žĄú Ž°†
Ū鳎ŹĄŽäĒ ÍĶ¨žĚłŽĎźžēĒžĚī ŽįúžÉĚŪēėŽäĒ ÍįÄžě• ŪĚĒŪēú Ž∂ÄžúĄžĚīŽč§. Ū鳎ŹĄžēĒÍ≥ľ human papilloma virus(HPV)žôÄžĚė žóįÍīÄžĄĪžĚÄ žěė žēĆŽ†§ž†ł žěąžúľŽ©į, HPVŽäĒ ŪĚ°žóį, žĚĆž£ľžôÄ Ūē®ÍĽė ŽĎźÍ≤ĹŽ∂ÄžēĒžĚė ÍįÄžě• ž§ĎžöĒŪēú žõźžĚłžĚī ŽźėŽäĒ žöĒžĚłžĚīŽč§. 1990ŽÖĄŽĆÄ žĚīž†ĄžóźŽäĒ ÍĶ¨žĚłŽĎź Ž∂ÄžúĄÍįÄ ŽĎźÍ≤ĹŽ∂ÄžēĒ ž§Ď žĚīžį®žĄĪ žõźŽįúžēĒ(second primary malignancy)žĚī ŽĎź Ž≤ąžßłŽ°ú ÍįÄžě• ŪĚĒŪēėÍ≤Ć ŽįúžÉĚŪēėŽäĒ žĚľžį® žõźŽįú Ž∂ÄžúĄŽ°ú žēĆŽ†§ž†ł žěąžóąžúľŽāė, žĶúÍ∑ľ HPVžĚė ž∂úŪėĄ žĚīŪõĄžóźŽäĒ ŽįúžÉĚŽ•†žĚī žĶúžÜĆ žąėž§ÄžúľŽ°ú ŪėĄž†ÄŪěą ÍįźžÜĆŪĖąŽč§[1]. ŽĎźÍ≤ĹŽ∂ÄžēĒžúľŽ°ú žā¨ŽßĚŪēėŽäĒ ŪôėžěźžĚė žēĹ 1/3žĚÄ žĚīžį®žĄĪ žõźŽįúžēĒžóź žĚėŪēú Í≤ÉžĚīŽ©į, žĚīŽäĒ žõźÍ≤© ž†ĄžĚīŽ°ú žĚłŪēú žā¨ŽßĚžĚė žēĹ 3Žįįžóź ŪēīŽčĻŪēúŽč§ŽäĒ Ž≥īÍ≥†ÍįÄ žěąŽäĒ ŽįĒ[2,3], ŽĎźÍ≤ĹŽ∂Ä žēĒžóźžĄú žĚīžį®žĄĪ žõźŽįúžēĒžĚÄ žěĄžÉĀž†ĀžúľŽ°ú ž§ĎžöĒŪēėŽč§. žĶúÍ∑ľ, HPVžôÄ ÍīÄŽ†®Žźú žĚīžį®žĄĪ žõźŽįúžēĒ ž¶ĚŽ°ÄŽď§žĚī Žč§žąė Ž≥īÍ≥†ŽźėÍ≥† žěąžĖī, žěĄžÉĀžĚėŽď§Í≥ľ Ž≥ĎŽ¶¨ŪēôžěźŽď§žĚÄ žĚī žßąŪôėÍĶįžóź ŽĆÄŪēī ŪôúŽįúŪēėÍ≤Ć žóįÍĶ¨ ž§ĎžĚīŽč§[4]. ŪēúŪéł, ÍłįÍīÄžēĒ(tracheal cancer)žĚÄ 100ŽßĆ Ž™ÖŽčĻ 1ÍĪīžĚė ŽįúŽ≥ĎŽ•†žĚĄ Ž≥īžĚīŽäĒ ŽďúŽ¨ł žßąŪôėžĚīŽč§[5]. Ž≥ł ž¶ĚŽ°ÄŽäĒ Í≥†žúĄŪóė HPV žĖĎžĄĪ Ū鳎ŹĄžēĒ ŪôėžěźžóźžĄú, žĚīžčúžĄĪ(metachronous)žúľŽ°ú ÍłįÍīÄžóź žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŽįúžÉĚŪēú ž≤ę Ž≤ąžßł žā¨Ž°ÄŽ°ú Ž¨łŪóĆ Í≥†žįįÍ≥ľ Ūē®ÍĽė Ž≥īÍ≥†ŪēėŽäĒ ŽįĒžĚīŽč§.
ž¶Ě Ž°Ä
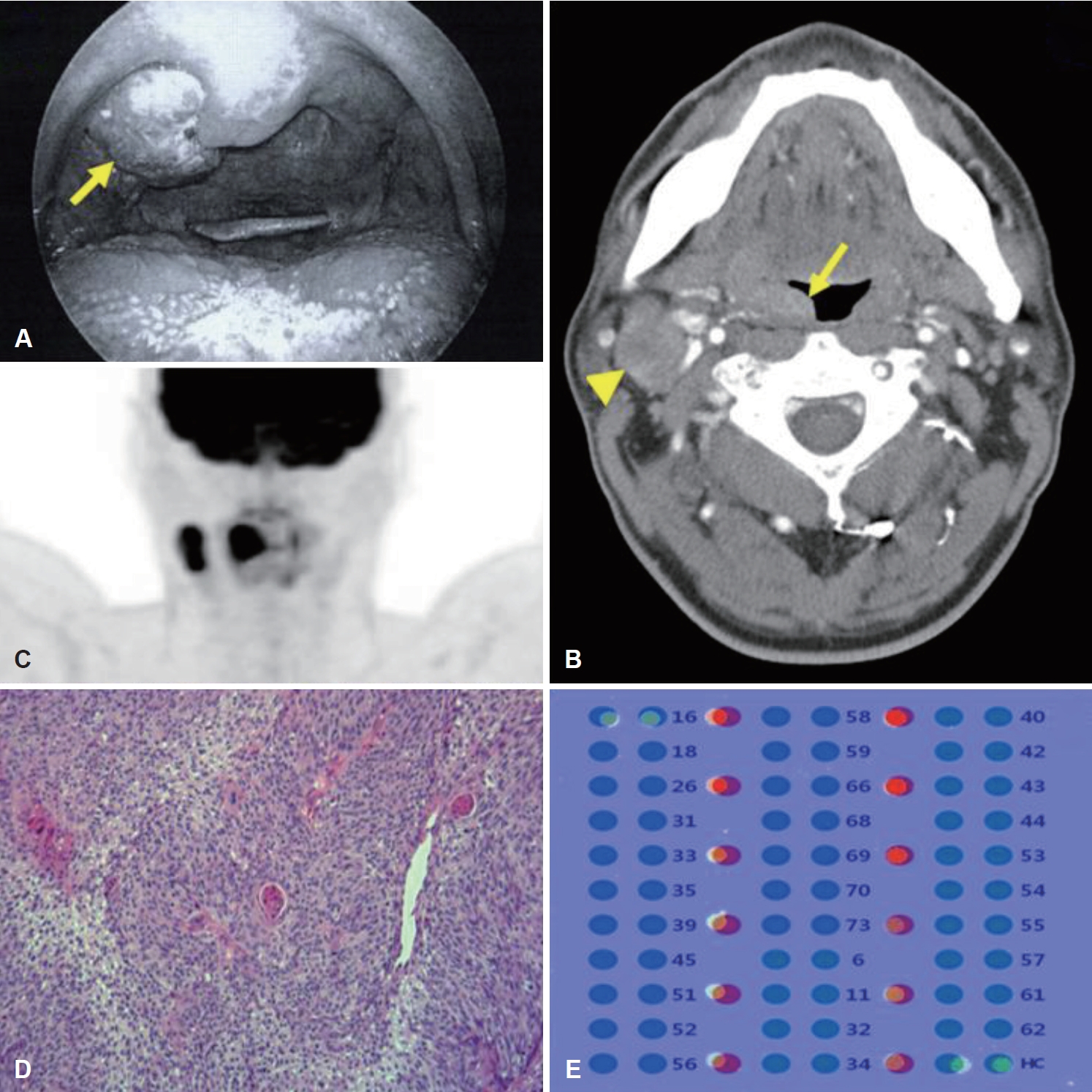
47žĄł Žā®žěź ŪôėžěźÍįÄ žöįžł° Ū鳎ŹĄ žĘÖŽ¨ľžĚĄ ž£ľžÜĆŽ°ú ŪÉÄ Ž≥Ďžõź ŽāīžõźŪēėžó¨ žčúŪĖČŪēú ž°įžßĀ Í≤Äžā¨žóźžĄú ŪéłŪŹČžĄłŪŹ¨žēĒ žÜĆÍ≤¨žúľŽ°ú Ž≥łžõźžóź žĚėŽĘįŽźėžóąŽč§. ŪôėžěźŽäĒ 20ÍįĎŽÖĄ žĚīžÉĀžĚė ŪĚ°žóįžěźžėÄžúľŽ©į žā¨ŪöĆž†Ā žĚĆž£ľžěźžėÄžúľŽāė ŽįúžēĒ Ž¨ľžßąžóź ŽÖłž∂úŽźú Í≥ľÍĪįŽ†•žĚÄ žóÜžóąŽč§. žč†ž≤ī Í≤Äžā¨žóźžĄú žöįžł° Ū鳎ŹĄžóź žēĹ 2 cmžĚė žú†ŽĎźžÉĀ žĘÖŽ¨ľžĚī ŪôēžĚłŽźėžóąžúľŽ©į(Fig. 1A), žöįžł° Í≤ĹŽ∂Ä level II žėĀžó≠žóź žēĹ 3 cmžĚė Žč®Žč®ŪēėÍ≥† žēēŪÜĶžĚī žóÜžúľŽ©į ž£ľŽ≥Ä ž°įžßĀžóź Í≥†žį©Žźú žĖĎžÉĀžĚė žĘÖŽ¨ľžĚī žīČžßÄŽźėžóąŽč§.
Í≤ĹŽ∂Ä žĽīŪď®ŪĄįŽč®žłĶžī¨žėĀ Í≤Äžā¨(neck CT)žóźžĄú ŽĻĄŽĆÄžĻ≠ž†ĀžĚł Ū鳎ŹĄžĚė ŽĻĄŽĆÄ ŽįŹ ž°įžėĀ ž¶ĚÍįē žÜĆÍ≤¨žĚĄ Ž≥īžėÄžúľŽ©į, ŽŹôžł° Í≤ĹŽ∂Äžóź Žč§žąėžĚė Ž¶ľŪĒĄž†ą ŽĻĄŽĆÄÍįÄ ŪôēžĚłŽźėžóąŽč§(Fig. 1B). ÍįÄžě• ŪĀį Ž¶ľŪĒĄž†ąžĚÄ žě•Í≤Ĺ žēĹ 3 cmŽ°ú žł°ž†ēŽźėžóąŽč§. žĖĎž†ĄžěźŽį©ž∂ú žĽīŪď®ŪĄįŽč®žłĶžī¨žėĀ Í≤Äžā¨(PET-CT)žóźžĄú ŽŹôžł° Ž¶ľŪĒĄž†ą ž†ĄžĚīŽ•ľ Ž≥īžėÄžúľŽāė, ŪÉÄ žě•Íłį ž†ĄžĚīžĚė ž¶ĚÍĪįŽäĒ žóÜžóąŽč§(Fig. 1C). Ū鳎ŹĄ žĘÖŽ¨ľžĚė ŪéÄžĻė žÉĚÍ≤Ğ̥ žě¨žčúŪĖČŪēú Í≤įÍ≥ľ ž§ĎŽďĪŽŹĄ Ž∂ĄŪôĒŽŹĄžĚė ŪéłŪŹČžĄłŪŹ¨žēĒ(moderately differentiated squamous cell carcinoma)(Fig. 1D)žĚīžóąžúľŽ©į, Ūē®ÍĽė žčúŪĖČŪēú DNA chip test(Fig. 1E)žóźžĄú HPV-16žóź ŽĆÄŪēī žĖĎžĄĪžĚĄ ŽāėŪÉÄŽÉąŽč§.
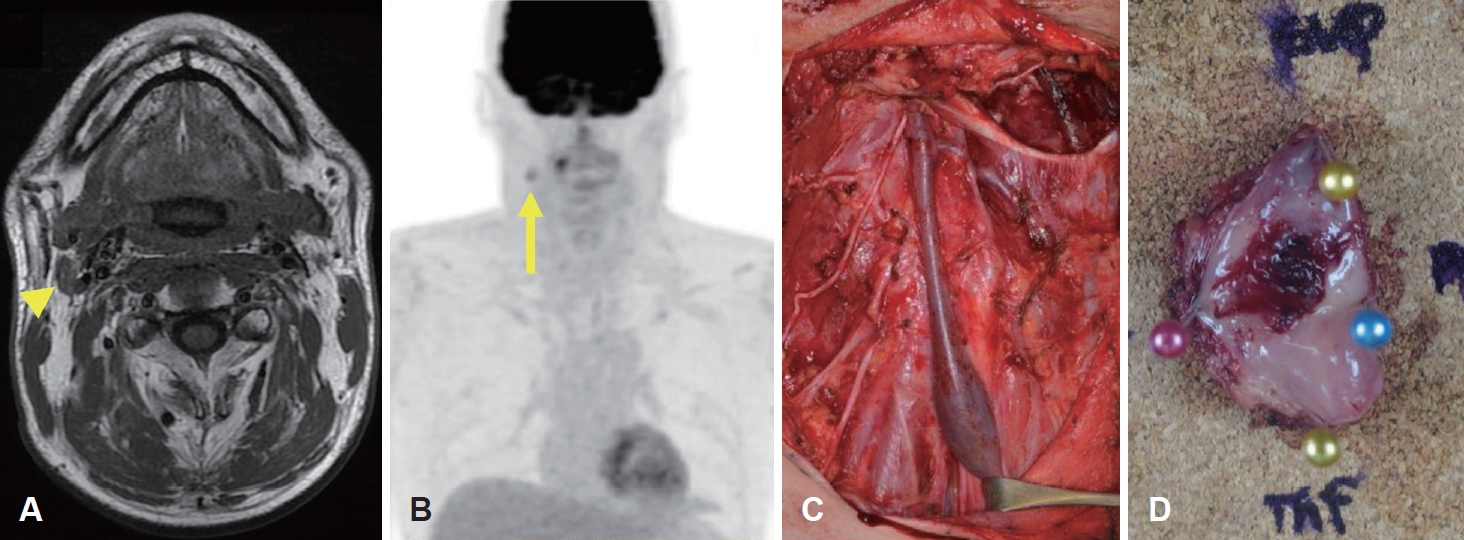
ŪôėžěźŽäĒ Žč§Ūēôž†ú ŪĆÄÍ≥ľ ŽÖľžĚėŽ•ľ ÍĪįž≥ź 6ž£ľžĚľ ŽŹôžēą cetuximabžĚĄ žĚīžö©Ūēú Ūē≠žēĒ ŽįŹ ŽŹôžčú Žį©žā¨žĄ† žĻėŽ£Ć(concurrent chemoradiotherapy, CCRT)(72Gy/40 fractionations)Ž•ľ žčúŪĖČŽįõžēėŽč§. CCRT žĘÖŽ£Ć 3ÍįúžõĒ ŪõĄžóź žčúŪĖČŪēú Í≤ĹŽ∂Ä žěźÍłį Í≥ĶŽ™Ö žėĀžÉĀ Í≤Äžā¨(neck MRI) (Fig. 2A)žóźžĄú žöįžł° Ū鳎ŹĄžĚė ŪĀ¨ÍłįŽäĒ ÍįźžÜĆŪēėžėÄžúľŽāė, žöįžł° Í≤ĹŽ∂Ä level IIžóź žĚľŽ∂Ä Ž¶ľŪĒĄž†ąžĚī Žā®žēĄžěąŽäĒ žÜĆÍ≤¨žĚĄ ŪôēžĚłŪē† žąė žěąžóąžúľŽ©į, žĚī Ž≥ĎŽ≥ÄžĚÄ PET-CTžóźžĄú fluorodeoxyglucose Í≥†žĄ≠ž∑®Ž•ľ Ž≥īžĚīŽäĒ ž†ĄžĚīžĄĪ Ž¶ľŪĒĄž†ąŽ°ú ŪĆźŽč®ŽźėžóąŽč§(Fig. 2B). žöįžł° žł°Í≤ĹŽ∂ÄžĚė žěĒžó¨ Ž¶ľŪĒĄž†ąžóź ŽĆÄŪēī Ž≥ÄŪėē Í∑ľžĻė Í≤ĹŽ∂Ä ž†ąž†úžą† type II(Fig. 2C) ŽįŹ žöįžł° Ū鳎ŹĄ ž†ąž†úžą†(Fig. 2D)žĚĄ žčúŪĖČŪēėžėÄŽč§. Ž≥ĎŽ¶¨ž°įžßĀŪēôž†Ā Í≤įÍ≥ľžóźžĄú žīĚ 20ÍįúžĚė Ž¶ľŪĒĄž†ą ž§Ď Í≤ĹŽ∂Ä level IIžĚė 1Íįú Ž¶ľŪĒĄž†ąžóźžĄú ŪéłŪŹČžĄłŪŹ¨žēĒ ž†ĄžĚīÍįÄ ŽįúÍ≤¨ŽźėžóąŽč§. žöįžł° Ū鳎ŹĄžóźžĄúŽäĒ 1√ó0.9 cmžĚė Í≥†Ž∂ĄŪôĒ ŪéłŪŹČžĄłŪŹ¨žēĒ(well differentiated squamous cell carcinoma)žĚī ŪôēžĚłŽźėžóąžúľŽ©į, žč¨Ž∂ÄŽ•ľ ŪŹ¨Ūē®Ūēėžó¨ Ž™®Žď† ž†ąž†úžóįžóźžĄú žĘÖžĖĎžĚÄ ŽįúÍ≤¨ŽźėžßÄ žēäžēėŽč§.
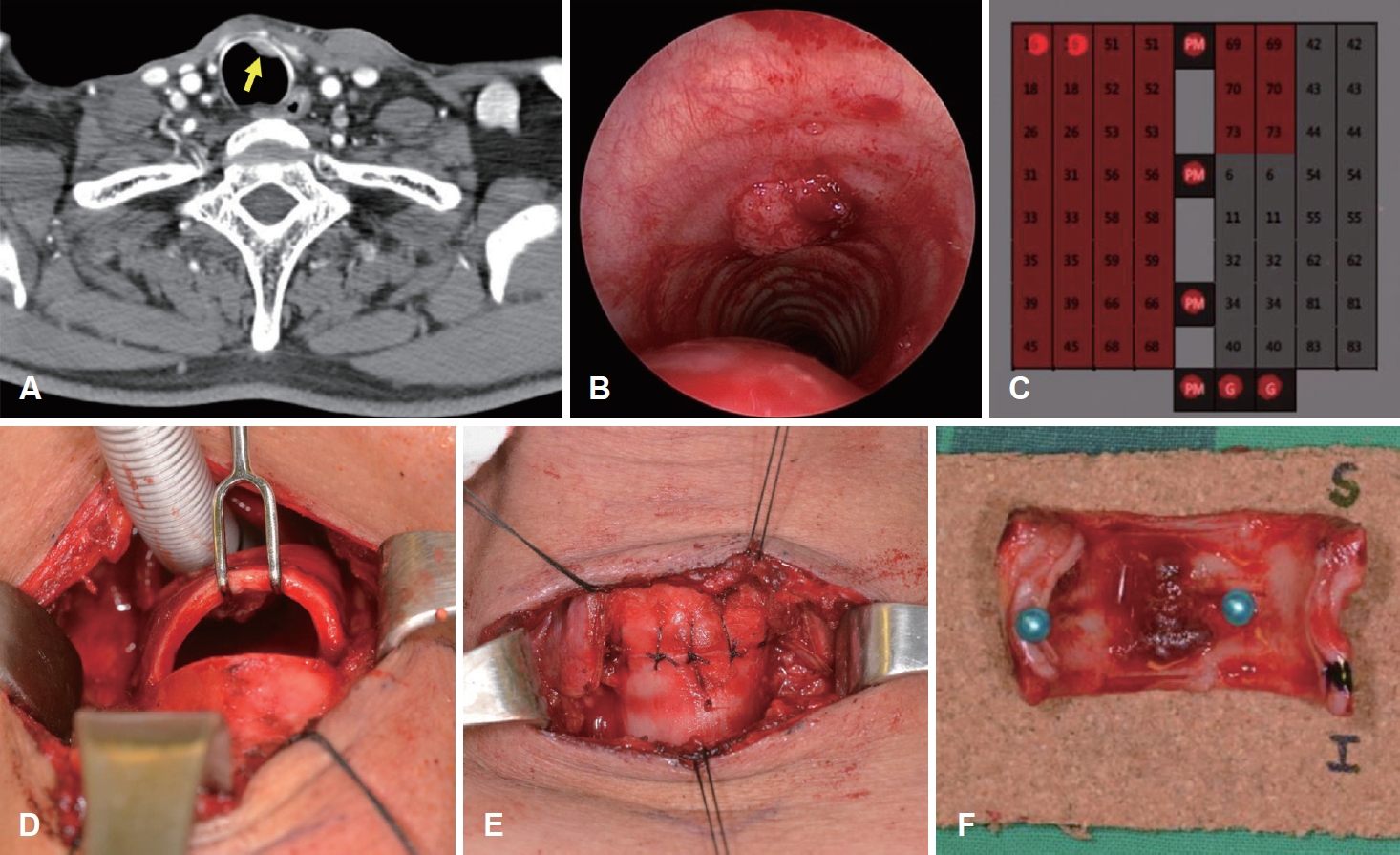
22ÍįúžõĒžĚė ž∂Ēž†Ā ÍīÄžįį ÍłįÍįĄ ŽŹôžēą žě¨Žįú ŽėźŽäĒ ž†ĄžĚīžĚė ž¶ĚÍĪįŽäĒ žóÜžóąŽč§. Í∑łŽü¨Žāė, CTžóźžĄú žĘĆžł° ž†ēž§Ď ž£ľžúĄ ÍłįÍīÄ ŽāīÍįēžóź žēĹ 1.1 cmžĚė ž°įžėĀ ž¶ĚÍįēŽźėŽäĒ Ž≥ĎŽ≥ÄžĚī ŽįúÍ≤¨ŽźėžóąŽč§(Fig. 3A). Í≤ĹžĄĪ ÍłįÍīÄžßÄÍ≤ĹÍ≤Äžā¨žóźžĄú ÍłįÍīÄžĚė ŽāīÍįē Žāī žú†ŽĎźžÉĀ žĘÖŽ¨ľžĚī ŪôēžĚłŽźėžóąŽč§(Fig. 3B). žÉĚÍ≤Ä Í≤įÍ≥ľ ŪéłŪŹČžĄłŪŹ¨žēĒžĚīžóąÍ≥†, p16 Ž©īžó≠žóľžÉČžóź ŽĆÄŪēī žĖĎžĄĪ, DNA chip testžóźžĄú HPV-16 žĖĎžĄĪžĚīžóąŽč§(Fig. 3C). ÍłįÍīÄžēĒ Ž≥ĎŽ≥Äžóź ŽĆÄŪēī 3Ž≤ąžßłŽ∂ÄŪĄį 6Ž≤ąžßł ÍłįÍīÄŽ•ú ž†ąž†ú ŽįŹ ÍłįÍīÄ Žč®Žč®Ž¨łŪē©žą†Í≥ľ Ūē®ÍĽė ÍįĎžÉĀžĄ† ŪėĎŽ∂Ä ž†ąž†úžą†, žĖĎžł° ž§Ďžč¨ Í≤ĹŽ∂Ä Ž¶ľŪĒĄž†ą ž≤≠žÜĆžą†žĚĄ žčúŪĖČŪēėžėÄÍ≥†, ÍłįÍīÄž†ąÍįúžą†žĚÄ žčúŪĖČŪēėžßÄ žēäžēėŽč§(Fig. 3D-F). žąėžą† ž§Ď ŽŹôÍ≤į ž†ąŪéł Í≤Äžā¨Ž•ľ žčúŪĖČŪēėžó¨ ÍłįÍīÄžĚė ž†ąž†úžóįžóź žěĒžó¨ žĘÖžĖĎ žĄłŪŹ¨ÍįÄ žóÜžĚƞ̥ ŪôēžĚłŪēėžėÄŽč§. žąėžą† 2žĚľ ŪõĄ ž§ĎŪôėžěźžč§žóźžĄú ÍłįÍīÄ Žāī ŪäúŽłĆŽ•ľ ŽįúÍīÄŪēėžėÄÍ≥†, žĚľŽįėŽ≥Ϟ觎°ú ž†Ąžč§ŪēėžėÄŽč§. Ž≥ĎŽ¶¨ž°įžßĀŪēôž†Ā Í≤Äžā¨ Í≤įÍ≥ľ ÍłįÍīĞ󟞥ú ž†źŽßČŪēėžłĶ(submucosa)žĚĄ žĻ®Ž≤ĒŪēėŽäĒ ž§ĎŽ∂ĄŪôĒŽŹĄžĚė ŪéłŪŹČžĄłŪŹ¨žēĒžĚī ŪôēžĚłŽźėžóąŽč§. žīĚ 4ÍįúžĚė ž§Ďžč¨ Í≤ĹŽ∂Ä Ž¶ľŪĒĄž†ąžóźžĄúŽäĒ ž†ĄžĚī žÜĆÍ≤¨žĚĄ Ž≥īžĚīžßÄ žēäžēėŽč§. ÍłįÍīÄ žąėžą† 2ž£ľ ŪõĄ Ūē©Ž≥Ďž¶Ě žóÜžĚī ŪôėžěźŽäĒ ŪáīžõźŪēėžėÄŽč§. ŪôėžěźŽäĒ žąėžą† ŪõĄ 4ŽÖĄ 8ÍįúžõĒžĚė ž∂Ēž†Ā ÍīÄžįį ÍłįÍįĄ ŽŹôžēą Ū鳎ŹĄ, ÍłįÍīÄ ŽįŹ Í≤ĹŽ∂Ä ŽďĪžóź žě¨Žįú ŽįŹ ž†ĄžĚīžĚė žÜĆÍ≤¨ žóÜžĚī žôłŽěėžóźžĄú ž∂Ēž†Ā ÍīÄžįį ž§Ďžóź žěąŽč§. Ž≥ł žóįÍĶ¨ŽäĒ žąúž≤úŪĖ•ŽĆÄŪēôÍĶźŽ∂Äž≤úŽ≥Ďžõź žěĄžÉĀžóįÍĶ¨žč¨žĚėžúĄžõźŪöĆžĚė žäĻžĚłžĚĄ ŽįõžēėŽč§(2019-11-012).
Í≥† žįį
Warren [6]žĚī ž†úžčúŪēú ž†ēžĚėžóź ŽĒįŽ•īŽ©ī, žĚīžį®žĄĪ žõźŽįúžēĒžĚīŽěÄ Íłįž°īžĚė žĘÖžĖĎÍ≥ľ ŪēīŽ∂ÄŪēôž†ĀžúľŽ°ú ÍĶ¨Ž≥ĄŽźėŽäĒ Ž≥ĄÍįúžĚė Ž∂ÄžúĄžóźžĄú ŽįúžÉĚŪēú žĘÖžĖĎžúľŽ°úžĄú ž°įžßĀŪēôž†ĀžúľŽ°ú žēÖžĄĪžúľŽ°ú ž¶ĚŽ™ÖŽźėÍ≥†, ž†ĄžĚīžĚė ÍįÄŽä•žĄĪžĚÄ Žįįž†úŽźėžĖīžēľ ŪēúŽč§Í≥† ŪēėžėÄŽč§. ŽėźŪēú ÍĶ≠žÜĆ žě¨ŽįúÍ≥ľžĚė ÍįźŽ≥ĄŽŹĄ ŪēĄžöĒŪēúŽćį, Ž≥ł ž¶ĚŽ°ÄžóźžĄú Ū鳎ŹĄžôÄ ŪēīŽ∂ÄŪēôž†ĀžúľŽ°ú žôĄž†ĄŪěą Ž∂ĄŽ¶¨ŽźėžĖī žěąŽäĒ ÍłįÍīÄžĚė ž†źŽßČŪēėžłĶžóź ÍĶ≠ŪēúŽźú žĘÖžĖĎžĚī ŽįúžÉĚŪēėžėÄÍ≥† Ū鳎ŹĄžēĒžóź ŽĆÄŪēú žąėžą† žčú ÍłįÍīÄž†ąÍįúžą†žĚĄ žčúŪĖČŪēėžßÄ žēäžēėÍłį ŽēĆŽ¨łžóź žąėžą†Ž°ú žĚłŪēú žĘÖžĖĎ ŪĆĆžĘÖ(seeding)žĚė ÍįÄŽä•žĄĪžĚÄ Žß§žöį ŽāģŽč§Í≥† žÉĚÍįĀŽźėžĖī žěĄžÉĀž†ĀžúľŽ°ú žĚīžį®žĄĪ žõźŽįúžēĒžĚė ž†ēžĚėžóź Ž∂ÄŪē©ŪēúŽč§.
HPVÍįÄ ŽĎźÍ≤ĹŽ∂ÄžēĒžĚė ž§ĎžöĒŪēú žúĄŪóėžĚłžěźŽ°ú ŽįĚŪėÄžßÄŽ©īžĄú žĚīžôÄ ÍīÄŽ†®Žźú žĚīžį®žĄĪ žõźŽįúžēĒ ŽėźŪēú žÉąŽ°úžöī ÍīĞ訞ā¨Ž°ú Ž∂ÄžÉĀŪēėžėÄŽäĒŽćį, žĶúÍ∑ľ žėĀÍĶ≠žóźžĄú žčúŪĖČŪēú Ž©ĒŪÉÄ Ž∂ĄžĄĚžóź ŽĒįŽ•īŽ©ī ÍĶ¨žĚłŽĎź ŽįŹ žěźÍ∂ĀÍ≤ĹŽ∂Ä, žôłžĚĆŽ∂Ä ŽįŹ Ūē≠Ž¨ł ŽďĪžóźžĄú ŽįúžÉĚŪēú HPV žĖĎžĄĪžĚė žõźŽįúžēĒ ŪôėžěźŽäĒ HPVžôÄ ÍīÄŽ†®Žźú žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŽįúžÉĚŪē† ŪôēŽ•†žĚī žēĹ 5Žįį ž¶ĚÍįÄŪēúŽč§Í≥† ŪēėžėÄŽč§[4]. ŪēúŪéł, ÍĶ≠Žāī ŽĎźÍ≤ĹŽ∂ÄžēĒ Ūôėžěź ŽćįžĚīŪĄįŽ•ľ Ž∂ĄžĄĚŪēú žĚīžčúžĄĪ žĚīžį®žĄĪ žõźŽįúžēĒ žóįÍĶ¨žóźžĄúŽäĒ HPV žĖĎžĄĪ ÍĶ¨žĚłŽĎźžēĒžĚė Í≤Ĺžöį ŪõĄŽĎź, ŪēėžĚłŽĎźžēĒŽ≥īŽč§ žĚīžį®žĄĪ žõźŽįúžēĒ ŽįúžÉĚŽ•†žĚī ŪÜĶÍ≥Ąž†ĀžúľŽ°ú žú†žĚėŪēėÍ≤Ć ŽāģÍ≤Ć ŽāėŪÉÄŽā¨Žč§[7].
Íłįž°ī žóįÍĶ¨Žď§žóź ŽĒįŽ•īŽ©ī žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŪėłŽįúŪēėŽäĒ Ž∂ÄžúĄŽäĒ ŽĎźÍ≤ĹŽ∂Ä, žčĚŽŹĄ, ŪŹź ŽďĪžúľŽ°ú Ž≥īÍ≥†ŽźėžĖīžôĒŽäĒŽćį, Ž≥ł ž¶ĚŽ°ÄžóźžĄúŽäĒ žēĒ ŽįúžÉĚŽ•† žěźž≤īÍįÄ Žß§žöį ŽďúŽ¨ł ÍłįÍīĞ󟞥ú žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŽįúžÉĚŪēėžėÄžúľŽ©į žĚīŽäĒ Ž¨łŪóĆžÉĀ Ž≥īÍ≥†Žźú ŽįĒÍįÄ žóÜŽč§. ž†ÄžěźŽď§žĚÄ ŪôėžěźžĚė ŪĚ°žóįŽ†•Í≥ľ HPV ÍįźžóľžĚī žĄúŽ°ú žÉĀžäĻž†ĀžúľŽ°ú žėĀŪĖ•žĚĄ ŽĮłžĻú Í≤įÍ≥ľŽ°ú žėąžł°ŪēúŽč§. Syrj√§nen [8]žóź ŽĒįŽ•īŽ©ī, žõźž£ľ žĄłŪŹ¨Ž°ú ÍĶ¨žĄĪŽźėžĖī žěąŽäĒ ŪėłŪĚ° žÉĀŪĒľŽäĒ HPVžĚė žĚľžį® ŪĎúž†ĀžĚī žēĄŽčąžßÄŽßĆ, žĚėžĚłžĄĪ ŪéłŪŹČžõźž£ľžÉĀŪĒľž†ĎŪē©Ž∂Ä(iatrogenic squamocolumnar junctions) ŽėźŽäĒ ŪĚ°žóįžóź žĚėŪēī ŽįúžÉĚŪēú ŪéłŪŹČžÉĀŪĒľŪôĒžÉĚ(squamous metaplasia)žĚÄ HPV ÍįźžóľžĚė žßĄžěÖ Ž∂ÄžúĄÍįÄ Žź† žąė žěąŽč§Í≥† ŪēėžėÄŽč§. ž¶Č, Ž≥ł ž¶ĚŽ°ÄžóźžĄú ŪĚ°žóįžóź žĚėŪēī ŽįúžÉĚŪēú ÍłįÍīÄžĚė ŪėłŪĚ° žÉĀŪĒľžĄłŪŹ¨žĚė Ž≥ÄŪôĒŽ°ú žĚłŪēī HPV Íįźžóľžóź ž∑®žēĹŪēú ŪôėÍ≤ĹžĚī ž°įžĄĪŽźėžóąÍ≥† Í∑ł Í≤įÍ≥ľ žĚīžį®žĄĪ žõźŽįúžēĒžĚī ÍłįÍīĞ󟞥ú ŽįúžÉĚŪēú Í≤ÉžúľŽ°ú ž∂Ēžł°ŪēúŽč§.
ŽĎźÍ≤ĹŽ∂ÄžēĒžóźžĄú žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŪėłŽįúŪēėŽäĒ žĚīžú†ŽäĒ Slaughter ŽďĪ[9]žĚī ž†úžčúŪēú žÉĀŽ∂ÄÍłįžčĚŽŹĄÍīÄ(upper aerodigestive tract) ž†Ąž≤īÍįÄ ŪĚ°žóį ŽďĪ ŽįúžēĒ Ž¨ľžßąžóź ŽŹôžčúžóź ŽÖłž∂úŽźėžĖī ŽįúžÉĚŪēúŽč§ŽäĒ ‚Äėfield cancerization‚Äô ÍįúŽÖźžĚī žĚľŽįėž†ĀžĚīŽč§. Í∑łŽü¨Žāė HPV ÍįźžóľÍ≥ľ ÍīÄŽ†®Žźú žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŽįúžÉĚŪēėŽäĒ Íłįž†Ąžóź ŽĆÄŪēīžĄúŽäĒ žēĄžßĀ Ž™ÖŪôēŪěą ŽįĚŪėÄžßÄžßÄ žēäžēėŽč§. žĚīŽ•ľ žĄ§Ž™ÖŪēėÍłį žúĄŪēīžĄú ž†úžčúŽźú ÍįÄžĄ§žóźŽäĒ Žč®žĚľžĚė žßÄžÜ枆ĀžĚł HPV ÍįźžóľžĚī Žč§žīąž†źžĚė žĘÖžĖϞ̥ žú†ŽįúŪēúŽč§ŽäĒ Í≤ÉÍ≥ľ, HPVžĚė Žč§ž§Ď ÍįźžóľžĚī žĄúŽ°ú Žč§Ž•ł ŽŹÖŽ¶Ĺž†ĀžĚł Ž∂ÄžúĄžóźžĄú ŽįúžÉĚŪēėžó¨ žĘÖžĖϞ̥ žú†ŽįúŪē† žąė žěąŽč§ŽäĒ Í≤É, Í∑łŽ¶¨Í≥† žĶúžīąžĚė HPV Íįźžóľžóź žĚėŪēī ŽįúžÉĚŪēú ŪĀīŽ°†žĚī žĄúŽ°ú Žč§Ž•ł ŪēīŽ∂ÄŪēôž†Ā Ž∂ÄžúĄŽ°ú žĚīŽŹôŪēėžó¨ ŽįúžÉĚŪēėŽäĒ, ŪĀīŽ°†žĚī žóįÍīÄŽźėžĖī žěąŽäĒ žĘÖžĖϞ̥ žú†ŽįúŪēúŽč§ŽäĒ Í≤ÉžĚī žěąŽč§[10].
ŽĎźÍ≤ĹŽ∂ÄžĚė žĚīžį®žĄĪ žõźŽįúžēĒžóźžĄú HPV typežĚĄ Ž∂ĄžĄĚŪēú žĚīž†ĄžĚė žóįÍĶ¨Žď§žóź ŽĒįŽ•īŽ©ī, ŽŹôžĚľŪēú HPV-16žóź žĚėŪēī žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŽįúžÉĚŪēėŽ©į, žĚľŽ∂Ğ󟞥úŽäĒ žóľÍłį žĄúžóīžĚī žôĄž†ĄŪěą žĚľžĻėŪēėŽäĒ Í≤įÍ≥ľŽ•ľ Ž≥īžėÄŽč§Í≥† Ž≥īÍ≥†ŪēėžėÄŽč§[11,12]. ŪēúŪéł žó¨žĄĪžĚė Í≤Ĺžöį HPV žĖĎžĄĪ ÍĶ¨žĚłŽĎźžēĒžĚĄ žßĄŽč®ŽįõžĚÄ ŪôėžěźÍĶįžóźžĄú žĚīžį®žĄĪ žěźÍ∂ĀÍ≤ĹŽ∂ÄžēĒ ŽįúŽ≥ĎŽ•†žĚī žú†žĚėŪēėÍ≤Ć ŽÜíŽč§Í≥† ŪēėžėÄžúľŽ©į[7], žěźÍ∂ĀÍ≤ĹŽ∂ÄŽäĒ žěė žēĆŽ†§žßĄ HPV žóįÍīÄ žēĒ ŪėłŽįú Ž∂ÄžúĄžĚīŽč§. žĚīŽü¨Ūēú ÍįÄžĄ§ ŽįŹ žóįÍĶ¨ Í≤įÍ≥ľŽď§žĚĄ Ū܆ŽĆÄŽ°ú, žĚľžį®ž†ĀžúľŽ°ú ŽįúžÉĚŪēú žĘÖžĖϞ󟞥ú HPV ÍįźžóľžĚī ž°īžě¨ŪēėŽäĒ Í≤Ĺžöį žčúÍįĄ ÍįĄÍ≤©žĚĄ ŽĎźÍ≥† Ž≥ĄÍįúžĚė ŪēīŽ∂ÄŪēôž†Ā Ž∂ÄžúĄ, ŪäĻŪěą HPV ÍįźžóľžĚī žČĹÍ≤Ć ŽįúžÉĚŪēėŽäĒ žúĄžĻėžóź žĚīžį®žĄĪ žõźŽįúžēĒžĚĄ ŽįúžÉĚžčúŪā§ŽäĒ žúĄŪóė žöĒžĚłžúľŽ°úžĄú žěĎžö©Ūē®žĚĄ ž∂Ēž†ēŪē† žąė žěąÍ≤†Žč§.
ŽĎźÍ≤ĹŽ∂ÄžĚė ÍĶ≠žÜĆ žßĄŪĖČžĄĪ ŪéłŪŹČžĄłŪŹ¨žēĒ(locoregionally advanced squamous cell carcinoma)žóźžĄú cetuximabžĚĄ žā¨žö©ŪēėŽäĒ CCRTŽäĒ žĻėŽ£Ć Ūö®Í≥ľÍįÄ žěÖž¶ĚŽźėžĖī ŽĄźŽ¶¨ žā¨žö©ŽźėÍ≥† žěąŽč§[13]. Í∑łŽü¨Žāė Ūē≠žēĒžĻėŽ£ĆŽāė Žį©žā¨žĄ†žĻėŽ£Ć žěźž≤īÍįÄ žĚīžį®žĄĪ žõźŽįúžēĒžĚė žúĄŪóėžöĒžĚłžúľŽ°ú žěĎžö©Ūē† žąė žěąžĖī žĚīžóź ŽĆÄŪēú ŽßéžĚÄ žóįÍĶ¨ÍįÄ žčúŪĖČŽźėžĖīžôĒŽč§. žĶúÍ∑ľ žčúŪĖČŽźú žěĄžÉĀ žčúŪóėžóź ŽĒįŽ•īŽ©ī(RTOG 0234) ŽĎźÍ≤ĹŽ∂Ä ÍĶ≠žÜĆ žßĄŪĖČžĄĪ ŪéłŪŹČžĄłŪŹ¨žēĒ ŪôėžěźŽď§žĚĄ ŽĆÄžÉĀžúľŽ°ú žąėžą† ŽįŹ cisplatinÍ≥ľ cetuximab Ž≥ĎŪē© žöĒŽ≤ēžĚĄ žčúŪĖČŪēú ÍĶįžĚė žēĹ 8%žóźžĄú žĚīžį®žĄĪ žõźŽįúžēĒžĚī ŽįúžÉĚŪēėžėÄŽč§Í≥† Ž≥īÍ≥†Ūēú ŽįĒ žěąžúľŽāė[14], žĚīŽäĒ Íłįž°īžóź ŽĎźÍ≤ĹŽ∂ÄžēĒžóźžĄú žĚīžį®žĄĪ žõźŽįúžēĒ ŽįúžÉĚŽ•†žĚī žēĹ 8~20% ž†ēŽŹĄŽ°ú Ž≥īÍ≥†ŽźėžóąŽćė Í≤ÉÍ≥ľ žú†žā¨Ūēú Í≤įÍ≥ľžĚīŽč§[2,15]. žēĄžßĀÍĻĆžßÄ ÍĶ¨žĚłŽĎźžēĒžĚĄ ŪŹ¨Ūē®Ūēú ŽĎźÍ≤ĹŽ∂Ä žĘÖžĖϞ󟞥ú Ūē≠žēĒžĻėŽ£ĆÍįÄ žĚīžį®žĄĪ žõźŽįúžēĒžóź ŽĮłžĻėŽäĒ žėĀŪĖ•Ž†•žóź ŽĆÄŪēīžĄú ŽįĚŪėĞߥ ŽįĒŽäĒ ž†úŪēúž†ĀžĚīŽč§. ŽĒįŽĚľžĄú žīąžĻėŽ£ĆŽ°ú žąėžą†žĚĄ žĄ†ŪÉĚŪēú Í≤ĹžöįžôÄ CCRTŽ•ľ žčúŪĖČŪēú Í≤Ĺžöį, CCRTÍįÄ žĚīžį®žĄĪ žõźŽįúžēĒ ŽįúžÉĚ ŽįŹ žÉĚž°īŽ•†žóź ŽĮłžĻėŽäĒ žúĄŪóė žėĀŪĖ•žóź ŽĆÄŪēīžĄúŽäĒ Ž≥īŽč§ ŽßéžĚÄ žóįÍĶ¨ÍįÄ ŪēĄžöĒŪē† Í≤ÉžúľŽ°ú žÉĚÍįĀŽźúŽč§. ŪäĻŪěą HPV statusŽ•ľ ŪŹ¨Ūē®Ūēú biomarker ŽėźŪēú žĚīžį®žĄĪ žõźŽįúžēĒ ŽįúžÉĚžĚė ž§ĎžöĒ žúĄŪóė žöĒžĚłžúľŽ°ú žėąžÉĀŽźėŽäĒ ŽįĒ, žĚīŽ•ľ ŪŹ¨Ūē®Ūēú Žč§ÍįĀž†Ā žúĄŪóė žöĒžĚł Ž∂ĄžĄĚžĚĄ ŪÜĶŪēī žěĄžÉĀž†ĀžúľŽ°ú žĻėŽ£Ć Žį©Ž≤ē ž†Āžö©žóź ŽįėžėĀŪē† žąė žěąžĚĄ Í≤ÉžúľŽ°ú ÍłįŽĆÄŽźúŽč§.
žěĄžÉĀžĚėŽď§žĚÄ žĚľžį® žēĒ žßĄŽč® žčú HPV ÍįźžóľžĚī ŪôēžĚłŽźú ŪôėžěźžĚė Í≤Ĺžöį žĚīžį®žĄĪ žõźŽįúžēĒžĚĄ žĚľžúľŪā§ŽäĒ ŽŹÖŽ¶Ĺ žúĄŪóė žöĒžĚłžúľŽ°ú žěĎžö©Ūē† žąė žěąžúľŽĮÄŽ°ú HPV ÍīÄŽ†® žĚīžį®žĄĪ žõźŽįúžēĒžĚī Žč§žĖĎŪēú ŪēīŽ∂ÄŪēôž†Ā žúĄžĻėžóźžĄú ŽįúžÉĚŪē† žąė žěąžĚƞ̥ ž£ľžßÄŪēėžó¨ ž∂Ēž†Ā ÍīÄžįį žčú ž†Āž†ąŪēú Í≤Äžā¨Žď§žĚĄ žĄ†ŪÉĚŪēėžó¨ žčúŪĖČŪēėžó¨žēľ Ūē† Í≤ÉžĚīŽč§. ŽėźŪēú HPV žĖĎžĄĪžĘÖžĖĎ ŽįŹ žĚīžį®žĄĪ žõźŽįúžēĒžĚė ŽįúžÉĚ Íłįž†Ąžóź ŽĆÄŪēú žóįÍĶ¨Ž•ľ ŪÜĶŪēī žĚī žßąŪôėžóź ŪäĻžĚīž†ĀžĚł žĻėŽ£ĆŽ≤ē ÍįúŽįú ŽėźŪēú ÍįÄŽä•Ūē† Í≤ÉžúľŽ°ú žÉĚÍįĀŽźúŽč§.