м„ң лЎ
м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ(neurofibromatosis type 2, NF2)мқҖ 22лІҲ м—јмғүмІҙм—җ мһҲлҠ” NF2 мў…м–‘ м–өм ң мң м „мһҗмқҳ ліҖмқҙлЎң мқён•ҙ л§җмҙҲмӢ кІҪ лҳҗлҠ” мӨ‘추мӢ кІҪ мЎ°м§Ғм—җм„ң лӢӨл°ңм„ұ мў…м–‘мқҙ л°ңмғқн•ҳлҠ” л§Өмҡ° л“ңл¬ё м§ҲнҷҳмқҙлӢӨ. мғҒм—јмғүмІҙ мҡ°м„ұмңјлЎң мң м „лҗҳлҠ” м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмқҖ м•Ҫ 60000лӘ…лӢ№ 1лӘ… м •лҸ„мқҳ мң лі‘лҘ мқ„ ліҙмқҙл©°[1], мқҙ м§Ҳнҷҳм—җ мқҙнҷҳлҗң нҷҳмһҗл“ӨмқҖ мӢ кІҪкі„, лҲҲ, н”јл¶Җ лі‘ліҖмқҙ л°ңмғқн•ҳкІҢ лҗңлӢӨ. м–‘мёЎм„ұ м „м •мӢ кІҪмҙҲмў…(vestibular schwannoma)мқҖ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗм—җм„ң к°ҖмһҘ нқ”н•ҳкІҢ ліҙмқҙлҠ” мһ„мғҒ м–‘мғҒмқҙлӮҳ лӢӨлҘё лҮҢмӢ кІҪ, мІҷмҲҳмӢ кІҪ, л§җмҙҲмӢ кІҪм—җм„ңлҸ„ мӢ кІҪмҙҲмў…(schwannoma)мқҙ л°ңмғқн• мҲҳ мһҲлӢӨ. м–‘мёЎм„ұ м „м •мӢ кІҪмҙҲмў…мқҙ мһҲкұ°лӮҳ, мқјмёЎм„ұ м „м •мӢ кІҪмҙҲмў…мқё кІҪмҡ°м—җлҸ„ мҲҳл§үмў…(meningioma), мӢ кІҪкөҗмў…(glioma), мӢ кІҪ섬мң мў…(neurofibroma), л°ұлӮҙмһҘ(cataract)мқҙ мһҲлҠ” кІҪмҡ° м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмңјлЎң 진лӢЁн• мҲҳ мһҲлӢӨ. мһҗм„ён•ң 진лӢЁ кё°мӨҖмқҖ Table 1м—җ кё°мҲ н•ҳмҳҖлӢӨ[2,3].
мҳҒкөӯмқҳ мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳ(Genetic Severity Score) м§Җн‘ңлҠ” м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗл“Өмқҳ мң м „мһҗнҳ•м—җ л”°лқј н‘ңнҳ„нҳ•мқ„ 분лҘҳн•ң кІғмқҙлӢӨ(Table 2). лҸҢм—°ліҖмқҙм—җ л”°лқјм„ң мЎ°м§Ғ м„һмһ„мҰқ(tissue mosaicism), м „нҳ•м Ғ(classic), мӨ‘мҰқ(severe)мқҳ м„ё к°Җм§Җ 분лҘҳлЎң лӮҳлҲ„л©°, м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗл“Өмқҳ мҳҲнӣ„лҘј 추측н•ҳм—¬ нҷҳмһҗлҘј мғҒлӢҙн•ҳкұ°лӮҳ мҲҳмҲ м Ғ мІҳм№ҳлӮҳ м •мң„м Ғ л°©мӮ¬м„ м№ҳлЈҢлҘј кІ°м •н• л•Ң м°ёкі м§Җн‘ңлЎң мӮ¬мҡ©н•ңлӢӨ[4].
лҜёкөӯкіј мң лҹҪм—җм„ңлҠ” м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмқҳ мң м „нҳ•кіј н‘ңнҳ„нҳ•мқҳ м—°кҙҖм„ұмқҙ мһҳ к·ңлӘ…лҗҳм–ҙ мһҲлӢӨ. мқјл°ҳм ҒмңјлЎң м ҲлӢЁнҳ• лҸҢм—°ліҖмқҙ(truncating mutation)лҘј к°Җм§ҲмҲҳлЎқ мӢ¬н•ң мһ„мғҒ мҰқмғҒмқҙ лӮҳнғҖлӮҳл©°, м ҲлӢЁл¶Җ лҸҢм—°ліҖмқҙ(splice site mutation), мІҙм„ёнҸ¬ м„һмһ„мҰқ(somatic mosaicism), кіјмҳӨ лҸҢм—°ліҖмқҙ(missense mutation)мқё кІҪмҡ° мғҒлҢҖм ҒмңјлЎң лҠҰмқҖ лӮҳмқҙм—җ мҰқмғҒмқҙ лӮҳнғҖлӮҳлҠ” нҺёмқҙлқј м•Ңл Өм ё мһҲлӢӨ[5-9].
м Җмһҗл“Өмқҙ мЎ°мӮ¬н•ң л°”м—җ л”°лҘҙл©ҙ, м•„мӢңм•„м—җм„ңлҠ” м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмқҳ мң м „нҳ•мқҙ мғҲлЎӯкІҢ ліҙкі лҗң кІғ мҷём—җлҠ” мң м „нҳ•кіј н‘ңнҳ„нҳ•мқҳ м—°кҙҖм„ұм—җ лҢҖн•ҙ м—°кө¬лҗң мһҗлЈҢлҠ” м—ҶлҠ” мғҒнғңмқҙлӢӨ. мқҙм—җ ліё м—°кө¬м—җм„ң мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳ м§Җн‘ңлҘј мқҙмҡ©н•ҳм—¬ н•ңкөӯм—җм„ңмқҳ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗл“Өмқҳ мң м „нҳ•кіј н‘ңнҳ„нҳ• мӮ¬мқҙмқҳ м—°кҙҖм„ұмқ„ м•Ңм•„ліҙкі мһҗ н•ҳмҳҖлӢӨ.
лҢҖмғҒ л°Ҹ л°©лІ•
лҢҖ мғҒ
2010л…„ 1мӣ”~2020л…„ 5мӣ”к№Ңм§Җ мҲңмІңн–ҘлҢҖн•ҷкөҗ л¶ҖмІңлі‘мӣҗ мқҙ비мқёнӣ„кіјм—җ лӮҙмӣҗн•ң нҷҳмһҗ мӨ‘ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмңјлЎң 진лӢЁл°ӣмқҖ нҷҳмһҗ 27лӘ…мқҳ мқҳл¬ҙкё°лЎқкіј мң м „мһҗ кІҖмӮ¬ кІ°кіјлҘј нӣ„н–Ҙм ҒмңјлЎң 분м„қн•ҳмҳҖлӢӨ. мқҙл“Ө мӨ‘ мҳҒмғҒмқҳн•ҷм Ғ кІҖмӮ¬лҘј нҶөн•ҙ м–‘мёЎм„ұ м „м •мӢ кІҪмҙҲмў…мқҙ нҷ•мқёлҗң нҷҳмһҗ мӨ‘ 1л…„ мқҙмғҒ 추м Ғ кҙҖм°°н•ң нҷҳмһҗлҘј нҸ¬н•Ён•ҳмҳҖкі , мқјмёЎм„ұ м „м •мӢ кІҪмҙҲмў…мқ„ к°–кі мһҲкұ°лӮҳ мң м „мһҗ кІҖмӮ¬лҘј мӢңн–үн•ҳм§Җ м•ҠмқҖ нҷҳмһҗл“ӨмқҖ м ңмҷён•ҳмҳҖлӢӨ. к°Ғ нҷҳмһҗмқҳ мҷёлһҳ лӮҙмӣҗ лӢ№мӢң мЈј мҰқмғҒ, мІҳмқҢ 진лӢЁлҗң лӮ м§ң, мІӯл ҘкІҖмӮ¬, мҳҒмғҒмқҳн•ҷм Ғ кІҖмӮ¬ кІ°кіј, м•Ҳкіј 진лЈҢкё°лЎқм§Җ л“ұмқҳ мқҳл¬ҙкё°лЎқмқ„ нҶөн•ҙ мЎ°мӮ¬н•ҳмҳҖлӢӨ. ліё м—°кө¬лҠ” ліёмӣҗ м—°кө¬мңӨлҰ¬ мӢ¬мқҳ мң„мӣҗнҡҢ(Institutional Review Board, IRB)мқҳ мҠ№мқёмқ„ л°ӣм•„ мӢңн–үн•ҳмҳҖлӢӨ(IRB No. 2020-08-018).
мң м „мһҗ кІҖмӮ¬
к°Ғ нҷҳмһҗл“Өмқҳ л§җмҙҲ нҳҲм•Ўмқ„ мұ„м·Ён•ҳм—¬ мң м „мһҗ лҸҢм—°ліҖмқҙ кІҖмӮ¬лҘј мӢңн–ү нӣ„ мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳм—җ л”°лқј 분лҘҳн•ҳмҳҖлӢӨ. лҸҢм—°ліҖмқҙ кІҖмӮ¬лҠ” м§Ғм ‘ DNA м—јкё°м„ңм—ҙкІҖмӮ¬(direct DNA sequencing)мҷҖ лӢӨмӨ‘кІ°м°°мқҳмЎҙ н”„лЎңлёҢ мҰқнҸӯ(multiplex ligation-dependent probe amplification, MLPA)мқ„ мӮ¬мҡ©н•ҳмҳҖлӢӨ.
м§Ғм ‘ DNA м—јкё°м„ңм—ҙкІҖмӮ¬лҠ” нҷҳмһҗл“Өмқҳ л§җмҙҲнҳҲм•ЎмңјлЎңл¶Җн„° м–»мқҖ л°ұнҳҲкө¬мқҳ DNAлҘј мқҙмҡ©н•ҳмҳҖлӢӨ. Wizardв“Ү Genomic DNA Purification Kit(Promega, Madison, WI, USA)лҘј мқҙмҡ©н•ҳм—¬ 추м¶ңлҗң DNAлҠ” м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ мң м „мһҗмқҳ м „мІҙ мҪ”л”© мҳҒм—ӯ(exon 1-16)кіј м—‘мҶҗ-мқёнҠёлЎ (exon-intron) кІҪкі„лҘј м Ғм Ҳн•ң мӢңлҸҷмІҙ м„ёнҠё(primer set)лҘј мқҙмҡ©н•ҳм—¬ мӨ‘н•© нҡЁмҶҢ м—°мҮ„л°ҳмқ‘(polymerase chain reaction)мңјлЎң мҰқнҸӯмӢңмј°лӢӨ. к°Ғ мӨ‘н•© нҡЁмҶҢ м—°мҮ„ л°ҳмқ‘ мӮ°л¬јл“ӨмқҖ BigDye Terminator Cycle Sequencing Ready Reaction Kit(Applied Biosystems, Rotkreuz, Switzerland)лЎң мҲңнҷҳ мҲңм„ң кІ°м •(cycle sequencing) нӣ„ ABI Prism 3130 Genetic Analyzer(Applied Biosystems)мңјлЎң м „кё°мҳҒлҸҷмқ„ н•ҳмҳҖлӢӨ. л°ңкІ¬лҗң мң м „мһҗ ліҖмқҙлҠ” DNA sequence assembly software Sequencher 4.10.1(Gene Codes Corporation, Ann Arbor, MI, USA)мқ„ мқҙмҡ©н•ҳм—¬ 분м„қн•ҳмҳҖмңјл©°, GenBankмқҳ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ мӢңнҖҖмҠӨ(GenBank ID NM_000268.3)лҘј м°ёмЎ°м„ңм—ҙлЎң мӮ¬мҡ©н•ҳмҳҖлӢӨ.
лҸҢм—°ліҖмқҙ м„ңм—ҙмқҙ л°ңкІ¬лҗҳм§Җ м•Ҡкұ°лӮҳ, мӨ‘н•© нҡЁмҶҢ м—°мҮ„л°ҳмқ‘мқҙ мӢӨнҢЁн•ң кІҪмҡ°, нҒ° лҸҢм—°ліҖмқҙ(large mutation)лҘј нҷ•мқён•ҳкё° мң„н•ҙ, SALSA P044-NF2 Kit(MRC-Holland, Amsterdam, Netherlands)мқ„ мқҙмҡ©н•ҳм—¬ лӢӨмӨ‘кІ°м°°мқҳмЎҙ н”„лЎңлёҢ мҰқнҸӯ(MLPA)мқ„ мӢңн–үн•ҳмҳҖлӢӨ. ABI 9700 Thermal Cycler(Model 9700; Applied Biosystems, Foster City, CA, USA)лҘј мқҙмҡ©н•ҳм—¬ н”„лЎңлёҢ нҳјн•©л¬јкіј көҗмһЎн•ҳм—¬ кІ°н•©мӢңнӮЁ нӣ„ мӨ‘н•© нҡЁмҶҢ м—°мҮ„л°ҳмқ‘ мҰқнҸӯмқ„ н•ҳмҳҖмңјл©°, мӨ‘н•© нҡЁмҶҢ м—°мҮ„л°ҳмқ‘ мҰқнҸӯ мӮ°л¬јмқҖ ABI Prism 3130xl Genetic Analyzer(Applied biosystems)лҘј мқҙмҡ©н•ҳм—¬ м „кё°мҳҒлҸҷмқ„ мӢңн–үн•ҳкі GeneMarker 1.9 software(SoftGenetics, LLC, State College, PA, USA)лҘј нҶөн•ҙ 분м„қн•ҳмҳҖлӢӨ.
мІӯл ҘкІҖмӮ¬
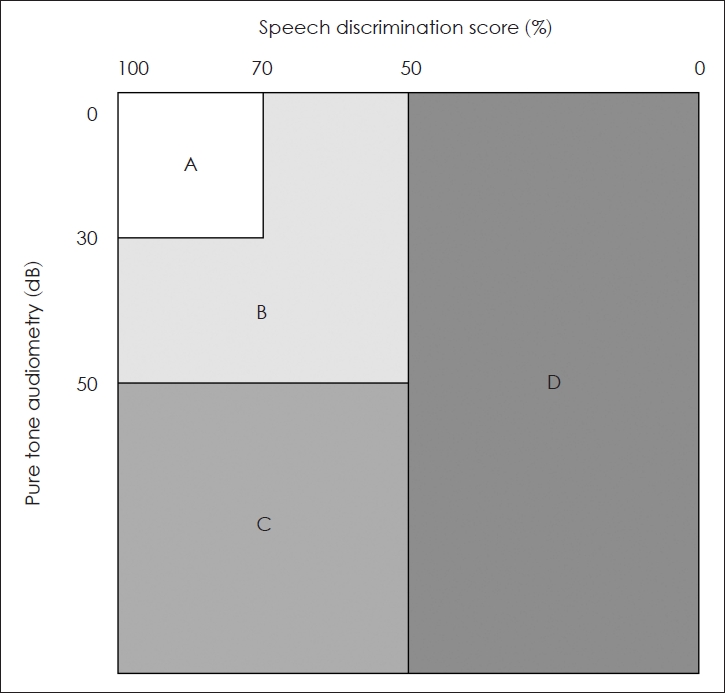
лӘЁл“ нҷҳмһҗл“ӨмқҖ лӮҙмӣҗ лӢ№мӢң мҲңмқҢмІӯл ҘкІҖмӮ¬мҷҖ м–ҙмқҢлӘ…лЈҢлҸ„кІҖмӮ¬лҘј мӢңн–үн•ҳмҳҖмңјл©°, мҲңмқҢмІӯл ҘкІҖмӮ¬лҠ” 0.5, 1, 2, 3 kHz мЈјнҢҢмҲҳмқҳ мІӯл Ҙм—ӯм№ҳмқҳ нҸүк· мңјлЎң кі„мӮ°н•ҳмҳҖкі , м–ҙмқҢлӘ…лЈҢлҸ„кІҖмӮ¬лҠ” лӢЁмқҢм Ҳ лӢЁм–ҙ лӘ©лЎқмқ„ нҷҳмһҗм—җкІҢ мқҪкІҢ н•ң л’Ө м •нҷ•нһҲ л°ңмқҢн•ң кІҪмҡ°лҘј нҚјм„јнҠёлЎң н‘ңмӢңн•ҳмҳҖлӢӨ. к°Ғ нҷҳмһҗл“Өмқҳ мҲңмқҢм—ӯм№ҳнҸүк· кіј м–ҙмқҢлӘ…лЈҢлҸ„ мҲҳм№ҳлҠ” American Academy of Otolaryngology-Head and Neck Surgery(AAO-HNS) 분лҘҳлІ•мқ„ мқҙмҡ©н•ҙ A, B, C, Dкө°мңјлЎң 분лҘҳн•ҳмҳҖлӢӨ(Fig. 1) [10]. мӮ¬нҡҢм Ғмқ‘мІӯл ҘмқҖ AAO-HNS 분лҘҳлІ•м—җм„ң мҲңмқҢм—ӯм№ҳнҸүк· мқҙ 50 dB HL лҜёл§Ңмқҙкі , м–ҙмқҢлӘ…лЈҢлҸ„к°Җ 50%лҘј мҙҲкіјн•ҳлҠ” Aкө°кіј Bкө°м—җ н•ҙлӢ№н•ҳлҠ” кө¬к°„мқҳ мІӯл ҘмңјлЎң м •мқҳн•ҳмҳҖлӢӨ.
мҳҒмғҒкІҖмӮ¬ л°Ҹ м•Ҳкіј 진лЈҢ кё°лЎқл¶Җ нҷ•мқё
нҷҳмһҗл“ӨмқҖ мІ« лӮҙмӣҗ лӢ№мӢң мЎ°мҳҒмҰқк°• мёЎл‘җкіЁ мһҗкё°кіөлӘ…мҳҒмғҒкіј мЎ°мҳҒмҰқк°• мІҷ추 мһҗкё°кіөлӘ…мҳҒмғҒмқ„ мҙ¬мҳҒн•ҳм—¬, м „м •мӢ кІҪмҙҲмў…мқҙлӮҳ мҲҳл§үмў…, мІҷ추종양 л“ұмқҙ мһҲлҠ”м§Җ нҸүк°Җн•ҳмҳҖлӢӨ. лҳҗн•ң нҷҳмһҗл“ӨмқҖ мөңмҙҲ лӮҙмӣҗ лӢ№мӢңл¶Җн„° мЈјкё°м Ғмқё м•ҲкіјкІҖ진мқ„ мӢңн–үн•ҳм—¬ л°ұлӮҙмһҘ, мӢңмӢ кІҪмҲҳл§үмў…(optic nerve meningioma), л§қл§үм „л§ү(epiretinal membrane), мӢңмӢ кІҪкөҗмў…(optic nerve glioma), л§қл§үкіјмҳӨмў…(retinal harmatoma) л“ұмқҳ м—¬л¶ҖлҘј нҷ•мқён•ҳмҳҖлӢӨ.
кІ° кіј
27лӘ…мқҳ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗл“Ө мӨ‘ ліё м—°кө¬м—җ нҸ¬н•Ёлҗң нҷҳмһҗлҠ” мҙқ 11лӘ…мңјлЎң, 2лӘ…мқҖ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ к°ҖмЎұл Ҙмқҙ мһҲм—Ҳкі (мӮ¬лЎҖ 8лІҲ, 10лІҲ), к·ё мҷё 9лӘ…мқҖ мӮ°л°ңм Ғ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмқҙм—ҲлӢӨ. нҷҳмһҗ м—°л №мқҖ 6~47м„ёлЎң лӢӨм–‘н•ҳкІҢ 분нҸ¬н•ҳмҳҖкі нҸүк· нҳ„мһ¬ м—°л №мқҖ 24.9м„ёмҳҖмңјл©°, мІ« 진лӢЁ мӢң нҸүк· м—°л №мқҖ 21.6м„ёмҳҖлӢӨ. лӮЁл…Җ 비мңЁмқҖ 6:5лЎң 비мҠ·н•ҳмҳҖкі , нҸүк· м¶”м Ғ кҙҖм°° кё°к°„мқҖ м•Ҫ 33к°ңмӣ”мқҙм—ҲлӢӨ. м–‘мёЎ мІӯл Ҙм—ӯм№ҳлҘј 비көҗн•ҳм—¬ мўӢмқҖ к·Җ(better ear)лҘј лҢҖмғҒмңјлЎң н–Ҳмқ„ л•Ң, AAO-HNS кё°мӨҖ Aкө°мқҖ 8лӘ…, Bкө°мқҖ 3лӘ…, Cкө°кіј Dкө°мқҖ к°Ғк°Ғ 0лӘ…мқҙм—ҲлӢӨ.
мң м „мһҗ кІҖмӮ¬м—җм„ңлҠ” 11лӘ… мӨ‘ 7лӘ…мқҳ нҳҲм•Ўм—җм„ң лҸҢм—°ліҖмқҙк°Җ нҷ•мқёлҗҳм—ҲлӢӨ. м—‘мҶҗ 2-13м—җ м ҲлӢЁнҳ• лҸҢм—°ліҖмқҙк°Җ мһҲлҠ” нҷҳмһҗ 4лӘ…, м—‘мҶҗ 1-7м—җ м ҲлӢЁл¶Җ лҸҢм—°ліҖмқҙк°Җ мһҲлҠ” нҷҳмһҗ 2лӘ…, к·ёлҰ¬кі н”„лЎңлӘЁн„°(promotor)лӮҳ м—‘мҶҗ 1м—җ кІ°мҶҗ лҸҢм—°ліҖмқҙк°Җ мһҲлҠ” нҷҳмһҗк°Җ 1лӘ…мқҙм—ҲлӢӨ. 11лӘ… мӨ‘ 2лӘ…мқ„ м ңмҷён•ҳкі 9лӘ…мқҳ м–‘мёЎ мІӯл Ҙмқҙ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙм—җ н•ҙлӢ№лҗҳм—ҲлӢӨ. лҳҗн•ң, 11лӘ… мӨ‘ 6лӘ…м—җкІҢм„ң м–‘мёЎм„ұ м „м •мӢ кІҪмҙҲмў… мҷём—җ мІҷ추종양мқҙ мЎҙмһ¬н•ҳмҳҖлӢӨ(Table 3).
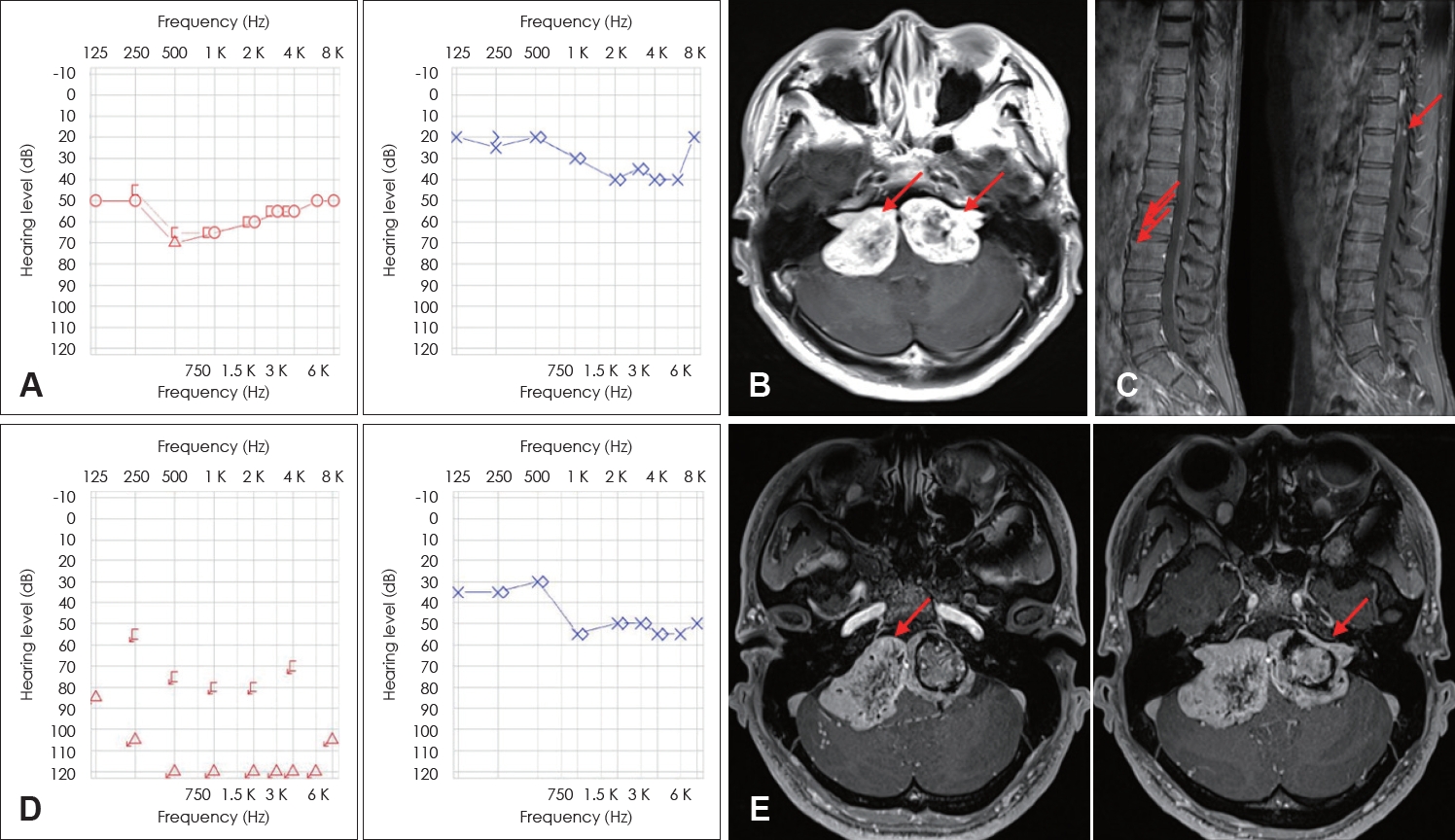
мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳм—җ л”°лқј нҷҳмһҗлҘј лӮҳлҲ„м—Ҳмқ„ л•Ң(Table 4), к·ёлЈ№ 1м—җлҠ” 4лӘ…мқҳ нҷҳмһҗк°Җ нҸ¬н•Ёлҗҳм—Ҳкі нҷҳмһҗл“Өмқҳ 진лӢЁ лӢ№мӢңмқҳ нҸүк· м—°л №мқҖ 33.3м„ёмҳҖлӢӨ. мқҙл“Ө мӨ‘ 2лӘ…мқҙ м–‘мёЎ к·Җ лӘЁл‘җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ к°Җм§Җкі мһҲм—Ҳкі , лӮҳлЁём§Җ 2лӘ…мқҖ мқјмёЎм—җм„ңл§Ң мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ ліҙмҳҖлӢӨ. мқҙл“Ө мӨ‘ н•ң лӘ…мқҙ 추м Ғ кҙҖм°° кё°к°„ лҸҷм•Ҳ AAO-HNS кё°мӨҖмңјлЎң м–‘мёЎ к·Җ лӘЁл‘җ Dкө°мңјлЎң мІӯл Ҙмқҙ м Җн•ҳлҗҳм—ҲлӢӨ(Fig. 2).
к·ёлЈ№ 2Aм—җ н•ҙлӢ№н•ҳлҠ” нҷҳмһҗлҠ” 1лӘ…мқҙм—ҲлӢӨ. мқҙ нҷҳмһҗмқҳ мІ« 진лӢЁ мӢңмқҳ м—°л №мқҖ 15.0м„ёмҳҖмңјл©°, мІӯл ҘмқҖ AAO-HNS Bкө°м—җ н•ҙлӢ№лҗҳм—ҲлӢӨ.
к·ёлЈ№ 2Bм—җлҠ” 2лӘ…мқҙ нҸ¬н•Ёлҗҳм—Ҳкі м§„лӢЁ лӢ№мӢңмқҳ м—°л №мқҖ к°Ғк°Ғ 3м„ё, 30м„ёмҳҖлӢӨ. 2лӘ…мқҳ лӘЁл‘җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙм—җ н•ҙлӢ№лҗҳм—ҲлӢӨ.
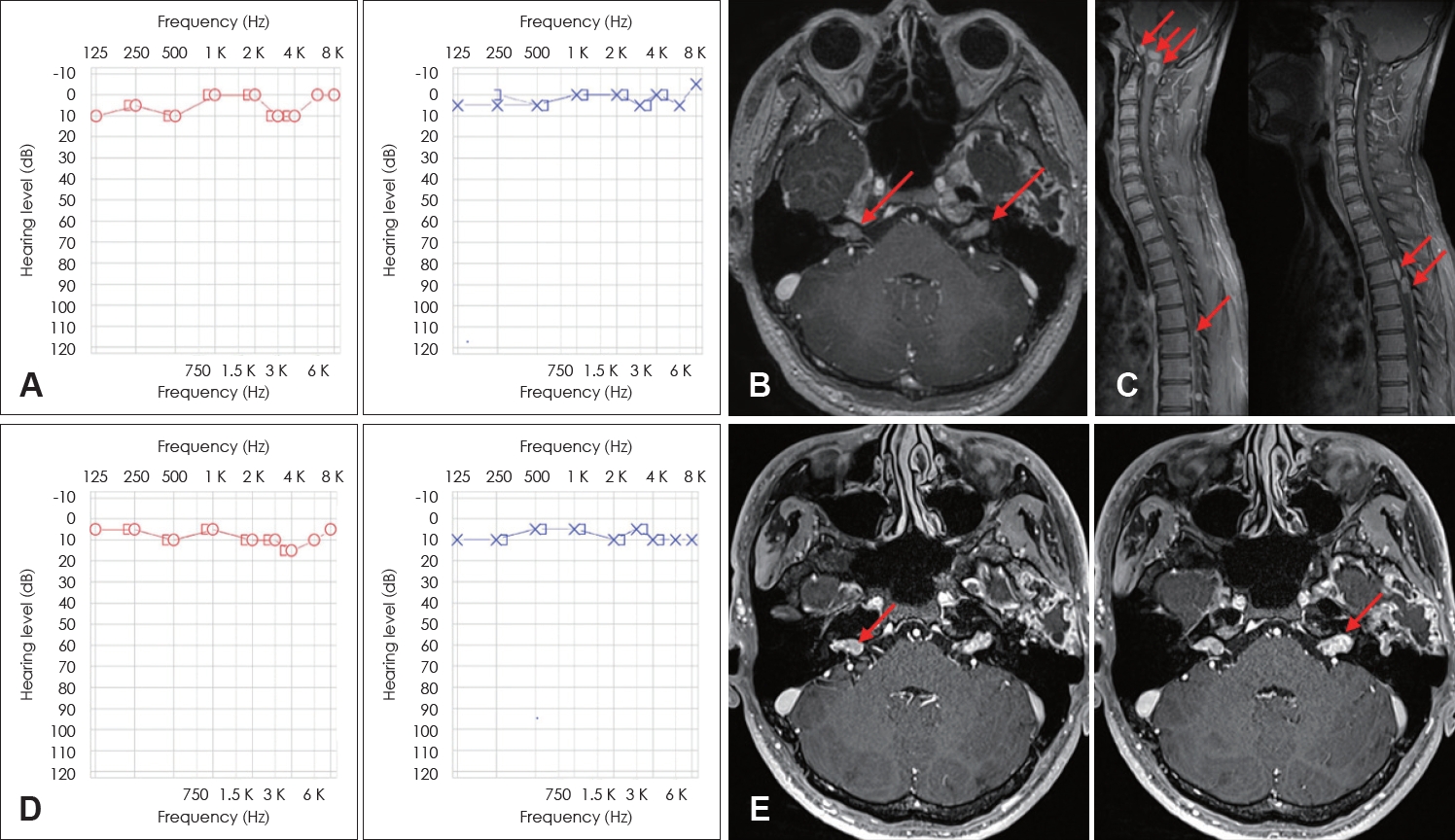
к·ёлЈ№ 3м—җлҠ” 4лӘ…мқҳ нҷҳмһҗк°Җ нҸ¬н•Ёлҗҳм—ҲлӢӨ. нҷҳмһҗл“Өмқҳ мІ« 진лӢЁ мӢңмқҳ нҸүк· м—°л №мқҖ 14.3м„ёмҳҖмңјл©°, мІӯл ҘмқҖ 4лӘ… лӘЁл‘җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙм—җ н•ҙлӢ№лҗҳм—ҲлӢӨ(Fig. 3).
к·ёлЈ№ 1м—җм„ңл§Ң мӢңл Ҙм Җн•ҳмҷҖ л°ұлӮҙмһҘ л“ұмқҳ м•Ҳкіјм Ғ мҰқмғҒмқҙ лҸҷл°ҳлҗң нҷҳмһҗк°Җ нҸ¬н•Ёлҗҳм—ҲлӢӨ. мҳҒмғҒмқҳн•ҷм Ғ кІҖмӮ¬м—җм„ң к·ёлЈ№ 1м—җ нҸ¬н•Ёлҗң 4лӘ… лӘЁл‘җ мІҷ추종양мқҙ лҸҷл°ҳлҗҳм—Ҳмңјл©°, к·ёлЈ№ 2BмҷҖ к·ёлЈ№ 3м—җм„ңлҠ” к°Ғк°Ғ н•ң лӘ…м”©л§Ң л°ңкІ¬лҗҳм—ҲлӢӨ.
мІ« мІӯл ҘкІҖмӮ¬м—җм„ң 17м„ё мқҙмғҒмқҙл©°, м–‘мёЎ к·Җ лӘЁл‘җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙм—җ н•ҙлӢ№лҗң 5лӘ…мқҖ 추м Ғ кҙҖм°° кё°к°„ лҸҷм•Ҳ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ мң м§Җн–ҲлӢӨ. 진лӢЁ мӢң н•ңмӘҪ к·ҖлқјлҸ„ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙм—җ н•ҙлӢ№н•ҳм§Җ м•ҠлҠ” нҷҳмһҗлҠ” 2лӘ…мқҙ мһҲм—Ҳкі лӘЁл‘җ к·ёлЈ№ 1м—җ н•ҙлӢ№н•ҳмҳҖлҠ”лҚ°, мқҙл“ӨмқҖ лӘЁл‘җ 추м Ғ кҙҖм°° кё°к°„ лҸҷм•Ҳ мІӯл Ҙм Җн•ҳ мҶҢкІ¬мқ„ ліҙмҳҖлӢӨ.
кі м°°
м ң2нҳ• мӢ кІҪ섬мң мў…мҰқмқҖ 22лІҲ м—јмғүмІҙмқҳ мһҘмҷ„м—җ мң„м№ҳн•ң NF2 мң м „мһҗмқҳ лҸҢм—°ліҖмқҙлЎң мқён•ҙ л°ңмғқн•ңлӢӨ. NF2 мң м „мһҗлҠ” л©ҖлҰ°(merlin)мқҙлқј л¶ҲлҰ¬лҠ” мў…м–‘м–өм ң лӢЁл°ұм§Ҳмқ„ кө¬м„ұн•ҳлҠ”лҚ°, мӢ кІҪкі„ лӮҙмқҳ мҠҲл°ҳм„ёнҸ¬м—җм„ң мғқм„ұлҗҳлҠ” л©ҖлҰ°мқҖ м„ёнҸ¬к°Җ л№ лҘё мҶҚлҸ„лЎң м„ұмһҘн•ҳкұ°лӮҳ л¶„н• н•ҳм§Җ лӘ»н•ҳкІҢ мЎ°м Ҳн•ҳлҠ” м—ӯн• мқ„ н•ңлӢӨ. NF2 мң м „мһҗк°Җ ліҖнҳ•лҗҳл©ҙ л©ҖлҰ°мқҙ м •мғҒм Ғмқё кё°лҠҘмқ„ мҲҳн–үн•ҳм§Җ лӘ»н•ҙ м„ёнҸ¬к°Җ л№ лҘҙкІҢ м„ұмһҘн•ҳкі л¶„м—ҙн•ҳм—¬ м–‘м„ұмў…м–‘мқ„ л°ңмғқмӢңнӮЁлӢӨ. м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗмқҳ м•Ҫ 95%м—җм„ң м–‘мёЎм„ұ м „м •мӢ кІҪмҙҲмў…мқҙ л°ңмғқн•ңлӢӨкі м•Ңл Өм ё мһҲмңјл©°, лӮңмІӯ, мқҙлӘ…, м–ҙм§ҖлҹјмҰқмқ„ мЈјлЎң нҳёмҶҢн•ңлӢӨ. ліё м—°кө¬м—җ нҸ¬н•Ёлҗң нҷҳмһҗл“Өм—җм„ңлҸ„ м Ҳл°ҳ мқҙмғҒм—җм„ң лӮңмІӯ, мқҙлӘ… л“ұмқҳ к·Җ мҰқмғҒл“Өмқ„ мЈј мҰқмғҒмңјлЎң нҳёмҶҢн•ҳмҳҖлӢӨ.
м ң2нҳ• мӢ кІҪ 섬мң мў…мҰқмқҖ м№ҳлЈҢ л°©м№Ёмқ„ кІ°м •н•ҳкё° л§Өмҡ° м–ҙл Өмҡҙ м§Ҳлі‘мқҙлӢӨ. мң м „мһҗнҳ•-н‘ңнҳ„нҳ•мқҳ мғҒкҙҖкҙҖкі„м—җ лҢҖн•ң м—°кө¬л“Өмқ„ кё°л°ҳмңјлЎң нҷҳмһҗмқҳ мң м „нҳ•м—җ к·јкұ°н•ң мҳҲнӣ„ мҳҲмёЎмқҖ лҸ„мӣҖмқҙ лҗ мҲҳ мһҲлӢӨ. мҳҒкөӯмқҳ мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳм—җ лҢҖн•ҙ 진н–үлҗң м„ н–ү м—°кө¬м—җ л”°лҘҙл©ҙ мң м „м Ғ мӨ‘мҰқлҸ„мҷҖ мІ« 진лӢЁ мӢңмқҳ лӮҳмқҙмҷҖ нҳ„мһ¬ лӮҳмқҙлҠ” мқҢмқҳ мғҒкҙҖкҙҖкі„лҘј к°Җм§Җл©°, мІ« 진лӢЁ мӢң нҸүк· лӮҳмқҙлҠ” к·ёлЈ№ 1мқҳ кІҪмҡ° 47.0м„ё, к·ёлЈ№ 3мқҳ кІҪмҡ° 15.9м„ёлЎң м•Ңл Өм ё мһҲлӢӨ. лҳҗн•ң мң м „м Ғ мӨ‘мҰқлҸ„к°Җ лҶ’мқҖ к·ёлЈ№мқјмҲҳлЎқ мІҷ추종양мқҳ л°ңкІ¬ л№ҲлҸ„к°Җ лҶ’м•ҳмңјл©°, м•Ҳкіјм Ғ м§Ҳнҷҳкіј мІӯл Ҙм Җн•ҳ лҳҗн•ң м„ нҳ• кІҪн–Ҙм„ұмқ„ ліҙмқёлӢӨкі ліҙкі лҗҳм—ҲлӢӨ[4].
ліё м—°кө¬м—җм„ңлҠ” к·ёлЈ№ 1мқҳ мІ« 진лӢЁ мӢң нҸүк· м—°л №мқҖ 33.3м„ё, к·ёлЈ№ 3мқҳ мІ« 진лӢЁ мӢң нҸүк· м—°л №мқҖ 14.3м„ёлЎң м•һм„ м—°кө¬мҷҖ 비мҠ·н•ң кІҪн–Ҙм„ұмқ„ ліҙмҳҖлӢӨ. к·ёлҹ¬лӮҳ мІӯл Ҙмқҳ кІҪмҡ° к·ёлЈ№ 3м—җ нҸ¬н•Ёлҗң 4лӘ… лӘЁл‘җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ к°Җм§Җкі мһҲм—Ҳмңјл©°, мҳӨнһҲл Ө к·ёлЈ№ 1м—җм„ң мқјмёЎмқҳ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙм—җ нҸ¬н•Ёлҗҳм§Җ м•ҠлҠ” мІӯл Ҙмқ„ к°Җ진 нҷҳмһҗк°Җ л‘җ лӘ… нҸ¬н•Ёлҗҳм—ҲлӢӨ. м•Ҳкіјм Ғ м§Ҳнҷҳмқ„ к°Җ진 нҷҳмһҗлҠ” к·ёлЈ№ 1м—җм„ңл§Ң л°ңкІ¬лҗҳм—Ҳмңјл©°, к·ёлЈ№ 1мқҳ нҷҳмһҗл“Өм—җкІҢм„ң лӘЁл‘җ мІҷ추종양мқҙ нҷ•мқёлҗҳм–ҙ, 1лӘ…м—җкІҢм„ңл§Ң мІҷ추종양л§Ң нҷ•мқёлҗң к·ёлЈ№ 3кіјлҠ” лҢҖ비лҗҳлҠ” лӘЁмҠөмқ„ ліҙмҳҖлӢӨ. м „мІҙм ҒмңјлЎң к·ёлЈ№ 1 нҷҳмһҗкө°мқҙ к·ёлЈ№ 3 нҷҳмһҗкө°ліҙлӢӨ мӢ¬к°Ғн•ң мһ„мғҒм–‘мғҒмқ„ ліҙм—¬, кё°мЎҙ ліҙкі лҗң м—°кө¬мқҳ кІ°кіјмҷҖлҠ” лӢӨлҘё кІҪн–Ҙм„ұмқ„ лқ м—ҲлӢӨ.
мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳмҷҖ мІӯл Ҙмқҳ кҙҖкі„лҘј м—°кө¬н•ң лӢӨлҘё н•ң м—°кө¬м—җм„ңлҠ” мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳм—җ л”°лқј, мЎ°м§Ғ м„һмһ„мҰқ к·ёлЈ№м—җм„ңлҠ” AAO-HNS Aкө°мқё нҷҳмһҗк°Җ 64% к°Җлҹү лҗҳм—ҲмңјлӮҳ, мӨ‘мҰқ к·ёлЈ№м—җм„ңлҠ” м Ҳл°ҳ мқҙмғҒмқҳ нҷҳмһҗк°Җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ мһғм–ҙлІ„л ёкі , 35%л§Ңмқҙ AAO-HNS Aкө°м—җ н•ҙлӢ№лҗҳм—ҲлӢӨ[11]. ліё м—°кө¬м—җм„ңлҠ” мЎ°м§Ғ м„һмһ„мҰқ к·ёлЈ№ мӨ‘ AAO-HNS Aкө°м—җ н•ҙлӢ№н•ҳлҠ” нҷҳмһҗлҠ” 4лӘ… мӨ‘ 2лӘ…, мӨ‘мҰқ к·ёлЈ№м—җм„ң Aкө°м—җ н•ҙлӢ№н•ҳлҠ” нҷҳмһҗлҠ” 4лӘ… мӨ‘ 4лӘ…мқҙм—ҲлӢӨ. мқҙлҠ” кё°мЎҙ м—°кө¬мҷҖ м°Ёмқҙм җмқ„ ліҙмқҙлҠ” кІ°кіјмқҙлӮҳ лҢҖмғҒ нҷҳмһҗ мҲҳк°Җ м Ғм–ҙ 추к°Җм Ғмқё м—°кө¬к°Җ н•„мҡ”н• кІғмңјлЎң ліҙмқёлӢӨ.
мқҙм „ м—°кө¬м—җ л”°лҘҙл©ҙ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗл“ӨмқҖ лӮҳмқҙк°Җ л“Өм–ҙк°җм—җ л”°лқј мІӯл Ҙмқҙ л–Ём–ҙм§ҖлҠ” лӘЁмҠөмқ„ ліҙмқҙлҠ”лҚ°, мЎ°м§Ғ м„һмһ„мҰқ к·ёлЈ№мқҳ нҷҳмһҗл“Ө мӨ‘ м Ҳл°ҳмқҖ 80м„ёк№Ңм§Җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ мң м§Җн•ҳлӮҳ кІҪлҸ„мҷҖ мӨ‘л“ұлҸ„ к·ёлЈ№м—җм„ңлҠ” 44~46м„ё, мӨ‘мҰқ к·ёлЈ№м—җм„ңлҠ” 32м„ём—җ м Ҳл°ҳмқҳ нҷҳмһҗк°Җ мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ мһғм–ҙлІ„лҰ°лӢӨкі н•ҳмҳҖлӢӨ[11].
ліё м—°кө¬м—җм„ң мІ« 진лӢЁ мӢң 17м„ё мқҙмғҒмқҙл©° м–‘мёЎ к·Җ лӘЁл‘җ AAO-HNS Aкө°м—җ н•ҙлӢ№лҗң 5лӘ…мқҖ 추м Ғ кҙҖм°° кё°к°„ лҸҷм•Ҳ м •мғҒмІӯл Ҙмқ„ мң м§Җн•ҳмҳҖмңјл©° к°ҖмһҘ кёҙ 추м Ғ кҙҖм°° кё°к°„мқҖ 35к°ңмӣ”мқҙм—ҲлӢӨ. мқҙм „ м—°кө¬кІ°кіјмҷҖ лӢӨлҘҙкІҢ м—°л №м—җ л”°лқј мІӯл Ҙм Җн•ҳк°Җ 진н–үлҗҳлҠ” лӘЁмҠөмқ„ ліҙмқҙм§Җ м•Ҡм•ҳмңјлӮҳ, нҷҳмһҗл“Өмқҳ лӮҳмқҙк°Җ мқҙм „ м—°кө¬мқҳ к°Ғ кө°м—җ л”°лҘё мӮ¬нҡҢм Ғмқ‘мІӯл Ҙмқ„ мһғм–ҙлІ„лҰ¬лҠ” нҸүк· м—°л №лҢҖм—җ лҜём№ҳм§Җ лӘ»н•ҳлҜҖлЎң ліҙлӢӨ мһҘкё°к°„мқҳ 추м Ғ кҙҖм°°мқҙ н•„мҡ”н• кІғмңјлЎң ліҙмқёлӢӨ.
ліё м—°кө¬лҠ” лҸҷм–‘мқём—җм„ң мң м „м Ғ мӨ‘мҰқлҸ„ м җмҲҳлҘј мқҙмҡ©н•ҳм—¬ м ң 2нҳ• мӢ кІҪ섬мң мў…мҰқмқҳ мң м „мһҗнҳ•кіј н‘ңнҳ„нҳ•мқҳ м—°кҙҖм„ұм—җ лҢҖн•ҙ м—°кө¬н•ң мІ« л…јл¬ёмқҙлқјлҠ” мқҳлҜёк°Җ мһҲлӢӨ. кІ°кіјм ҒмңјлЎң м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗл“ӨмқҖ мң м „мһҗнҳ•кіј н‘ңнҳ„нҳ•мқҙ кё°мЎҙм—җ м•Ңл Ө진 м—°кө¬л“Өкіј мқјм№ҳн•ҳм§Җ м•ҠлҠ” кІғмңјлЎң лӮҳнғҖлӮ¬лӢӨ. лҳҗн•ң мІ« 진лӢЁ мӢңм—җ мӮ¬нҡҢм Ғмқ‘ мІӯл Ҙмқ„ к°Җм§Җкі мһҲлӢӨл©ҙ мң м „мһҗнҳ•кіј мғҒкҙҖм—Ҷмқҙ мІӯл Ҙмқ„ мң м§Җн• мҲҳ мһҲлҠ” кІғмңјлЎң мғқк°ҒлҗңлӢӨ.
ліё м—°кө¬мқҳ м ңн•ңм җмңјлЎңлҠ” лӢЁмқј кё°кҙҖ м—°кө¬мқҙкі , нҷҳмһҗ мҲҳк°Җ л§Өмҡ° м Ғм—Ҳкё° л•Ңл¬ём—җ, н•ңкөӯ м ң2нҳ• мӢ кІҪ섬мң мў…мҰқ нҷҳмһҗмқҳ мң м „мһҗ нҳ•кіј н‘ңнҳ„нҳ•мқҳ кҙҖкі„м—җ лҢҖн•ң кІ°лЎ мқ„ лҸ„м¶ңн•ҳлҠ” лҚ° н•ңкі„к°Җ мһҲм—ҲлӢӨ. м•һмңјлЎң лӢӨкё°кҙҖ м—°кө¬ л“ұмқ„ нҶөн•ҙ лҚ” л§ҺмқҖ нҷҳмһҗ мһҗлЈҢлҘј мқҙмҡ©н•ҳм—¬ мқёмў…к°„мқҳ м°ЁмқҙлӮҳ нӣ„м„ұм Ғ мҡ”мқёл“Өмқ„ н•Ёк»ҳ 분м„қн•ҳлҠ” 추к°Җ м—°кө¬к°Җ н•„мҡ”н• кІғмңјлЎң ліҙмқёлӢӨ.