ņä£ļĪĀ
ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”Ø(obstructive sleep apnea, OSA)ņØĆ ļ░śļ│ĄņĀüņØĖ ņĢ╝Ļ░ä ĻĖ░ļÅä ĒÅÉņćäņÖĆ ļ╣łļ▓łĒĢ£ ņłśļ®┤ ņżæļŗ©ņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ņŗ¼Ēśł Ļ┤ĆĻ│ä ņ¦łĒÖś, ņéČņØś ņ¦ł ņĀĆĒĢś ļ░Å ņłśļ®┤ Ļ░Éņåī ļō▒ņØś ĒĢ®ļ│æņ”ØņØ┤ ļ░£ņāØĒĢśļŖö ĒØöĒĢ£ ņ¦łĒÖśņØ┤ļŗż [1,2]. ņ£Āļ│æļźĀņØĆ ļé©ņä▒ņØś ņĢĮ 22%, ņŚ¼ņä▒ņØś 17%ļĪ£ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż [3]. ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”ØņØś ņ╣śļŻīļŖö ņāØĒÖ£ņŖĄĻ┤ĆĻĄÉņĀĢ, ņ¦ĆņåŹņä▒ ĻĖ░ļÅäņ¢æņĢĢĒśĖĒØĪ(continuous positive airway pressure, CPAP), ĻĄ¼Ļ░Ģ ļé┤ ņןņ╣ś ļ░Å ņłśņłĀņĀü ņ╣śļŻī ļō▒ņØś ļ░®ļ▓ĢņØ┤ ņ׳ļŗż. CPAPļŖö ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”ØņØś ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻī ļ░®ļ▓ĢņØ┤ņ¦Ćļ¦ī, ņŚ░ĻĄ¼ņŚÉ ļö░ļØ╝ ņł£ņØæļÅäĻ░Ć 17%-54%ļĪ£ ļé«Ļ▓ī ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ņ£╝ļ®░, CPAP ņ╣śļŻīĻ░Ć ņŗżĒī©ĒĢ£ ĒÖśņ×ÉļōżņŚÉĻ▓īļŖö ļŗżļźĖ ņ╣śļŻī ļ░®ļ▓ĢņØ┤ ĒĢäņÜöĒĢśļŗż [4]. CPAP, ņĢĮļ¼╝ņ╣śļŻī, ņāØĒÖ£ņŖĄĻ┤ĆĻĄÉņĀĢ ļō▒ņØś ņ╣śļŻīĻ░Ć ļ¦īņĪ▒ĒĢĀļ¦īĒĢ£ Ļ▓░Ļ│╝ļź╝ ņ¢╗ņ¦Ć ļ¬╗ĒĢ£ ĒÖśņ×ÉļōżņØĆ ņłśņłĀņĀü ņ╣śļŻīĻ░Ć ļīĆņĢłņØ┤ ļÉĀ ņłś ņ׳ļŗż [5]. ĻĖ░ļÅä ĒÅÉņćä ļČĆņ£äņØś ĒśĢĒā£ņŚÉ ļö░ļźĖ ļŗżņ¢æĒĢ£ ņłśņłĀņĀü ņ╣śļŻīĻ░Ć Ļ│ĀņĢłļÉśņŚłņ£╝ļ®░ ņłĀĒøä ļČĆņ×æņÜ®ņØä ņżäņØ┤Ļ│Ā ņä▒Ļ│ĄļźĀņØä ļåÆņØ┤ļŖö ņŚ¼ļ¤¼ ņłśņłĀ ļ░®ļ▓ĢņØ┤ ņåīĻ░£ļÉśĻ│Ā ņ׳ļŗż [6]. Ļ│ĀņŗØņĀüņØĖ ļ░®ļ▓Ģņ£╝ļĪ£ ĻĄ¼Ļ░£ņłśĻĄ¼Ļ░£ņØĖļæÉ ņä▒ĒśĢņłĀ(uvulopalatopharyngoplasty, UPPP)ņØ┤ ļäÉļ”¼ ņŗ£Ē¢ēļÉśĻ│Ā ņ׳ņ£╝ļ®░, ņĄ£ĻĘ╝ ņÖĖņĖĪ ņØĖļæÉļ▓Į ĒÅÉņćäļź╝ ĻĄÉņĀĢĒĢśĻĖ░ ņ£äĒĢ┤ lateral-expansion pharyngoplasty, expansion sphincter pharyngoplasty ļō▒ņØś ļŗżņ¢æĒĢ£ ņłśņłĀņĀü ņ╣śļŻī ļ░®ļ▓ĢņØ┤ Ļ│ĀņĢłļÉśņŚłņ£╝ļéś, ĻĖ░ņłĀņĀüņ£╝ļĪ£ ņ¢┤ļĀĄĻ│Ā ņ╣©ņŖĄņĀüņØ┤ļ®░ ņŗ£Ļ░äņØ┤ ņśżļל Ļ▒Ėļ”░ļŗżļŖö ļŗ©ņĀÉņØ┤ ņ׳ļŗż [7-9]. ļ│Ė ļģ╝ļ¼ĖņŚÉņä£ļŖö ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”ØņØä ņ╣śļŻīĒĢśĻĖ░ ņ£äĒĢ£ ĻĄ¼Ļ░£ņłśĻĄ¼Ļ░£ņØĖļæÉņä▒ĒśĢņłĀ ņżæ ļ╣äĻĄÉņĀü ņēĮĻ▓ī ņŗ£Ē¢ē Ļ░ĆļŖźĒĢśĻ│Ā ņĄ£ņåī ņ╣©ņŖĄņĀü ļ░®ļ▓ĢņØĖ palatopharyngeal muscle suspension suture techniqueņØä ņåīĻ░£ĒĢśĻ│Āņ×É ĒĢ£ļŗż.
ļ░®ļ▓Ģ
ņłśņłĀ ņĀä ĒÅēĻ░Ć(Preoperative assessment)
ņłśņłĀ ņĀä ĒÅēĻ░Ć Ļ│╝ņĀĢņŚÉņä£ ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”ØņØä ĒÅēĻ░ĆĒĢśļŖö ņØ╝ļ░śņĀüņØĖ ĒĢŁļ¬®ļōżņŚÉ ļīĆĒĢ┤ņä£ ĒÅēĻ░Ćļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼(polysomnography, PSG), ņĢĮļ¼╝ņ£ĀļÅäņłśļ®┤ļé┤ņŗ£Ļ▓Į(drug-induced sleep endoscopy, DISE)ņØä ĒåĄĒĢśņŚ¼ ņłśļ®┤ņØś ņ¦łĻ│╝ ņłśļ®┤ ņŗ£ ĒÅÉņćäĻ░Ć ļ░£ņāØĒĢśļŖö ļČĆņ£äļź╝ ĒīīņĢģĒĢśņśĆļŗż. ĻĘĖ ņÖĖņŚÉļÅä ņ▓┤ņ¦łļ¤ēņ¦Ćņłś(body mass index), Brodsky ĒÄĖļÅä ļČäļźśļ▓Ģ, ļ│ĆĒśĢ Mallampati ņ▓ÖļÅäļź╝ ĒÖĢņØĖĒĢśņśĆļŗż. PSG Ļ▓Ćņé¼ Ļ▓░Ļ│╝ņŚÉņä£ļŖö ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņłśņ╣śņØĖ apnea-hypopnea index (AHI)ņÖĆ respiratory disturbance index (RDI), lowest oxygen saturation (LSAT)ņØä ĒÖĢņØĖĒĢśņŚ¼ ņłśņłĀ ĒÜ©Ļ│╝ļź╝ ļ╣äĻĄÉĒĢĀ ņłś ņ׳ļÅäļĪØ ĒĢśņśĆļŗż. DISEļź╝ ĒåĄĒĢ┤ņä£ļŖö ĒÖśņ×ÉņØś ņÖĖņĖĪ ņØĖļæÉļČĆ ĒÅÉņćäņØś ņ£Āļ¼┤ļź╝ ĒīÉļŗ©ĒĢśņśĆĻ│Ā, Ļ░Ćņן ņŻ╝ļÉ£ ĒÅÉņćä ļČĆņ£äĻ░Ć ņ¢┤ļööņØĖņ¦Ć ĒīīņĢģĒĢĀ ņłś ņ׳ļÅäļĪØ ņŗ£Ļ░üĒÖöĒĢśļŖö Ļ▓āņŚÉ ņżæņĀÉņØä ļæÉļ®░ ĒÅēĻ░Ćļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż [10].
ņłśņłĀ ņłĀĻĖ░(Operative procedures)
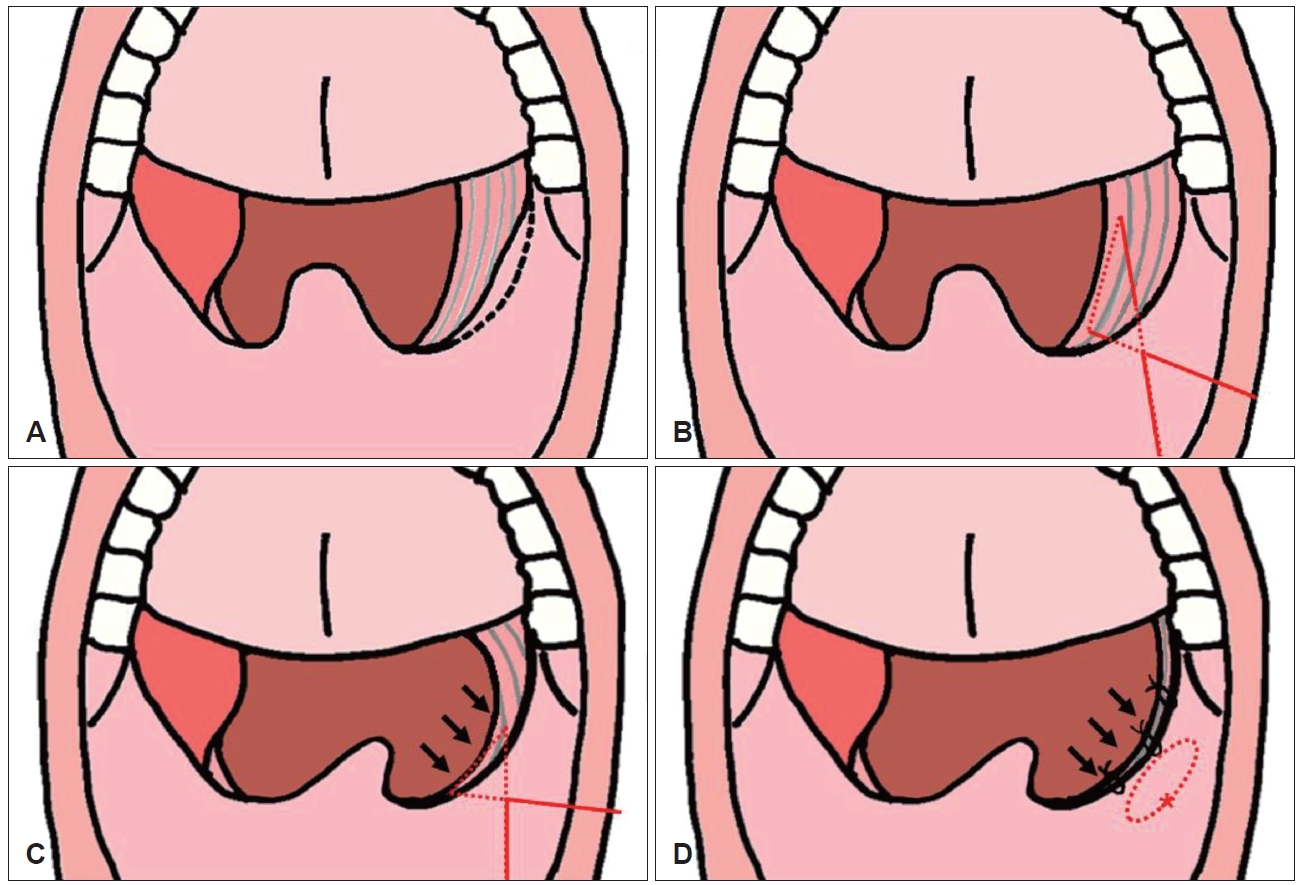
ņĢÖņÖĆņ£ä ņāüĒā£ņŚÉņä£ ņĀäņŗĀļ¦łņĘ©ņÖĆ ĻĖ░Ļ┤Ć ņéĮĻ┤ĆņØä ņŗ£Ē¢ēĒĢśĻ│Ā ĻĖ░Ļ┤Ć ļé┤ ĒŖ£ļĖīļź╝ ņżæņĢÖņ£╝ļĪ£ Ļ│ĀņĀĢĒĢśņśĆļŗż. ņØ┤Ēøä ĒÖśņ×ÉļŖö Rose ņ×ÉņäĖļź╝ ņĘ©ĒĢśĻ│Ā Crowe-Davis Ļ░£ĻĄ¼ĻĖ░(Medline, Northfield, IL, USA)ļź╝ ĻĄ¼Ļ░ĢņŚÉ ņ£äņ╣śĒĢśņŚ¼ ĻĄ¼ņØĖļæÉļź╝ ļģĖņČ£ņŗ£ņ╝░ļŗż. ĒÄĖļÅä Ļ▓Ėņ×ÉļĪ£ ĒÄĖļÅäļź╝ ļé┤ĒĢśņĖĪņ£╝ļĪ£ ņ×ĪņĢäļŗ╣ĻĖ░Ļ│Ā ĒÄĖļÅä ņāüĻĘ╣ņØä ņĀäĻĖ░ņåīņ×æĻĖ░ļĪ£ ņĀłĻ░£ĒĢ£ Ēøä ņĪ░ņŗ¼ņŖżļ¤ĮĻ▓ī ļ░Ģļ”¼ĒĢśņŚ¼ ĒÄĖļÅä Ēö╝ļ¦ēĻ│╝ ĒÄĖļÅäņÖĆ ņé¼ņØ┤ņØś ļ¼┤ĒśłĻ┤Ćņä▒ņØś ĒÄĖĒÅēĒĢ£ ļ®┤ņØä ļö░ļØ╝ ĒÄĖļÅäļź╝ ļ░Ģļ”¼ĒĢ£ Ēøä, ņ¢æņĖĪ ĒÄĖļÅäļź╝ ņĀłņĀ£ĒĢśĻ│Ā ļé£ ļÆż ļŗ©ĻĘ╣ ņĀäĻĖ░ņåīņ×æĻĖ░ļź╝ ņØ┤ņÜ®ĒĢśņŚ¼ ņĀäĻĄ¼Ļ░£ņäżĻČü(anterior pillar)ņØś ļé©ņØĆ ļČĆļČäņØś ņØ╝ļČĆļź╝ ņ£äņ¬Į ļČĆņ£ä Ļ▓ĮĻ│äļ®┤ņØä ļö░ļØ╝ ņĀłņĀ£ĒĢśņśĆļŗż(Fig. 1A). Monosyn 3-0 (B. Braun, Melsungen, Germany)ņØä ĻĄ¼ņ╣śĒøäņé╝Ļ░ü(retromolar trigone) ļČĆņ£äņŚÉņä£ ņĀÉļ¦ēĒĢśļĪ£ ĒåĄĻ│╝ņŗ£ņ╝£ ĒÄĖļÅäņÖĆņØś ņāüņĖĪņ£╝ļĪ£ ļéśņś¼ ņłś ņ׳ļÅäļĪØ ĒĢśņśĆļŗż. ņØ┤Ēøä ĒÄĖļÅäņÖĆ ļ░öļŗźņØś ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝(palatopharyngeus muscle)ņØä ņłśņ¦ü ļ░®Ē¢źņ£╝ļĪ£ Ļ░ĆļŖźĒĢ£ ļäōĻ▓ī ņĢĮ 2 cm ņĀĢļÅä Ļ▒ĖĻ│Ā ļéśņä£ ņĀÉļ¦ēĒĢśļź╝ ĒåĄĒĢśņŚ¼ ņ▓śņØī ļōżņ¢┤Ļ░öļŹś ĻĄ¼ņ╣śĒøäņé╝Ļ░üņ£╝ļĪ£ ļéśņś¼ ņłś ņ׳ļÅäļĪØ ĒĢśņśĆļŗż(Fig. 1B). ņĀüļŗ╣ĒĢ£ ĻĖ┤ņןņØä ņ£Āņ¦ĆĒĢ£ ņ▒äļĪ£ Ļ▓░ņ░░ņØä ņŗ£Ē¢ēĒĢśņśĆĻ│Ā, ĻĄ¼Ļ░£ļČĆ ņĪ░ņ¦üņØ┤ ņĀäņÖĖņāüļ░®ņ£╝ļĪ£ ļŗ╣Ļ▓©ņ¦ĆļŖö Ļ▓āņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż(Fig. 1C). ļ¦łņ¦Ćļ¦ēņ£╝ļĪ£ Vicryl 4-0 (Ethicon Inc., Raritan, NJ, USA)ņØä ņé¼ņÜ®ĒĢśņŚ¼ ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝Ļ│╝ ĻĄ¼Ļ░£ņäżĻĘ╝(palatoglossus muscle)ņØä 3-4ĒÜī ņĀĢļÅä ļ┤ēĒĢ®ĒĢśņŚ¼ ĻĄ¼Ļ░£ĒøäļČĆņØś ĻĖ░ļÅä ĒÖĢņןņØä ņ£äĒĢ£ ņĀüļŗ╣ĒĢ£ ĻĖ┤ņןņØä ņ£Āņ¦ĆĒĢĀ ņłś ņ׳ļÅäļĪØ ĒĢśņśĆļŗż(Fig. 1D) (Supplementary Video 1).
ņłśņłĀ Ēøä Ļ┤Ćļ”¼(Postoperative care)
ņłśņłĀ Ēøä Ļ┤Ćļ”¼ļŖö Ļ│ĀņŗØņĀüņØĖ ĻĄ¼Ļ░£ņłśĻĄ¼Ļ░£ņØĖļæÉņä▒ĒśĢņłĀņØä ņŗ£Ē¢ēĒĢ£ ĒÖśņ×ÉņÖĆ ļŗżļź┤ņ¦Ć ņĢŖĻ▓ī ņØ╝ļ░śņĀüņØĖ ņłśņłĀ Ēøä ļéśĒāĆļéĀ ņłś ņ׳ļŖö ĒåĄņ”Ø ļ░Å ĻĄ¼ņŚŁĻ░É, ļ│Ćļ╣ä ļō▒ņØś ņ”ØņāüņŚÉ ļīĆĒĢ£ ņ”Øņāü ņĪ░ņĀłņØä ņŗ£Ē¢ēĒĢśņśĆļŗż. ļśÉĒĢ£ ņłśņłĀ ĒøäņŚÉ ļ░£ņāØ Ļ░ĆļŖźĒĢ£ ņłśņłĀ ļČĆņ£ä ļČĆņóģņŚÉ ļīĆĒĢ£ ĒÅēĻ░Ć ļ░Å ņłśņłĀ ļČĆņ£ä ņČ£Ēśł ņ£Āļ¼┤ļź╝ ĒīÉļŗ©ĒĢśĻĖ░ ņ£äĒĢ┤ņä£ ņŻ╝ĻĖ░ņĀüņ£╝ļĪ£ ĒøäļæÉļé┤ņŗ£Ļ▓ĮņØä ņ┤¼ņśüĒĢśņśĆļŗż. ĒÖśņ×ÉļŖö ņłśņłĀ Ēøä 3ņØ╝Ļ░ä ņ×ģņøÉ ņ╣śļŻīļź╝ ļ░øņØĆļÆż ņØ╝ņāü ņāØĒÖ£ņØ┤ Ļ░ĆļŖźĒĢśļŗżĻ│Ā ĒīÉļŗ©ļÉśņ¢┤ Ēć┤ņøÉĒĢśņśĆļŗż. Palatopharyngeal muscle suspension sutureņŚÉ ņé¼ņÜ®ĒĢśņśĆļŹś monosynņØĆ mucosa ļé┤ļČĆļĪ£ ļ¦żļ¬░ļÉśņ¢┤ ņ£ĪņĢłņĀüņ£╝ļĪ£ Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśĻ│Ā, ņ¦ĆņåŹņĀüņØĖ ĻĖ┤ņן ņ£Āņ¦Ćļź╝ ņ£äĒĢśņŚ¼ ļ┤ēĒĢ®ņØä ļ░£ņé¼ĒĢśņ¦Ć ņĢŖņĢśļŗż. ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝Ļ│╝ ĻĄ¼Ļ░£ņäżĻĘ╝ņØä ļ┤ēĒĢ®ĒĢ£ Vicryl 4-0ļÅä ĒØĪņłśņä▒ ļ┤ēĒĢ®ņé¼ļĪ£ ņ×ÉņŚ░ņŖżļ¤ĮĻ▓ī ļģ╣ņØä ņłś ņ׳ļÅäļĪØ ļæÉņŚłļŗż.
ņłśņłĀ Ēøä Ļ▓░Ļ│╝(Postoperative result)
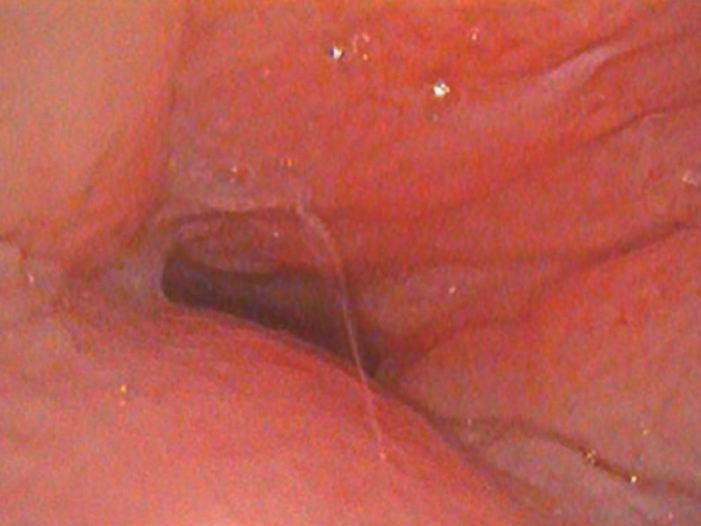
ņłśņłĀ ņĀä ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼ Ļ▓░Ļ│╝ AHIļŖö 57.5ĒÜī/hr, RDIļŖö 58.8ĒÜī/hr, LSATļŖö 79%ļĪ£ ĒÖĢņØĖļÉśņŚłļŗż(Table 1). ņłśņłĀ ņĀä ņĢĮļ¼╝ņ£ĀļÅä ņłśļ®┤ļé┤ņŗ£Ļ▓ĮņāüņŚÉņä£ļŖö ĻĄ¼Ļ░£ņłś ļ░Å ņÖĖņĖĪ ņØĖļæÉļ▓ĮņØś ĻĄ¼ņŗ¼ņä▒ ĒśĢĒā£ņØś ņÖäņĀäĒĢ£ ĒÅÉņćäĻ░Ć ĒÖĢņØĖļÉśņŚłņ£╝ļ®░, Ļ▓Ćņé¼ ņŗ£Ē¢ē ņżæ ņĮöĻ│©ņØ┤ ļ░Å ļ¼┤ĒśĖĒØĪņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż(Fig. 2). ņłśņłĀ ņĀä ĻĄ¼Ļ░Ģ ļé┤ ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņāü ņ¢æņĖĪ ĒÄĖļÅäņØś ļ╣äļīĆ, ņäżĻĘ╝ļČĆ ļ╣äļīĆņÖĆ ĒĢ©Ļ╗ś ņāüļīĆņĀüņ£╝ļĪ£ ĻĖĖĻ│Ā ļæÉĻ║╝ņÜ┤ ĻĄ¼Ļ░£ņłśļĪ£ ņØĖĒĢ£ ĻĖ░ļÅäņØś Ēśæņ░®ņØ┤ Ļ┤Ćņ░░ļÉśņŚłļŗż(Fig. 3). ĒÖśņ×ÉļŖö ņłśņłĀ ņĀä ņŻ╝Ļ┤ĆņĀüņØĖ ņ”Øņāüņ£╝ļĪ£ ņĮöļ¦ēĒל ļ░Å ņĮöĻ│©ņØ┤, ņŻ╝Ļ░ä ņĪĖļ”╝ņ”Ø, Ļ░£ņÜ┤ĒĢśņ¦Ć ļ¬╗ĒĢ£ ņłśļ®┤ ļ░Å ļČłļ®┤, Ēö╝ļĪ£Ļ░É ļō▒ņØä ĒśĖņåīĒĢśņśĆļŗż. ņłśņłĀ Ēøä 3Ļ░£ņøö ļÆżņŚÉ ņłśļ®┤ļŗżņøÉĻ▓Ćņé¼, ņĢĮļ¼╝ņ£ĀļÅä ņłśļ®┤ļé┤ņŗ£Ļ▓Į ņŗ£Ē¢ē ļ░Å ņ”Øņāü ĒśĖņĀä ņ£Āļ¼┤ņŚÉ ļīĆĒĢ£ ĒÅēĻ░Ćļź╝ ņŗ£Ē¢ēĒĢśņśĆļŗż. ņłśņłĀ Ēøä ņłśļ®┤ ļŗżņøÉĻ▓Ćņé¼ Ļ▓░Ļ│╝ AHI 23.9ĒÜī/hr, RDI 26ĒÜī/hr, LSAT 88%ļĪ£ ļīĆļČĆļČäņØś ņ¦ĆĒæ£Ļ░Ć Ļ░£ņäĀļÉ£ ņłśņ╣śļź╝ ļ│┤ņśĆļŗż(Table 1). ņłĀĒøä ņĢĮļ¼╝ ņ£ĀļÅäņłśļ®┤ ļé┤ņŗ£Ļ▓Įņāü ņłĀņĀä Ļ▓Ćņé¼ņÖĆ ļ╣äĻĄÉĒĢ┤ ĻĄ¼Ļ░£ņłśņØś ĒÅÉņćäļŖö ĒÖĢņØĖļÉśņ¦Ć ņĢŖņĢśņ£╝ļ®░ ņÖĖņĖĪ ņØĖļæÉļ▓ĮņØś ļ»ĖņĢĮĒĢ£ ĻĄ¼ņŗ¼ņä▒ ĒśĢĒā£ņØś ĒÅÉņćäĻ░Ć ņ׳ņŚłļŗż(Fig. 4). ņŻ╝Ļ░ä ņĪĖļ”╝ņ”Ø, Ēö╝ļĪ£Ļ░É ļō▒ ņłśņłĀ ņĀä ļŖÉļü╝ļŹś ņŻ╝Ļ┤ĆņĀü ņ”Øņāü ļ¬©ļæÉ ĒśĖņĀäļÉśņŚłļŗż. ņłśņłĀ Ēøä ĻĄ¼Ļ░Ģ ļé┤ ļé┤ņŗ£Ļ▓Į ņåīĻ▓¼ņāü ņłśņłĀ ņĀäņŚÉ ļ╣äĒĢ┤ ļ╣äņØĖļæÉĻ░ĢņØ┤ ļ¦ÄņØ┤ ļäōņ¢┤ņ¦ä Ļ▓āņØä ņĢī ņłś ņ׳ņŚłļŗż(Fig. 5). ņłĀĒøä 6Ļ░£ņøöņ¦Ė ļ╣äņØĖļæÉĻ░Ģ ņØ┤ļ¼╝Ļ░É ļō▒ņØś ĒĢ®ļ│æņ”Ø ņŚåņØ┤ Ļ┤Ćņ░░ ņżæņØ┤ļŗż.
Ļ▓░Ļ│╝
Lateral-expension pharyngoplastyļŖö ņāüņØĖļæÉņłśņČĢĻĘ╝(superior pharyngeal constrictor muscle)ņØś ņĀłņĀ£ ļ░Å ĒÜīņĀäņØä ĒżĒĢ©ĒĢśņŚ¼ ĻĄ¼Ļ░£Ēö╝ĒīÉņØä Z-ņä▒ĒśĢņ£╝ļĪ£ ļäōĒśĆņŻ╝ļŖö ņłĀņŗØņ£╝ļĪ£ ņĀĢņāü ĒĢ┤ļČĆĒĢÖņĀü ĻĘ╝ņ£Ī ĻĄ¼ņĪ░ļ¼╝ņŚÉ ņāüļŗ╣ĒĢ£ ļ│ĆĒśĢņØä Ļ░ĆĒĢśļŖö ņłĀņŗØņØ┤ļŗż. ņłśļ®┤ ļŗżņøÉĻ▓Ćņé¼ Ļ▓░Ļ│╝ļŖö Ļ│ĀņŗØņĀüņØĖ UPPPļ│┤ļŗż ĒÜ©Ļ│╝ņĀüņØ┤ļéś ņŚ░ĒĢśĻ│żļ×Ć, ĻĄ¼Ļ░£ņØĖļæÉĻĖ░ļŖźļČĆņĀä(velopharyngeal insufficiency), ņāüņ▓ś ļ▓īņ¢┤ņ¦É ļō▒ņØś ļČĆņ×æņÜ®ņØ┤ ņĪ░ĻĖł ļŹö ļ░£ņāØĒĢśļŖö Ļ▓āņ£╝ļĪ£ ļ│┤Ļ│ĀļÉśņŚłļŗż [9]. Expansion sphincter pharyngoplastyļŖö ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝ņØś ĒĢśļČĆņØś ņØ╝ļČĆļČäņØä ņĀłņĀ£ĒĢśņŚ¼ ĻĘ╝ņ£ĪņØä ņØ┤ļÅÖņŗ£ņ╝£ ņĀäļ░®, ņāüņÖĖņĖĪņ£╝ļĪ£ ļÅīļ”¼ļŖö ņłĀņŗØņØ┤ļŗż [10].
Single suspension sutureļŖö ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝ņØś Ļ░Ćņן ņāüļČĆ ļČĆņ£äņŚÉņä£ ļ┤ēĒĢ®ņØä ņŗ£ņ×æĒĢśņŚ¼ ņØĄļÅīĻĄ¼(pterygoid hamulus) ĻĘ╝ņ▓śņŚÉņä£ ĻĄ¼Ļ░£ņäżĻĘ╝ņØä ĒåĄĻ│╝ĒĢśļ®┤ņä£ ĒÄĖļÅäņÖĆņŚÉņä£ ļ┤ēĒĢ®ņØä ĒĢśņŚ¼ ĻĖ┤ņןņØä ĒśĢņä▒ĒĢśļŖö ņłĀņŗØņØ┤ļŗż [11]. ļ¦łņ░¼Ļ░Ćņ¦ĆļĪ£ pterygomandibular suspension sutureļŖö ņØĄļÅīĻĄ¼ ļåÆņØ┤ņŚÉņä£ ņØĄļÅīĒĢśņĢģļČĆ(pterygomandibular) Ļ░ĆņĖĪņŚÉņä£ ņŗ£ņ×æĒĢśņŚ¼ ĒøäĻĄ¼Ļ░£ņäżĻČü(posterior pillar)ļź╝ ĒåĄĻ│╝ĒĢ┤ņä£ ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝Ļ│╝ ĒøäĻĄ¼Ļ░£ņäżĻČü Ēö╝ĒīÉņØä Ļ▒ĖĻ│Ā ņØĄļÅīĻĄ¼ ļé┤ņĖĪņ£╝ļĪ£ ļÅīņĢäņÖĆņä£ ĻĖ┤ņןņØä ĒśĢņä▒ĒĢśļŖö ņłĀņŗØņØ┤ļŗż [12].
ņØ┤ļ¤¼ĒĢ£ ņĀÉņŚÉņä£ palatopharyngeal suspension sutureļŖö expension phayrngoplastyņÖĆļŖö ļŗżļź┤Ļ▓ī ņØĖļæÉĻĘ╝ņ£ĪņØä ņĀłņĀ£ĒĢśĻ▒░ļéś ĒÜīņĀäĒĢśņŚ¼ ņØĖļæÉļČĆļź╝ ĒÖĢņןĒĢśļŖö Ļ▓āņØ┤ ņĢäļŗłļØ╝ ļ╣äĻĄÉņĀü ļŹ£ ņ╣©ņŖĄņĀüņØĖ ļ░®ļ▓ĢņØĖ ļ┤ēĒĢ®ņé¼ļź╝ ĒåĄĒĢ┤ ĻĖ┤ņןņØä Ļ░ĆĒĢ£ļŗż. ļö░ļØ╝ņä£ ņĀĢņāü ĒĢ┤ļČĆĒĢÖņĀü ĻĄ¼ņĪ░ļź╝ ņ£Āņ¦ĆĒĢĀ ņłś ņ׳ņ£╝ļ®░, ļČĆņ×æņÜ®ņØś Ļ░ĆļŖźņä▒ļÅä ļé«ņØä Ļ▓āņ£╝ļĪ£ ĒīÉļŗ©ļÉ£ļŗż.
ĒāĆ ļģ╝ļ¼ĖņŚÉņä£ ņåīĻ░£ĒĢśļŖö suspension suture ņłĀņŗØļōżĻ│╝ ļ│Ė ļģ╝ļ¼ĖņØś palatopharyngeal suspension sutureņÖĆ ņ£Āņé¼ĒĢ£ ņĀÉņØ┤ ņ׳ņ¦Ćļ¦ī, ĒāĆ suspension sutureļŖö ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝ņŚÉ ĻĖ┤ņןļÅäļź╝ Ļ░ĆĒĢśļŖö ņ¦ĆņĀÉņØ┤ ĒĢśļéśņØś ņĀÉņØ┤ļØ╝ļŖö Ļ▓āņØä Ļ░Ćņן Ēü░ ņ░©ņØ┤ņĀÉņ£╝ļĪ£ ļ│╝ ņłś ņ׳ļŗż. Single suspension sutureļŖö ņØ┤ņÖĆ Ļ░ÖņØĆ ļŗ©ņĀÉņØä ĻĘ╣ļ│ĄĒĢśĻĖ░ ņ£äĒĢ┤ņä£ double suspension sutureļź╝ ņŗ£Ē¢ēĒĢśņŚ¼ ņ▓śņØī ņŗ£Ē¢ēĒĢ£ ļ┤ēĒĢ® ļČĆņ£äļ│┤ļŗż ņÖĖņĖĪĒĢśļ░® ļČĆņ£äļĪ£ ņ£Āņé¼ĒĢ£ ļ░®ņŗØņ£╝ļĪ£ ĒĢ£ ļ▓ł ļŹö ļ┤ēĒĢ®ņØä ņŗ£Ē¢ēĒĢ£ļŗż [13]. Palatopharyngeal suspension sutureļŖö ĒĢ£ ļ▓łņØś ļ┤ēĒĢ®ņ£╝ļĪ£ ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝ņØś ņāüļČĆļČĆĒä░ ĒĢśļČĆĻ╣īņ¦Ć ĒĢśļéśņØś ņĀÉņØ┤ ņĢäļŗī ņĀäļ░śņĀüņØĖ ĻĘ╝ņ£Īļ®┤(plane)ņ£╝ļĪ£ ĻĖ┤ņןļÅäļź╝ ņŻ╝ļ®┤ņä£ Ļ▓¼ņØĖĒĢĀ ņłś ņ׳ļŗżļŖö ņןņĀÉņØ┤ ņ׳ļŗż(Fig. 1C). ņØ┤ļ¤░ ņĀÉņŚÉņä£ ĒāĆ suspension sutureļ│┤ļŗż palatopharyngeal suspension sutureļŖö ĻĄ¼Ļ░£ņØĖļæÉĻĘ╝ņŚÉ ĻĖ┤ņןļÅäļź╝ ļŹö ļäōĻ▓ī ņżä ņłś ņ׳ņ£╝ļ®░, ņłĀĻĖ░ņØś ņŗ£Ļ░äļÅä ļŗ©ņČĢĒĢĀ ņłś ņ׳ļŗż.
Ļ▓░ļĪĀņĀüņ£╝ļĪ£ ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ ņåīĻ░£ĒĢ£ palatopharyngeal muscle suspension suture techniqueņØĆ ļŗżļźĖ ņłĀĻĖ░ņŚÉ ļ╣äĒĢ┤ ņĄ£ņåī ņ╣©ņŖĄņĀüņØ┤ļ®░, ņłĀĻĖ░Ļ░Ć ņ¢┤ļĀĄņ¦Ć ņĢŖņĢä ņ┤łņŗ¼ņ×ÉļÅä ņēĮĻ│Ā ļ╣Āļź┤Ļ▓ī ņŗ£Ē¢ēĒĢĀ ņłś ņ׳Ļ│Ā, ļśÉĒĢ£ Ļ░ĆņŚŁņĀüņØ┤ļØ╝ļŖö ņןņĀÉņØ┤ ņ׳ļŗż. ņØ┤ņŚÉ ņĀĆņ×ÉļōżņØĆ ņØ┤ ņłĀĻĖ░Ļ░Ć ĒÅÉņćäņä▒ ņłśļ®┤ļ¼┤ĒśĖĒØĪņ”ØņØś ņłĀĒøä ņä▒Ļ│ĄļźĀņØä ļåÆņØ╝ ņłś ņ׳ļŖö ņČöĻ░ĆņĀüņØĖ ņłĀņŗØ ņżæņØś ĒĢśļéśĻ░Ć ļÉĀ Ļ▓āņØ┤ļØ╝Ļ│Ā ņĀ£ņĢłĒĢśļŖö ļ░öņØ┤ļŗż.