мДЬ л°†
лСРк≤љлґАмЭШ мЮђк±імИШмИ†мЭД мЛЬнЦЙнХ† лХМмЧРлКФ мЧђлЯђк∞АмІА мЭЄмЮРлУ§мЭД к≥†л†§нХімХЉ нХЬлЛ§. лСРк≤љлґАмХФмЭД м†Им†ЬнХЬ нЫД мЮђк±імЭА к≥µмЧђлґАмЬДлВШ мИШнШЬлґАмЬДмЭШ нЪМл≥µмЭі лє®л¶ђ мЭіл£®мЦімІИ мИШ мЮИмЦімХЉ нХШл©∞, мҐЕмЦСмЭД м†Им†ЬнХШк≥† лВШмДЬ л∞ЬмГЭнХШлКФ 3м∞®мЫРм†Б кµђм°∞л•Љ к∞АмІАлКФ к≤∞мЖРмЭД м†Бм†ИнХШк≤М л≥µмЫРнХімХЉ кЄ∞лК•м†БмЬЉл°Ь мЧ∞нХШ, л∞ЬмД±, нЭ°мЭЄл∞©мІА лУ± л≥µмЮ°нХЬ кЄ∞лК•мЭД л≥ім°інХ† мИШ мЮИлЛ§[1]. мД±к≥µм†БмЭЄ мЮђк±імЭД мЬДнХі лСРк≤љлґАмЭШ лЛ§мЦСнХЬ мГЭл¶ђм†Б кЄ∞лК•к≥Љ нКємД±мЭД мЭінХінХШк≥† мЭіл•Љ мµЬлМАнХЬ л≥ім°інХШл©∞ кЄ∞лК•мЭД мЬ†мІАнХ† мИШ мЮИмЦімХЉ нХЬлЛ§[2]. мІДнЦЙлРЬ лСРк≤љлґАмХФмЭШ к≤љмЪ∞ мҐЕмЦСмЭД мХИм†ДнХШк≤М лЕЄмґЬнХШкЄ∞ мЬДнХі нХШмХЕ/нХШмИЬмЭД м†Ик∞ЬнХШк±∞лВШ кµђк∞Хм†А нШємЭА мЭЄлСРл•Љ кµђмД±нХШлКФ кЈЉмЬ°мЭД м†Ик∞ЬнХШлКФ мИ†мЛЭмЭі нХДмЪФнХ† мИШ мЮИлЛ§[3]. лШРнХЬ мЭілЯђнХЬ мИ†мЛЭмЭА м†Бм†ИнХЬ мЬ†л¶ђнФЉнМР мЮђк±і, нКєнЮИ нФЉнМРмЭД м†Им†ЬлґАмЬДмЧР мВљмЮЕнХШкЄ∞ мЬДнХі нХДмЪФнХЬ к≥Љм†ХмЭЉ мИШлПД мЮИлЛ§. нХШмІАлІМ мЭілЯђнХЬ мє®мКµм†БмЭЄ мИ†мЛЭмЭА м†ХмГБм°∞мІБмЭД мЖРмГБмЛЬмЉЬ, мИ†нЫД лІОмЭА нХ©л≥См¶ЭмЭД мЬ†л∞ЬнХ† мИШ мЮИмЬЉл©∞, мИШмИ† л∞П мИ†нЫД нХ≠мХФ/л∞©мВђмД†мєШл£М нЫД кЄ∞лК•м†БмЭЄ м†АнХШл°Ь мЭімЦімІИ мИШ мЮИлЛ§[4]. лФ∞лЭЉмДЬ мµЬкЈЉ лІОмЭА лСРк≤љлґАмЩЄк≥ЉмЭШлУ§мЭА мЭілЯђнХЬ мє®мКµм†БмЭЄ мИ†мЛЭл≥ілЛ§лКФ к≤љкµђк∞ХмИ†мЛЭ(transoral approach)мЭД нПђнХ®нХЬ лЛ§мЦСнХЬ мµЬмЖМ мє®мКµ мИ†мЛЭ(minimally invasive procedure)мЭД мД†нШЄнХЬлЛ§[5].
мµЬмЖМ мє®мКµ мИ†мЛЭмЭД мЭімЪ©нХЬ м†Им†Ь нЫД к≤∞мЖР лґАмЬДлКФ мЬ†л¶ђнФЉнМРмЭД мЭімЪ©нХЬ мЮђк±і мЛЬ кЄ∞мИ†м†БмЭЄ мֳ놧мЫА, нКєнЮИ нФЉнМРмЭД мВљмЮЕнХШлКФ к≥Љм†ХмЭШ мֳ놧мЫАмЭД мЬ†л∞ЬнХЬлЛ§. лСРк≤љлґАмЭШ мҐБк≥†, кєКмЭА к≤∞мЖРлґАмЬДмЭШ к≤љмЪ∞, нФЉнМРмЭД м†ХнЩХнХШк≤М мЬДмєШмЛЬмЉЬ ліЙнХ©нХШкЄ∞к∞А мֳ놧мЪ∞л©∞, нФЉнМРк≥Љ м†РлІЙмЭШ м†Им†ЬмЧ∞мЭД м†ХнЩХнХШк≤М лІЮмґФмЦі ліЙнХ©нХШмІА л™їнХі мєШмЬ†к∞А мІАмЧ∞лР† мИШ мЮИлЛ§. лШРнХЬ мИШмИ†к≥Љм†ХмЧРмДЬмЭШ к≥ЉлПДнХЬ м°∞мЮС(repeated flap manipulation) л∞П к≥ЉмЛ†м†ДмЭі л∞ЬмГЭнХ† мИШ мЮИмЬЉл©∞, нШИкіАк≤љмЭД мЬДмєШмЛЬнВ§к±∞лВШ нШИкіАлђЄнХ©мЭД мЛЬнЦЙнХ† лХМ кЇЊмЭік±∞лВШ мЖРмГБмЭД м§Д мИШлПД мЮИлЛ§.
вАЬнМ®лЯђмКИнКЄвАЭ кЄ∞л≤ХмЭА мЛђмЮ•нШИкіАмЩЄк≥Љ мИШмИ† мЛЬ мВђмЪ©лРШлКФ ліЙнХ©кЄ∞л≤ХмЬЉл°Ь нШИкіАмЭілВШ нМРлІЙмєШнЩШмИ† мЛЬ мҐБмЭА мИШмИ† лґАмЬДмЧРмДЬ м†ХнЩХнХЬ ліЙнХ©мЭД мЬДнХі мВђмЪ©лРЬлЛ§[6,7]. нМ®лЯђмКИнКЄ кЄ∞л≤ХмЭА нШИкіАмЭілВШ ліЙнХ©нХ† м†Ик∞ЬмЭШ лґАмЬДк∞А кєКмЭА к≤љмЪ∞ мВђмЪ©лРШлКФлН∞, мЧђлЯђ л∞ФмЭінКЄ(bite)л•Љ мЬДмєШмЛЬнВ® нЫД к≤∞м∞∞нХШмІА мХКмЭА мГБнГЬл°Ь л®Љм†А лЖФлСРк≥† мІДнЦЙнХШл©∞, мЧђлЯђк∞ЬмЭШ л∞ФмЭінКЄл•Љ ліЙнХ©нХ† лСР к∞ЬмЭШ нШИкіАмЧР мЬДмєШмЛЬнВ® нЫД лСР к∞ЬмЭШ нШИкіАмЭі лВЩнХШмВ∞м≤ШлЯЉ м†Ик∞ЬлґАл°Ь л³놧мШ§л©імДЬ лІЮлПДл°Э лФФмЮРмЭЄнХШмЧђ мЦСм™љ лБЭмЭД лПЩмЛЬмЧР мЮ°мХДлЛєк≤® ліЙнХ©нХШк≤М лРЬлЛ§[8].
мЭімЧР м†АмЮРлКФ нМ®лЯђмКИнКЄ кЄ∞л≤ХмЭД нЩЬмЪ©нХЬ лСРк≤љлґА мЬ†л¶ђнФЉнМР мЮђк±імИШмИ†, нКєнЮИ нФЉнМРмЭД мҐБк≥†, кєКмЭА к≤∞мЖРлґАмЬДмЧР мЬДмєШмЛЬнВђ мИШ мЮИлКФ мЮђк±імИШмИ†мЭШ м§АлєДмЩА мИШмИ† к≥Љм†ХмЭД м†АмЮРмЭШ к≤љнЧШк≥Љ нХ®кїШ мЖМк∞ЬнХШк≥†мЮР нХЬлЛ§.
л∞© л≤Х
к≤∞мЖРлґАмЬД ліЙнХ©(Suture through the edge of surgical defect)
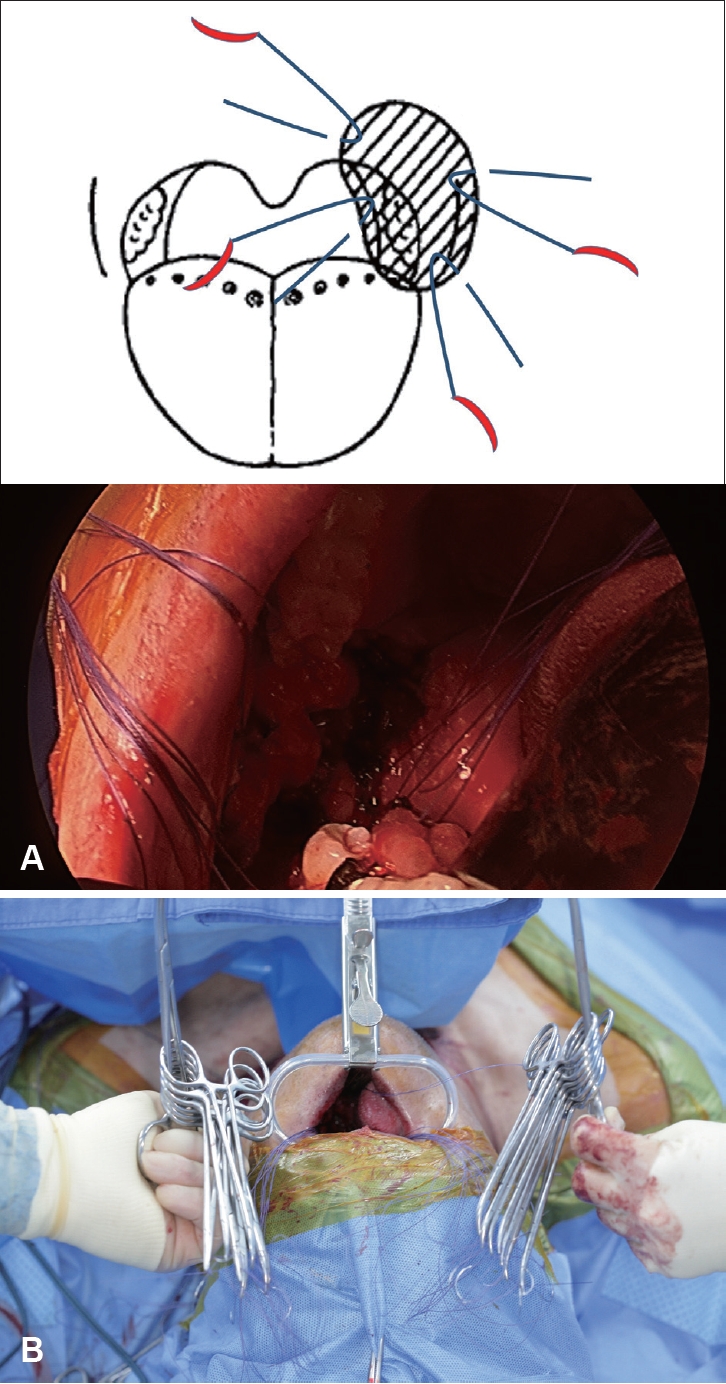
к≤љлґАл¶ЉнФДм†И м†Им†ЬмИ†(neck dissection) л∞П лСРк≤љлґАмХФ мЫРл∞ЬлґАмЬД м†Им†ЬмИ†мЭД лІИмєШк≥† лВШл©і мЬ†л¶ђнФЉнМРмЭД к±∞мГБнХШкЄ∞ м†Д к≤∞мЖРлґАмЬД ліЙнХ©мЭД мЛЬмЮСнХШк≤М лРЬлЛ§. нЧИнШИмЛЬк∞Д(ischemic time)мЭД м§ДмЭікЄ∞ мЬДнХі нФЉнМРк±∞мГБ м†Д м†Им†ЬмЧ∞мЭШ ліЙнХ©мЭД л®Љм†А мЛЬнЦЙнХЬлЛ§. м†Им†ЬмЧ∞мЭШ м†РлІЙ(mucosal edge of surgical defect)мЭД л∞ФлКШмЭД лґДл¶ђнХ† мИШ мЮИлКФ 3-0 нЭ°мИШмД± ліЙнХ©мВђ(vicrylвУЗ 3-0 pop-off suture)л•Љ мЭімЪ©нХШмЧђ л∞ФмЭінКЄ(bite)л•Љ мЛЬнЦЙнХЬ нЫД л™®мК§нВ§нЖ† нБілЮ®нФД(mosquito surgical clamp) лУ±мЭД мЭімЪ©нХШмЧђ к≥†м†ХнХілСФлЛ§(Fig. 1A and Supplementary Video 1). мЭілХМ мЛ§(string)мЭШ мИЬмДЬк∞А л∞ФлАМмІА мХКлПДл°Э м£ЉмЭШнХімХЉ нХЬлЛ§. л≥інЖµ мҐМмЪ∞л•Љ лВШлИДмЦі ліЙнХ©мВђлУ§мЭД лСР к∞Ь нШємЭА мДЄ к∞ЬмЭШ кЈЄл£ємЬЉл°Ь лВШлИДмЦі к≥†м†ХнХілСРлКФ к≤ГмЭі лВШм§СмЧР нФЉнМРмЭД мВљмЮЕнХ† лХМ кµђлґДмЭі мЪ©мЭінХШл©∞ ліЙнХ©мВђмЭШ л∞ФлКШмЭі лЦ®мЦімІАмІА мХКлПДл°Э м£ЉмЭШнХЬлЛ§(Fig. 1B). мЭінЫД к≥ДнЪНлРЬ мЬ†л¶ђ нФЉнМРмЭШ к±∞мГБмЭД мЛЬмЮСнХЬлЛ§.
нФЉнМР мВљмЮЕ л∞П ліЙнХ©(Flap inset and suture through the flap)
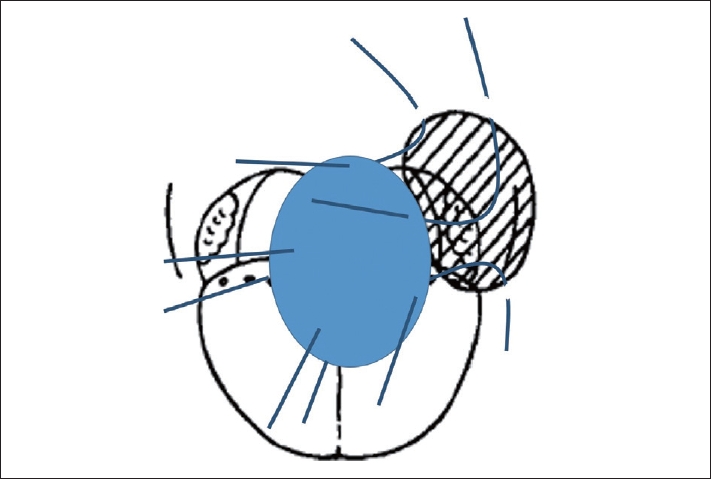
нФЉнМРмЭД к±∞мГБнХЬ мЭінЫД, нФЉнМРмЭД лСРк≤љлґА к≤∞мЖРлґАмЬДмЧР мЬДмєШмЛЬнВ®лЛ§. нШИкіАк≤љ(pedicle)мЭД лђЄнХ©нХ† нШИкіАлґАмЬД, мГБк∞СмГБлПЩлІ•(superior thyroidal artery)мЭілВШ мХИл©ілПЩлІ•(facial artery) лУ± м£Љл≥АмЧР мЬДмєШмЛЬнВ® нЫД нФЉнМРк≥Љ к≤∞мЖРлґАмЬДмЭШ ліЙнХ©мЭД мЛЬмЮСнХЬлЛ§. мЭілѓЄ к≤∞мЖРлґАмЬДмЧР мЬДмєШнХЬ ліЙнХ©мВђл•Љ мИЬмДЬмЧР лІЮмґФмЦі нФЉнМРмЧР л∞ФмЭінКЄл•Љ нХЬ мЭінЫД ліЙнХ©мВђмЭШ л∞ФлКШмЭД лЛєк≤®мДЬ м†Ьк±∞нХШк≥†, лЛ§мЛЬ нХЬ л≤И мИЬмДЬмЧР лІЮмґФмЦі л™®мК§нВ§нЖ† нБілЮ®нФДл•Љ мЭімЪ©нХі к≥†м†ХнХЬлЛ§(Fig. 2 and Supplementary Video 1). мЭілХМ ліЙнХ©мЭА кµђк∞Х л∞Фкє•мЭШ лДУмЭА к≥µк∞ДмЧРмДЬ нФЉнМРмЭШ м†Бм†ИнХЬ мЬДмєШл•Љ мХИм†ДнХШк≤М нЩХмЭЄнХЬ нЫД мЛЬнЦЙнХ† мИШ мЮИлЛ§. л™®лУ† ліЙнХ©мВђмЭШ л∞ФмЭінКЄл•Љ мЛЬнЦЙнХЬ мЭінЫДмЧР ліЙнХ©мВђмЭШ к≤∞м∞∞ лЛ®к≥Дл°Ь мІДнЦЙнХЬлЛ§. мЭілХМ мЧ≠мЛЬ мЛ§мЭШ мИЬмДЬ л∞П мҐМмЪ∞к∞А нШЉлПЩлРШмІА мХКлПДл°Э мЮШ кµђлґДнХі лСРлКФ к≤ГмЭі лІ§мЪ∞ м§СмЪФнХШлЛ§.
ліЙнХ©мВђ к≤∞м∞∞(Tie the knot of unlocked strings)
кµђк∞Х л∞Фкє•м™љ лДУмЭА к≥µк∞ДмЧРмДЬ ліЙнХ©мЭД мЛЬнЦЙнХЬ нФЉнМРмЭД к≤∞мЖРлґАмЬДл°Ь м†Бм†ИнХШк≤М л∞АмЦі лД£мЭА мЭінЫД мИЬмДЬлМАл°Ь к≤∞м∞∞нХШмІА мХКмЭА ліЙнХ©мВђмЭШ к≤∞м∞∞мЭД мИЬм∞®м†БмЬЉл°Ь мЛЬнЦЙнХЬлЛ§. мЭілѓЄ м†Им†ЬмЧ∞к≥Љ нФЉнМРмЭШ л∞ФмЭінКЄлКФ м†Бм†ИнХЬ мЬДмєШмЧР мЬДмєШмЛЬмЉ∞мЬЉлѓАл°Ь к≤∞м∞∞мЭА мЛЬмХЉмЧРмДЬ м†ХнЩХнХШк≤М нЩХмЭЄнХШмІА мХКк≥† мІДнЦЙнХілПД лђіл∞©нХШлЛ§. л≥інЖµ к∞АмЮ• мХИм™љ, мХДлЮШм™љ ліЙнХ©мВђлґАнД∞ к≤∞м∞∞мЭД мЛЬнЦЙнХШл©∞, мИШмИ†кЄ∞к≥Дл•Љ мЭімЪ©нХЬ к≤∞м∞∞л≥ілЛ§лКФ мЦСмЖРмЭД мЭімЪ©нХЬ к≤∞м∞∞(tie the knot)мЭі лє†л•ік≥† м†ХнЩХнХШк≤М мІДнЦЙнХ† мИШ мЮИлЛ§(Fig. 3 and Supplementary Video 1). мЭілХМлПД ліЙнХ©мВђмЭШ мИЬмДЬк∞А л∞ФлАМмІА мХКлПДл°Э м£ЉмЭШнХімХЉ нХШл©∞, мЛ§мЭі мЧЙнВ§лКФ к≤ГлПД м£ЉмЭШнХімХЉ нХЬлЛ§. мЭінЫД ліЙнХ©мЭі лґАм°±нХЬ лґАлґДмЭШ ліЙнХ©мЭД мґФк∞Ал°Ь мЛЬнЦЙнХШл©і нФЉнМР мВљмЮЕмЭД лБЭлВік≥† лѓЄмДЄнШИкіА мЬ†нХ©мИ†(microvascular anastomosis)л°Ь мІДнЦЙнХ† мИШ мЮИлЛ§.
к≤∞ к≥Љ
нМ®лЯђмКИнКЄ кЄ∞л≤ХмЭА мҐБк≥† кєКмЭА к≤∞мЖРмЧР нФЉнМРмЭД мВљмЮЕнХШлКФ лН∞ нЪ®к≥Љм†БмЭЄ мИШмИ†кЄ∞л≤ХмЭілЛ§. нКєнЮИ мµЬкЈЉ лСРк≤љлґАмЮђк±імЧР лІОмЭі мВђмЪ©лРШлКФ м†ДмЩЄлМАнЗінФЉнМР(anterolateral thigh free-flap) к∞ЩмЭі лґАнФЉк∞А нБ∞ нФЉнМРлПД нЪ®к≥Љм†БмЬЉл°Ь лє†л•Є мЛЬк∞Д мХИмЧР мВљмЮЕнХ† мИШ мЮИлЛ§. мИШмИ†мЛЬмХЉк∞А мґ©лґДнЮИ нЩХл≥ілРШмІА мХКмЭА к≤љмЪ∞мЧРлПД мХИм†ДнХШк≥† лє†л•ік≤М нФЉнМРмЭШ мВљмЮЕмЭД мІДнЦЙнХ† мИШ мЮИлКФ мИ†кЄ∞ м§С нХШлВШмЭілЛ§.