thyroidectomy has proven comparable to conventional surgery for most major outcomes. The incidence of recurrent laryngeal nerve (RLN) injury and hypoparathyroidism, the two most common significant complications of thyroidectomym, is similar between transoral and open approaches in experienced hands. A 2021 meta-analysis of 478 robotic/endoscopic thyroidectomy cases versus 673 open cases found no significant differences in rates of transient or permanent RLN palsy, transient hypocalcemia, permanent hypocalcemia, or postoperative hematoma between the two techniques [13]. Large series around the world likewise report low RLN palsy rates with robotic/transoral endoscopic thyroidectomy (on the order of 3%-5% transient and <1% permanent) that mirror traditional surgery [14]. For example, a global review of robotic/endoscopic thyroidectomy cases documented transient RLN paresis in ~3.9% and permanent RLN injury in only 0.6%, which is in line with historical open thyroidectomy outcomes [15]. Temporary postoperative hypocalcemia from parathyroid gland manipulation occurs in roughly 10%-20% of patients in both approaches, with permanent hypoparathyroidism being rare (~1% or less) [16]. Postoperative bleeding or hematoma requiring re-intervention is uncommon with robotic/endoscopic thyroidectomy (~0.4%-1%) and not significantly different from the open technique [17]. These data reinforce that robotic/transoral endoscopic thyroidectomy, when performed by trained surgeons under proper protocols, can achieve an overall safety profile equivalent to conventional thyroidectomy for major complications.
One area where differences do emerge is in operative time and perioperative recovery. Transoral thyroidectomy is technically demanding and tends to have a longer learning curve. Consequently, mean operative durations for robotic/endoscopic thyroidectomy are consistently longer than for open surgery. In a recent meta-analysis comparing endoscopic approaches, robotic/endoscopic thyroidectomy had an operative time about 17-35 minutes longer on average than remote endoscopic alternatives, and typically 20-30 minutes longer than a standard open thyroidectomy of similar extent [13]. Despite the prolonged operative time, hospitalization length after robotic/endoscopic thyroidectomy is similar to or only marginally longer than after open thyroidectomy. Most patients undergoing transoral thyroidectomy can be discharged within 1-2 days (or in some series, after a short 3-4 day stay largely comparable to the 2-3 day stay of open surgery) [18]. Postoperative pain levels are also reported to be comparable between the two approaches. Some patients experience transient chin or floor-of-mouth discomfort with robotic/endoscopic thyroidectomy, but severe pain is not typical, and overall analgesic requirements are akin to those in open thyroidectomy [19]. Thus, aside from a modest increase in OR time, the perioperative recovery trajectory (hospital stay, pain control, return to diet and activity) for transoral patients parallels that of conventional surgery.
Mental Nerve Injury and Sensory Changes
The mental nerve (a branch of the mandibular division of the trigeminal nerve) supplies sensation to the chin and lower lip, and it represents a unique anatomical consideration in the transoral vestibular approach [20]. Robotic/endoscopic thyroidectomy requires incisions in the oral vestibule (just under the lower lip), and lateral dissection tunnels are created in the chin region, an area traversed by the mental nerve and its branches. Consequently, surgeons identified mental nerve injury as a novel potential complication of transoral thyroidectomy that has no analog in open surgery [21]. Even without permanent nerve transection, stretching or contusion of the mental nerve during flap elevation can lead to numbness, tingling, or paraesthesia in the chin and lower lip postoperatively. The good news is that reported mental nerve sensory changes are usually transient and preventable with proper technique. Meticulous attention to the vestibular incision placement and dissection plane has dramatically reduced this risk. Incisions are placed within a defined “safety zone,” typically a 2-3 cm curvilinear incision in the midline vestibule, at least 10-15 mm above the lower lip sulcus to avoid the mental foramen where the nerve exits [22]. In addition, dissection in the chin flap is kept subperiosteal and limited to minimize traction on mental nerve fibers. When robotic/transoral endoscopic thyroidectomy is performed within these safeguards, studies have found a low incidence of significant mental nerve injury [23]. The topography of the established safety zone is elaborated by Fig. 1.
Topography of mental nerve and incision. A: Most medial branch of the mental nerve. B: Safety zone shaded green and danger zones shaded red. IL, incision line; Ilm, mid-incision position; ILc, canine-incision position; FHL, front horizontal line; mMN, medial mental nerve branch; mMNc, canine-position branch; mMNh, horizontal branch; mMNe, emergence point. Reproduced from Yang et al. Surg Endosc 2020;34(8):3414-23 with permission of Surg Endosc. [44]
Notably, the way sensory changes are evaluated can yield different incidence figures. If patients are directly questioned or examined grossly, only a minority might report noticeable numbness. For instance, one report noted approximately 10% of patients had mild transient chin numbness at 1 week postrobotic/endoscopic thyroidectomy. On the other hand, detailed testing will detect some degree of sensory change in virtually all transoral patients immediately after surgery [24]. A recent prospective study by Tae, et al. [24] used monofilament touch tests on 10 designated chin and neck zones in 43 patients: they found no difference in objective sensation of the chin and lower lip before vs. after surgery, indicating that the mental nerve was largely preserved. However, they did observe a temporary increase in pressure threshold in the submental region (upper neck under the chin), which resolved by 1-3 months postoperatively. In other words, when performed successfully and within proper anatomical bounds, robotic/ endoscopic thyroidectomy did not cause measurable long-term sensory loss in the mental nerve distribution. Similarly, Woo, et al. [25] reported that although 100% of patients had some immediate postoperative decrease in sensation in the chin/lower lip region (when mapped with fine 1 mm grid testing), these sensory deficits were transient. The affected numb area in transoral patients shrank dramatically from an average of ~535 mm² at 1 week to ~114 mm² at 1 month, and further down to ~21 mm² by 2 months. By the 2-month follow-up, 5 of 37 patients (14%) had completely recovered normal sensation, and the remaining 32 patients showed significant partial improvement with only minimal residual numb areas. No transoral patient in that series had permanent or functionally problematic numbness beyond the early postoperative period. In contrast, the control group who underwent open thyroidectomy had no sensory changes at any time, as expected. These results reinforce that mental nerve injury from robotic/endoscopic thyroidectomy is typically limited to a temporary neuropraxia, resolving within weeks to a few months, with proper oral incision placement playing a key role in prevention. To date, permanent mental nerve deficits are exceedingly rare when the vestibular approach is executed correctly [26]. Surgeons now universally emphasize the importance of staying within the safe dissection plane and have published cadaveric studies mapping mental nerve variation to guide safe zones.
Unique Risks and Considerations
Beyond mental nerve concerns, robotic/endoscopic thyroidectomy introduces a few unique risks not present in open thyroidectomy, though all are uncommon. One such complication is subcutaneous emphysema or CO2 embolism. The transoral technique traditionally relies on insufflation of CO2 gas to maintain the operative working space in the neck [27]. If the gas inadvertently enters venous channels (for example, through injury to the anterior jugular vein), a CO2 embolism could occur, a potentially life-threatening event. Fortunately, this complication is extremely rare; only isolated cases have been reported among thousands of robotic/endoscopic thyroidectomy procedures [28]. Preventive measures include careful patient positioning, meticulous hemostasis (to avoid open venous lumens), and using the lowest insufflation pressure that still provides an adequate working space (typically 4-6 mm Hg of pressure) [29]. Some surgeons have adopted gasless techniques using external retractors to eliminate this risk altogether [30]. Infections and wound complications are another consideration due to the oral entry point. There is a theoretical risk of introducing oral flora into the neck dissection planes, but in practice, infections have been rare (≈1%) with prophylactic antibiotics and povidone-iodine oral rinses [31]. A related issue is incision site problems: the vestibule incisions can sometimes lead to minor issues like wound separation, localized infection, or even a small perforation of the chin skin if dissection is too superficial [32]. Airway or swallowing issues are not significantly different from open surgery; if anything, robotic/endoscopic thyroidectomy avoids strap muscle cutting and extensive neck muscle retraction, which might contribute to the favorable postoperative voice and swallowing outcomes reported in some series [33]. In fact, one review noted superior functional voice outcomes in transoral patients, possibly due to reduced cervical tissue trauma. Routine intraoperative nerve monitoring (IONM) is recommended for robotic/endoscopic thyroidectomy to help avoid RLN palsy, given the restricted view and the need to identify the nerve endoscopically [34]. With IONM and refined endoscopic instruments, surgeons have achieved the same standard of nerve preservation as in open surgery. Table 1 provides a summary comparison of key outcomes and considerations between robotic/transoral endoscopic thyroidectomy and conventional thyroidectomy [10,24,34-36].
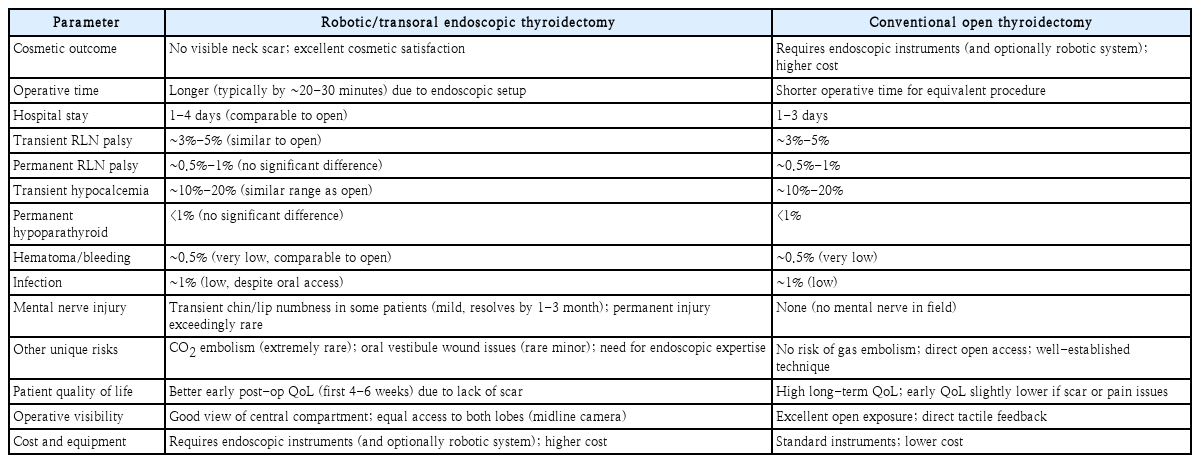
Key comparative outcomes of robotic/transoral endoscopic thyroidectomy vs. conventional open thyroidectomy
As shown in Table 1, robotic/endoscopic thyroidectomy achieves the primary advantage of an invisible scar and improved early postoperative quality-of-life metrics, without sacrificing oncologic or safety outcomes. Patients experience the psychological and cosmetic benefits of not having a neck incision, which can translate into better self-image and satisfaction in the immediate recovery period. On all major clinical endpoints, RLN injury, hypoparathyroidism, bleeding, infection, the transoral approach parallels the conventional approach. The one notable trade-off is the possibility of transient mental nerve-related numbness, a minor complication unique to robotic/endoscopic thyroidectomy, but one that is temporary and preventable with meticulous technique.
It should be noted that overall complication rates may initially appear slightly higher with robotic/endoscopic thyroidectomy when minor issues are included, especially early in a surgeon’s learning curve. For example, an early North American series reported a higher rate of “minor complications” in the transoral group (17.5%) compared to open surgery (9.3%), a difference driven largely by transient issues like mental nerve numbness, small skin perforations, or seromas [37]. However, as surgeons gain experience, these minor events have decreased significantly. Many high-volume centers now report minimal complication differences after surpassing the learning curve of roughly 20-30 cases [38]. The literature indicates a clear trend of improved outcomes with increased surgeon experience and refinements in technique (such as better flap elevation methods and use of nerve monitoring), bringing the minor complication rate of robotic/endoscopic thyroidectomy down over time. In essence, the more robotic/endoscopic thyroidectomy is practiced, the safer and more routine it becomes, much like any innovative surgical technique.
Current Role of Robotic/Transoral Endoscopic Thyroidectomy
Proper patient selection is paramount for robotic/endoscopic thyroidectomy to be safe and effective. Not every thyroid pathology or patient is suitable for this approach. Ideal candidates are those with a strong desire to avoid a neck scar and who have relatively small, non-invasive thyroid tumors or benign nodules. Common selection criteria include: thyroid nodules ≤5 cm, thyroid gland/lobe diameter ≲10 cm, and clinically N0 or small central compartment metastases only [39]. Most groups limit robotic/endoscopic thyroidectomy to cancers <2 cm in size (papillary microcarcinomas or small differentiated thyroid carcinomas) for oncologic safety [40]. Patients with known locally advanced cancer (extrathyroidal extension invading adjacent structures), large or bulky multinodular goiters, or extensive lateral neck metastasis are not candidates for transoral surgery [3]. Additionally, any history of radiation or major neck surgery could alter tissue planes and is generally considered a relative contraindication for the transoral route. Importantly, increased body-mass index is not a strict contraindication. Studies have shown obesity does not significantly increase robotic/endoscopic thyroidectomy complication rates, though it can make dissection more laborious [41-43].
From a surgeon’s perspective, adequate training in endoscopic or robotic thyroidectomy techniques is essential before attempting robotic/endoscopic thyroidectomy. The need for specialized equipment (endoscopic towers, laparoscopic instruments, energy devices, possibly a surgical robot for some) and the higher cost per case are practical considerations for widespread implementation. In some healthcare settings, the cost and longer operative time have limited routine use of robotic/endoscopic thyroidectomy despite patient interest. Nonetheless, as instrumentation improves and more surgeons become proficient, the efficiency of the procedure is expected to get closer to that of open surgery.
Conclusion
Transoral endoscopic thyroidectomy via the vestibular approach has proven to be a feasible, safe, and cosmetically rewarding alternative to conventional open thyroidectomy in appropriately selected patients. Over roughly a decade of development, accumulating evidence indicates that robotic/endoscopic thyroidectomy can achieve oncologic and clinical outcomes equivalent to the gold-standard transcervical approach. The paramount advantage of robotic/endoscopic thyroidectomy is the avoidance of any visible scar, which translates into higher early postoperative quality of life and patient satisfaction, particularly among those self-conscious about neck scarring. This cosmetic benefit does not come at the cost of higher permanent morbidity: major complication rates (RLN injury, permanent hypoparathyroidism, hematoma, etc.) are statistically no different from open surgery. The transoral route does introduce a distinct profile of minor risks, most notably transient mental nerve sensory changes, but with refined surgical technique and increased experience, these complications have been largely mitigated and are almost always temporary. Surgeons can virtually eliminate permanent mental nerve injury by adhering to safe zones for incisions and limiting dissection in the chin area. Rare complications like CO2 embolism are now well-recognized and preventable with proper precautions.
In conclusion, transoral endoscopic thyroidectomy has expanded the surgical armamentarium as a truly scarless thyroid surgery that does not compromise patient safety or treatment efficacy. It exemplifies the marriage of technological innovation with patient-centered care, addressing patients’ cosmetic concerns while maintaining excellent clinical outcomes. As more surgeons acquire expertise and long-term data continue to mature (particularly on recurrence rates and survivorship in oncologic cases), robotic/endoscopic thyroidectomy is poised to become an increasingly mainstream option for thyroidectomy. For the subset of patients intensely concerned about neck scars or with a history of keloids, robotic/endoscopic thyroidectomy offers a compelling solution with demonstrable benefits. Ongoing research and refinement, including comparisons of quality of life and cost-effectiveness, will further clarify the role of transoral thyroidectomy. Based on current evidence, however, it is clear that in the hands of experienced surgeons, robotic/endoscopic thyroidectomy is a safe and effective approach that yields outcomes on par with conventional surgery, all while leaving patients with nothing more than a hidden smile-line incision and an unscarred neck. The advent of this technique marks a significant advance in thyroid surgery, aligning surgical success with the cosmetic and emotional well-being of patients.
Notes
Conflict of Interest
Seung Hoon Woo is an editorial board member of the journal but was not involved in the peer reviewer selection, evaluation, or decision process of this article. No other potential conflicts of interest relevant to this article were reported.
Acknowledgments
This study was supported by the Dankook Institute of Medicine & Optics. This research was made possible through the support of the Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (MOE) (RS-2023-00247651 and NRF-2020R1A6A1A03043283), the Korea Medical Device Development Fund grant funded by the Ministry of Science and ICT, the Ministry of Trade, Industry, and Energy (MOTIE, Korea), the Ministry of Health & Welfare, and the Ministry of Food and Drug Safety (RS-2020-KD000027), the Regional Innovation Strategy (RIS) through the National Research Foundation of Korea (NRF) funded by the MOE (2021RIS-001), the SNUH Lee Kun-hee Child Cancer & Rare Disease Project, Republic of Korea (23C-02300100), and the Technology Innovation Program Development Program (20021987) funded by the MOTIE, Korea.
Author Contribution
Conceptualization: Ken Woo, Seung Hoon Woo. Data curation: Ken Woo. Formal analysis: Ken Woo. Investigation: Ken Woo. Methdology: Ken Woo. Project adminiatration: Seung Hoon Woo. Resources: Seung Hoon Woo. Software: Ken Woo. Supervision: Seung Hoon Woo. Validation: Seung Hoon Woo. Visualization: Ken Woo. Writing—original draft: Ken Woo. Writing—review & editing: Ken Woo, Seung Hoon Woo.