상악동에서 발생한 암육종 1예
Abstract
Carcinosarcoma is a highly malignant tumor characterized by dual malignant histologic differentiation of epithelial and mesenchymal components, which rarely occurs in the maxillary sinus. We experienced a case of carcinosarcoma mixed with a keratinizing squamous cell carcinoma and an osteosarcoma arising from the right maxillary sinus recently. A 55-year-old male patient presented with right nasal obstruction and epistaxis. The initial punch biopsy revealed a high-grade sarcoma, favoring an osteosarcoma. After general evaluation, the patient was staged as cT4aN0M0. The patient was treated by right total maxillectomy, radiotherapy, and chemotherapy. We present with a review of the literature a case of a carcinosarcoma originating from the right maxillary sinus that had invaded into the orbital cavity and protruded into the nasal cavity.
Key words: Carcinosarcoma ㆍ Maxillary sinus ㆍ Total maxillectomy
서 론
암육종(carcinosarcoma)은 상피세포 기원암과 중배엽 ].원암이 섞여 있는 형태의 암종으로 매우 드물게 발견되며 공격적인 진행을 보인다. 따라서 예후가 불량하며 재발을 억제하기 위해서는 광범위한 절제술을 포함한 적극적인 치료가 요구된다[1,2)
암육종은 편평상피로 덮혀있는 신체의 다양한 장기에서 발생할 수 있으며, 폐, 자궁, 난소, 위장관 그리고 피부에서 발생된다고 보고되고 있다[ 3- 8]. 두경부에서 가장 발생률이 높은 부위는 타액선이며, 국소 재발이 높은 경향을 보이며 일반적으로 발생된 후 30개월 내에 폐 혹은 뇌로 전이가 발생한다[ 8]. 문헌상 보고 예에서 알 수 있듯이 비강 혹은 부비강 내에서는 발생빈도가 특히 적다. 이와 같이 상악동에서 발생한 암육종은 주위조직의 침범률이 매우 높아 예후가 불량한데도 불구하고 발현빈도가 매우 드물어 초기 발견, 진단, 특히 치료방법에 대해서 가이드 라인이 확립되어 있지 않다[ 9, 10]. 저자들은 우측 상악동에 발생한 종양을 수술전 조직검사에서는 골육종으로 진단되었으나 수술 후 조직검사로 골육종과 상피세포암이 섞인 형태의 암육종으로 확인된 예를 경험하였기에 문헌 고찰과 함께 보고하고자 한다.
증 례
55세 남자 환자가 1주 전부터 시작된 우측 비폐색, 비출혈로 내원하였다. 우측 수양성 비루, 상악동부위의 통증이 동반되었고, 신체검진상에서 우측 상악 부위 압통 외에 만져지는 경부 종물은 없었고 기타 다른 내과적 질환이나 코수술의 병력은 없었다.
전비경 및 비내시경 검사에서 우측 비강을 완전 폐쇄시키고 있는 검붉은 색의 종괴가 코 안뜰까지 노출되어 있었다( Fig. 1A). 조직검사를 위해 펀치 생검술로 종괴를 일부 제거한 후에 다시 비내시경을 확인하였을 때 중비갑개의 하측, 하비갑개의 내측을 채우고 있는 단단하고 불규칙한 모양의 종괴가 확인되었다. 조직검사상 high grade sarcoma, favor osteosarcoma 소견을 보였다. 부비동 전산화단층촬영검사에서 우측 상악동의 앞벽과 내측벽, 사골동의 하벽, 안와저의 골파괴를 보이는 비균질의 조영증강되는 고형의 괴사성 종괴가 확인되었다( Fig. 1B and C). 종괴는 상악동 바깥으로 확장하여 하측두와, 안와저, 상악동 앞쪽 연조직까지 침범하고 있었으나 두개 내 침범은 보이지 않았다. 또한 종괴에 의해 이차적으로 발생한 부비동염이 우측 전두동, 사골동의 앞쪽에 관찰되었다( Fig. 1B and C). 경부 전산화단층촬영에서는 악성 림프절 전이로 의심되는 병변은 없었다. 자기공명영상검사에서는 우측 상악동, 사골동, 전두동, 비강내에 비강 내 출혈을 동반한 조영증강되는 종괴가 우측 저작근 공간, 협부 공간까지 확장되어 익돌근, 익구개와, 접구개공, 상악골을 침범하는 소견을 보였다( Fig. 1D and E). 경부초음파에서 양측 level 1, 2 , 3에 경계성 림프절들이 보여 우측 level IB에서 세침흡인검사를 시행하였고 단순한 임파선염으로 확인되었다.
양전자방출단층촬영에서 C T, M RI에서 언급되었던 우측 상악동의 악성종양으로 의심되는 대량의 fluorodeoxyglucose 섭취 증가가 확인되었고 경부 림프절 전이나 원격전이 소견은 보이지 않았다( Fig. 2A and B). 최종 임상병기는 경부 림프절이나 다른 부위 전이가 없는 cT4aN0M0로 확인되었다. 수술은 우측 전상악절제술을 계획하였고 안검하부에 횡절개를 포함한 Weber-Fergusson 절개로 노출시켰다. 치은 협부 절개를 동측의 상악결절까지 연장시킨 후 상부 협부 피판을 치은협부열, 치은순열을 통해 거상하였다. 하안검 피판은 안륜근보다 표면적으로, 외안각보다 1 cm 외측으로 들어올렸다. 안와의 골막하 박리를 시행하였고 우측 코 전정의 외측 절개를 통해 이상구로 비강을 확인하였다. Gigli saw를 이용하여 협골주, 구개를 절제하였고 절골도를 이용하여 비상악 절골을 시행하였다. 이어 날개판 골절술을 하고 연이어 상악골전적출을 하였다( Fig. 2C). 제거하자마자 출혈을 일으킨 내 상악골 동맥을 결찰하였다. 성형외과에서 상악동의 후외측면에 대해 좌측 허벅지로부터 부분층피부이식을 얻어 봉합하고 우측 상악동, 양측 비강내 패킹을 시행하였다. 수술장에서 상악동 전벽, 안와하벽, 사골동, 익구개와 침범이 보였다. 종양의 침범부위를 제거할 때 경계부위를 확인하기 위하여 동결 절편조직 검사는 시행하지 않았으나, 최대한으로 종양의 침범 부위를 제거하려고 하였다. 안와하벽은 암종에 의하여 파괴 되었으나 안와 골막은 암종에 의하여 안구가 상방편위된 상태로 수술 시 관찰되어 안구를 보존하기 위하여 암종과 접촉되어 있던 골막과 안와 하벽을 제거하였다. 임상경험상 안와 골막을 제거하여 안구주위의 지방조직이 노출될 정도로 제거하여도 예후에는 관련이 없었기 때문에 가능한 한 전상악 절제술 시 안구를 제거하지 않고 접촉된 안와골막의 일부는 제거하고 있다. 익구개와 방향으로는 전적출 시에 근육층막까지 제거하여 근육층이 관찰될 때까지 제거하였다. 사골동 방향으로는 정상 사골동점막을 포함하여 사골동의 천정부위의 골이 노출될 때까지 최대한으로 제거하였다. 상악동전벽에서는 골침식을 포함하여 종양으로 침범된 연조직은 정상조직을 포함하여 안전연을 확보하여 제거하였다. 이와 같이 전상악적출 후 육안적으로 종양이 남아있지 않다고 판단하였기 때문에 전적출술 후 연조직의 상처치유가 잘 회복되도록 피부이식을 행하였다. 병리결과에서 암육종, 즉 골육종과 각화성 편평세포암이 공존해 있는 소견을 보였으며, 면역염색에서도 2가지 형태가 섞여있는 암육종 소견을 보였다( Fig. 3). 수술 이후로 피부이식 부위가 안정적으로 유지되었고 수술후 10일째 obturator 제작되어 착용하였다. 술후 항암요법(adriamycin+ cisplatin)과 방사선 치료 병합요법을 하고 현재 추적 관찰하고 있다. 현재 술후 10개월이 지난 상태로 추적 관찰 중이며, 최근 촬영한 컴퓨터단층촬영에서 협골의 절제연에 국소재발된 암종의 음영이 관찰되어 추가로 시행한 항암요법에도 암종의 진행이 억제되지 않아 수술로 제거하였다 ( Fig. 4).
고 찰
암육종은 조직학적으로 상피세포와 중배엽 성분이 혼재되어 발생되고 있다. 중배엽성분은 육종양 기질(sarcomatoid stroma)로부터 구성되는데, 연골 육종(chondrosarcoma), 골육종(osteosarcoma)이 발생되기도 하며[ 8], 그러나 섬유육종(fibrosarcoma), 평활근 육종(leiomyosarcoma), 혹은 지방 육종(liposarcoma)이 발현될 수 있다[ 11, 12]. 이러한 이유로 본 예에서도 수술 전 조직검사에서는 골육종이나 분화도가 낮은 상피암으로 진단되었으나 상악동 전적출술 후에 시행한 조직검사에서는 골육종으로 확인되었다. 골육종의 특성상 pseudosarcoma, pseudosarcomatous squamous cell carcinoma, pleomorphic carcinoma, spindle cell carcinoma로 불리워지기도 한다. 일반적으로 상악동에서 발생한 암육종의 발생 빈도는 매우 적어 치료방법, 발생원인, 그리고 치료 후 예후 등에 대해서 논란이 많다. 암육종의 발생에 대한 2가지 가설이 제시되고 있는데, 수렴이론(convergence hypothesis)과 분화이론(divergence hypothesis)이 있다. 수렴이론은 2개의 줄기세포주에서 이질성 종양이 발생한다는 이론이고, 분화이론은 한 개의 줄기세포에서 상피세포와 중배엽성분으로 분화한다는 이론이다[ 2]. Lichtiger 등[ 13]은 방추세포에서 상피세포분화가 발현되면서 육종성분으로 분화한다는 것을 보고했는데 이러한 연구는 육종발생의 분화이론을 옹호하고 있다. 우리의 증례를 포함하여 최근부터 후향적으로 발표된 15예를 분석한 결과, 상악동에서 발생한 육종 환자의 평균연령은 57.7세였고, 9명은 남성 환자이고 여성 환자는 6명이었다. 발견될 당시의 병기는 대부분이 T3N0M0 이상이었다. 보고된 예의 병리학적 소견을 분석하여 보면 대부분에서 방추세포 성분과 상피세포 성분이 발현되어 있었다. 보고된 예에서 본 예에서 관찰된 골육종소견에 대해서는 기술되어 있지 않았다( Supplementary Table 1). 이 중 11예(73%)에서 수술요법이 시행되었고, 13예(86%)에서 방사선 치료가 시행되었다. 4예(26%)에서 수술요법과 방사선 치료가 병행되었고, 2예(13%)에서 수술요법과 항암요법이 병행되었다. 6예(40%)에서 수술요법과 방사선 치료 그리고 항암요법이 병행되었다. 2예(13%)에서는 방사선 요법이 시행되었고 1예(6%)에서만 수술없이 방사선요법과 항암요법이 시행되었다( Supplementary Table 1). 상악동에서 발생한 암육종은 발생빈도가 매우 적어 일반적으로 합의된 치료 가이드라인은 없는 상황이다. 그러나 두경부 영역에서 발생한 암육종은 수술요법이 가장 일반적으로 행하여지는 치료양상이다. 그럼에도 불구하고 상악동에서 발생한 예가 매우 적고 생존률이 매우 낮아 상악동의 암육종에서 대해서 적절한 치료방침을 정하는 것은 현재로서는 가능하지 않다고 판단된다. 그러하지만 이 종양의 특징적인 공격적인 침윤성 때문에 가능하면 매우 적극적인 수술요법과 항암요법 그리고 방사선 요법의 병용요법이 필요하다고 판단된다. 현재까지 본예에서는 상악동 전적출술과 방사선 요법 그리고 항암요법으로 진행이 억제되고 있다.
저자들은 일측성 비폐쇄로 내원한 환자에서 영상의학적 검사, 수술적 치료 및 조직검사를 통해 상악동에서 발생한 암육종을 1예를 치험하였기에 문헌 고찰과 함께 보고하는 바이다.
Notes
Author Contribution
Conceptualization: Tae Hoon Lee, Sang Hag Lee. Data curation: Tae Hoon Lee, Sang Hag Lee. Formal analysis: Tae Hoon Lee, Sang Hag Lee. Investigation: Tae Hoon Lee, Sang Hag Lee. Methodology: Da Bin Lee, Seung Hyeok Lee. Project administration: Da Bin Lee, Seung Hyeok Lee. Resources: Da Bin Lee, Seung Hyeok Lee. Supervision: Sang Hag Lee. Validation: Sang Hag Lee. Visualization: all authors. Writing—original draft: Tae Hoon Lee, Sang Hag Lee. Writing—review & editing: Tae Hoon Lee, Sang Hag Lee.
Fig. 1.
The profiles of carcinosarcoma involving the right sinonasal cavity which were evaluated with endoscopy, PNS CT, and MRI. A: Endoscopic view shows reddish mass protruded through anterior naris. B: Coronal view of PNS CT demonstrates the mass in the right maxillary sinus, invading the orbital cavity and destructing the medial wall of the maxillary sinus. C: Axial view of PNS CT reveals that maxillary sinus mass invades the infratemporal fossa, protruding into the nasal cavity. D: Axial T2-weighted PNS MRIs show the maxillary sinus mass involving the infratemporal fossa and nasal cavity. E: Coronal T2-weighted PNS MRIs show the maxillary sinus mass involving the infratemporal fossa, orbital cavity, and nasal cavity. PNS, paranasal sinus. 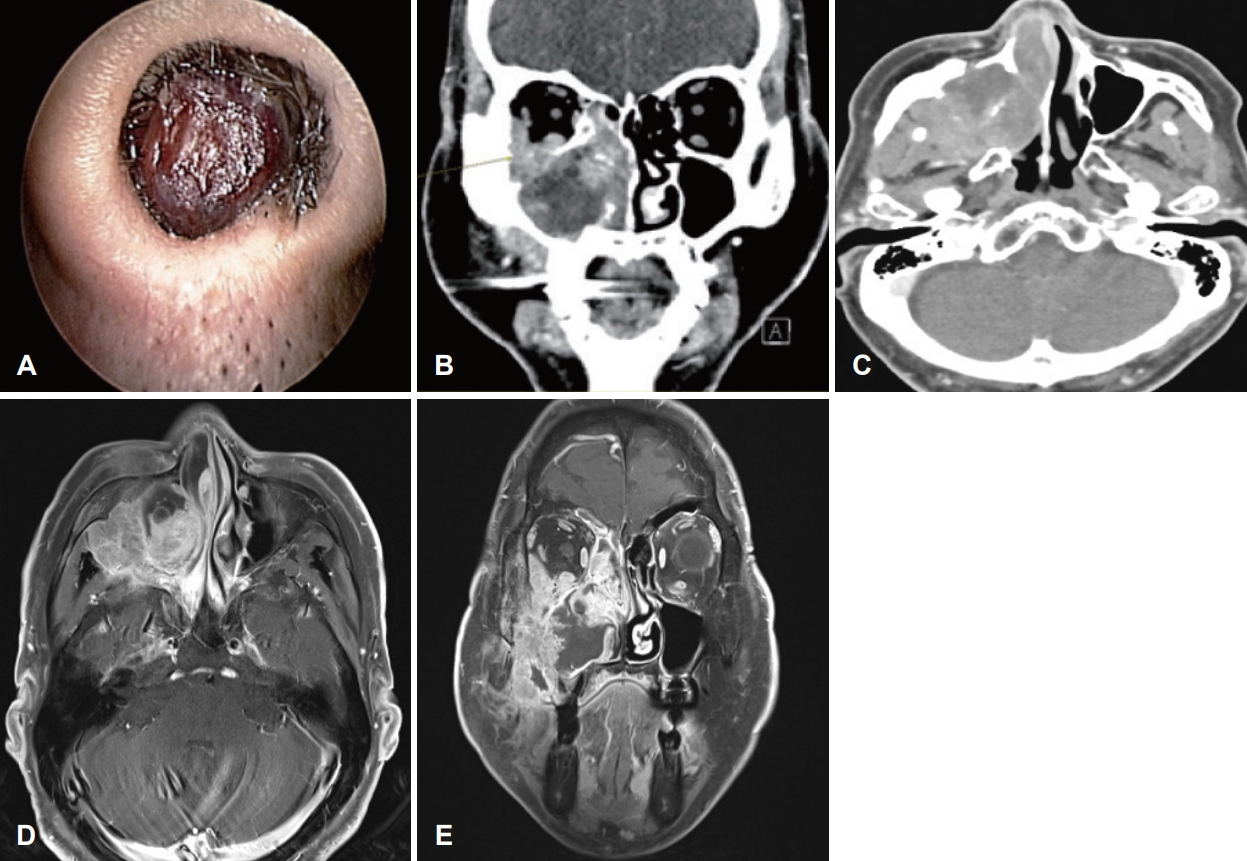
Fig. 2.
The localization of carcinosarcoma defined with PET-CT and its removal by total maxillectomy. A: Whole-body FDG PET-CT shows a hypermetabolic mass in the right maxillary sinus (arrows). B: PET-CT image in the axial plane shows FDG uptake in the maxillary sinus mass invading adjacent ethmoid sinus and nasal cavity (arrows). C: Total maxillectomy defect with orbital contents preserved (black arrow indicates infraorbital capsule, blue arrow indicates buccal fat pad). FDG, fluorodeoxyglucose. 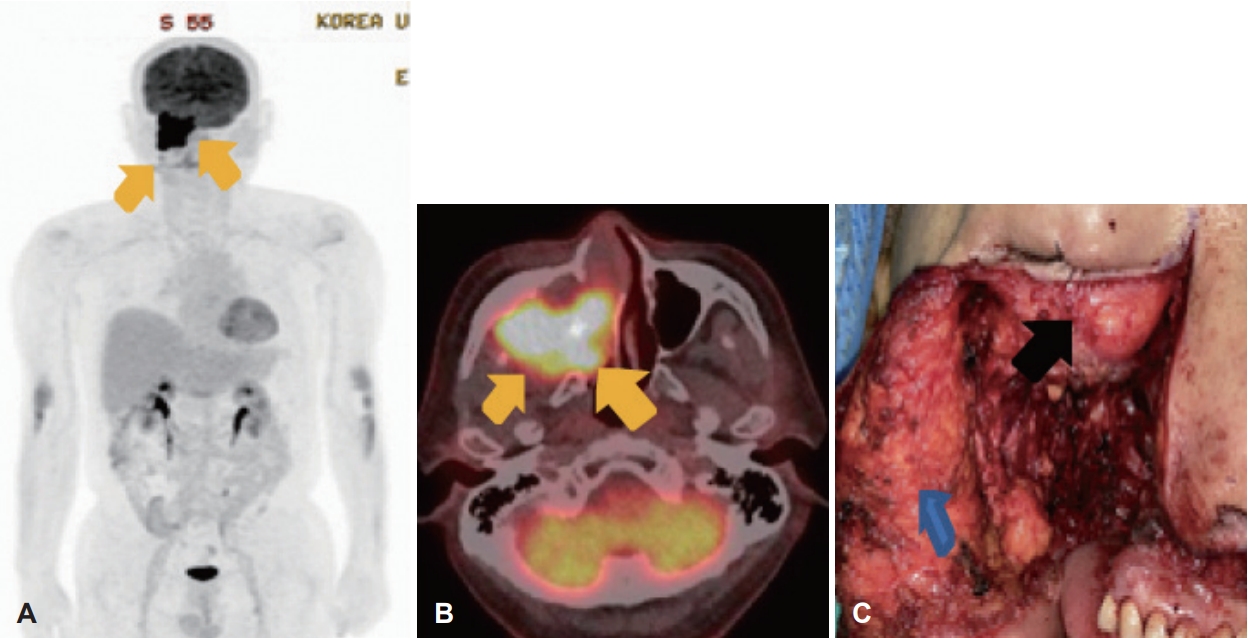
Fig. 3.
Histopathological staining of tumor biopsy specimens. A: Representative H&E-stained section from the excisional biopsy of the malignant sinonasal neoplasm showing squamous cell carcinoma. In higher magnification, the section composed of squamous cell carcinoma with keratinization (arrow) It shows squamous cells which are not organized, have pleomorphism of nuclear structure (×200). B: Pinkish materials which resemble osteoid (unmineralized bone tissue) (arrow) are found between spindle shape sarcomatous cells (arrowheads). This section composed of osteosarcoma (H&E, ×200). C: Positive vimentin staining (×20). D: Positive cytokeratin staining (×20). H&E, hematoxylin and eosin. 
Fig. 4.
CT scan shows a regional recurrence of tumor mass in anterior resection margin of zygomatic bone (arrow). 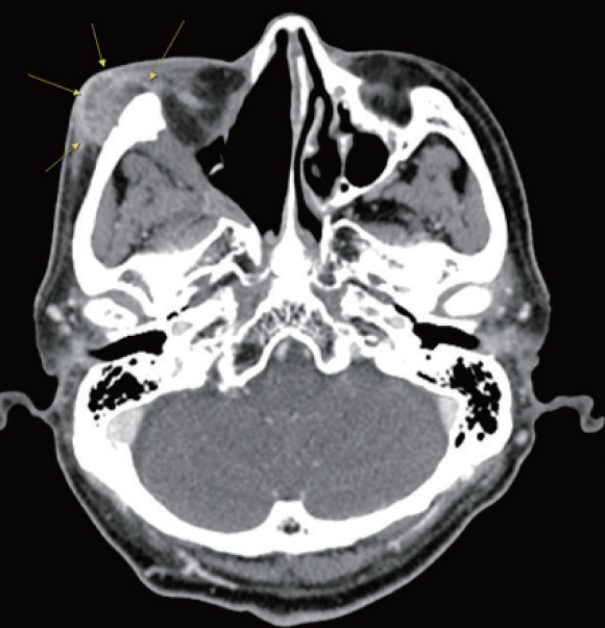
REFERENCES
1. Goellner JR, Devine KD, Weiland LH. Pseudosarcoma of the larynx. Am J Clin Pathol 1973;59(3):312-26.   2. Furuta Y, Nojima T, Terakura N, Fukuda S, Inuyama Y. A rare case of carcinosarcoma of the maxillary sinus with osteosarcomatous differentiation. Auris Nasus Larynx 2001;28 Suppl:S127-9. 3. Koss MN, Hochholzer L, Frommelt RA. Carcinosarcomas of the lung: A clinicopathologic study of 66 patients. Am J Surg Pathol 1999;23(12):1514-26. 4. Chen X, Arend R, Hamele-Bena D, Tergas AI, Hawver M, Tong GX, et al. Uterine carcinosarcomas: Clinical, histopathologic and immunohistochemical characteristics. Int J Gynecol Pathol 2017;36(5):412-9. 7. Tschen JA, Goldberg LH, McGavran MH. Carcinosarcoma of the skin. J Cutan Pathol 1988;15(1):31-5. 8. Stephen J, Batsakis JG, Luna MA, von der Heyden U, Byers RM. True malignant mixed tumors (carcinosarcoma) of salivary glands. Oral Surg Oral Med Oral Pathol 1986;61(6):597-602. 9. Carrillo JF, Güemes A, Ramírez-Ortega MC, Oñate-Ocaña LF. Prognostic factors in maxillary sinus and nasal cavity carcinoma. Eur J Surg Oncol 2005;31(10):1206-12. 10. Bhattacharyya N. Factors affecting survival in maxillary sinus cancer. J Oral Maxillofac Surg 2003;61(9):1016-21. 11. Carson HJ, Tojo DP, Chow JM, Hammadeh R, Raslan WF. Carcinosarcoma of salivary glands with unusual stromal components. Report of two cases and review of the literature. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 1995;79(6):738-46. 12. Tortoledo ME, Luna MA, Batsakis JG. Carcinomas ex pleomorphic adenoma and malignant mixed tumors. Histomorphologic indexes. Arch Otolaryngol 1984;110(3):172-6. 13. Lichtiger B, Mackay B, Tessmer CF. Spindle-cell variant of squamous carcinoma. A light and electron microscopic study of 13 cases. Cancer 1970;26(6):1311-20.
|
|














