м„ң лЎ
м•…м„ұмў…м–‘мқҙ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ҳлҠ” кІҪмҡ°лҠ” л§Өмҡ° л“ңл¬јл©° 비л¶Җ비강м—җм„ң л°ңмғқн•ҳлҠ” м•…м„ұмў…м–‘мқҳ 9%лҘј м°Ём§Җн•ңлӢӨ[1,2]. мөңк·ј 10л…„ лҸҷм•Ҳ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң м–‘м„ұкіј м•…м„ұмў…м–‘мқҳ л№ҲлҸ„м—җ лҢҖн•ң м—°кө¬кІ°кіјм—җм„ң к°ҖмһҘ нқ”н•ң м•…м„ұмў…м–‘мқҖ м•…м„ұнқ‘мғүмў…, plasmacytoma, м „мқҙм•”мқҙлқјкі ліҙкі н•ҳкі мһҲлӢӨ[3]. 32мҳҲлҘј 분м„қн•ң м—°кө¬кІ°кіјм—җм„ңлҠ” м•…м„ұнқ‘мғүмў…, мғҳм•”мў…(adenocarcinoma), нҺёнҸүмғҒн”јм•”, м—°кіЁмңЎмў…(chondrosarcoma) к°Ғк°Ғ 1мҳҲм”© ліҙкі лҗҳм—ҲлӢӨ[4]. мөңк·ј 10л…„к°„ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң м•…м„ұмў…м–‘ 14мҳҲлҘј 분м„қн•ң ліҙкі м—җм„ңлҠ” 6мҳҲк°Җ нҺёнҸүмғҒн”јм•”мқҙм—Ҳкі , м•…м„ұнқ‘мғүмў…, нҳҲкҙҖмЈјмң„м„ёнҸ¬мў…(hemangiopericytoma), мғҳм•”мў…, мғҳлӮӯм•”мў…(adenoid cystic carcinoma), нҡЎл¬ёк·јмңЎмў…(rhabdomycosarcoma) мҲңмқҙм—ҲлӢӨ[5]. мқҙмҷҖ к°ҷмқҙ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң нҺёнҸүмғҒн”јм•”мқҳ л°ңмғқл№ҲлҸ„лҠ” л§Өмҡ° л“ңл¬јлӢӨ. нҺёнҸүмғҒн”јм•”мқҖ л¬јлЎ лӢӨлҘё м•…м„ұмў…м–‘мқҳ л№ҲлҸ„лҸ„ м Ғм–ҙ м№ҳлЈҢл°©лІ•м—җ лҢҖн•ң кІ°кіјк°Җ лҸ„м¶ңлҗҳм–ҙ мһҲм§Җ м•Ҡм•„м„ң м •нҷ•н•ң м№ҳлЈҢлІ•мқҖ нҳ„мһ¬к№Ңм§Җ м •лҰҪлҗҳм–ҙ мһҲм§Җ м•ҠлӢӨ.
к·ёлҹјм—җлҸ„ л¶Ҳкө¬н•ҳкі л№„мӨ‘кІ© м•…м„ұмў…м–‘мқҳ к·јліём Ғмқё м№ҳлЈҢл°©лІ•мқҖ 비강 лӮҙм—җм„ң л°ңмғқн•ң м•…м„ұмў…м–‘мқҳ м№ҳлЈҢлІ•м—җ мӨҖн•ң мҷёкіјм Ғ мў…м–‘м Ғм¶ңмҲ кіј мҲ нӣ„ л°©мӮ¬м„ м№ҳлЈҢмқҙлӢӨ. мөңк·јм—җлҠ” 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң м•…м„ұмў…м–‘мқҳ м ңкұ°м—җлҠ” лӮҙмӢңкІҪмқ„ мқҙмҡ©н•ң ліҙмЎҙм Ғ мҲҳмҲ мқҙ л§Һмқҙ м Ғмҡ©лҗҳкі мһҲлҠ” мӢӨм •мқҙлӢӨ. к·ёлҹ¬лӮҳ мҷёкіјм Ғ м ‘к·јлІ•мқҖ 비мӨ‘кІ©м—җ л°ңмғқн•ң мў…м–‘мқҳ мң„м№ҳ л°Ҹ нҒ¬кё°м—җ л”°лқјм„ң кІ°м •лҗңлӢӨкі ліҙкі н•ҳмҳҖлӢӨ[6].
ліё мҰқлЎҖлҠ” 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң нҺёнҸүмғҒн”јм•”мқҙ 비мӨ‘кІ©мқҳ м—°кіЁл¶Җмң„мҷҖ кіЁл¶Җмң„лҘј л„“кІҢ м№ЁлІ”н•ҳмҳҖкё° л•Ңл¬ём—җ м•”мў…мқ„ 충분нһҲ м ңкұ°н• мҲҳ мһҲлҸ„лЎқ мҲҳмҲ мӢңм•јлҘј нҷ•ліҙн•ҳкё° мң„н•ҙ 비мҷём ‘к·јлІ•мқ„ мқҙмҡ©н•ҳм—¬ м ңкұ°н•ң 1мҳҲлҘј кІҪн—ҳн•ҳмҳҖкё°м—җ л¬ён—Ң кі м°°кіј н•Ёк»ҳ ліҙкі н•ҳкі мһҗ н•ңлӢӨ.
мҰқ лЎҖ
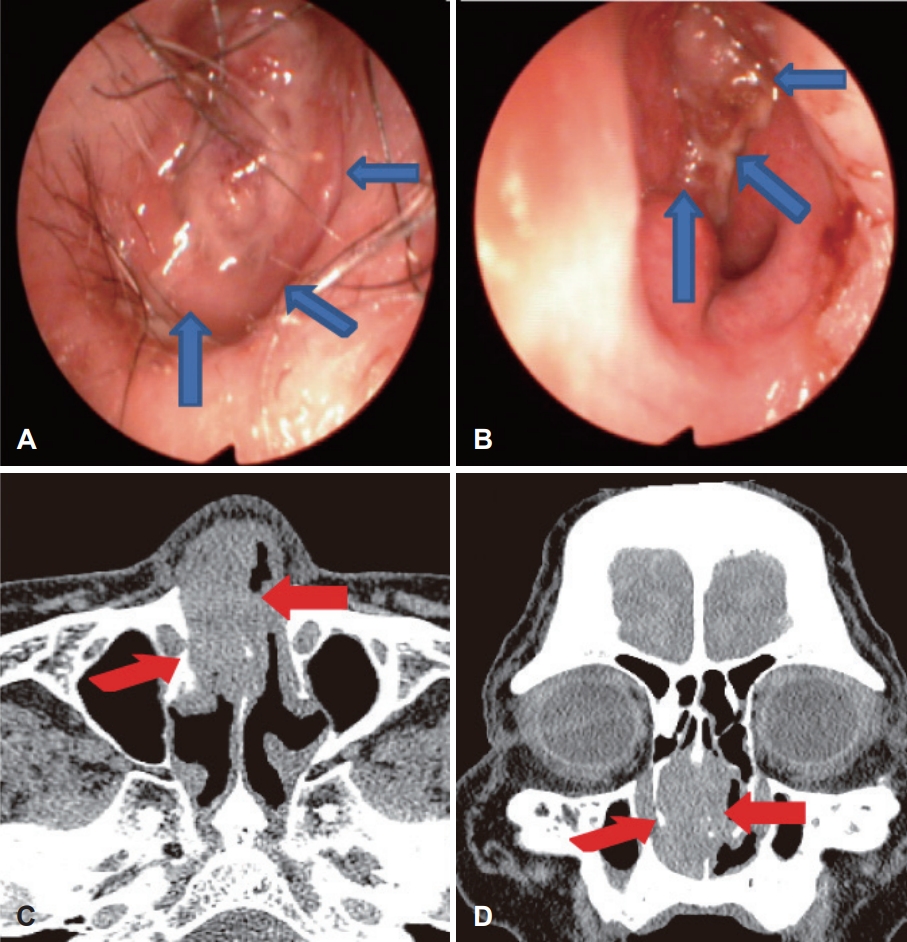
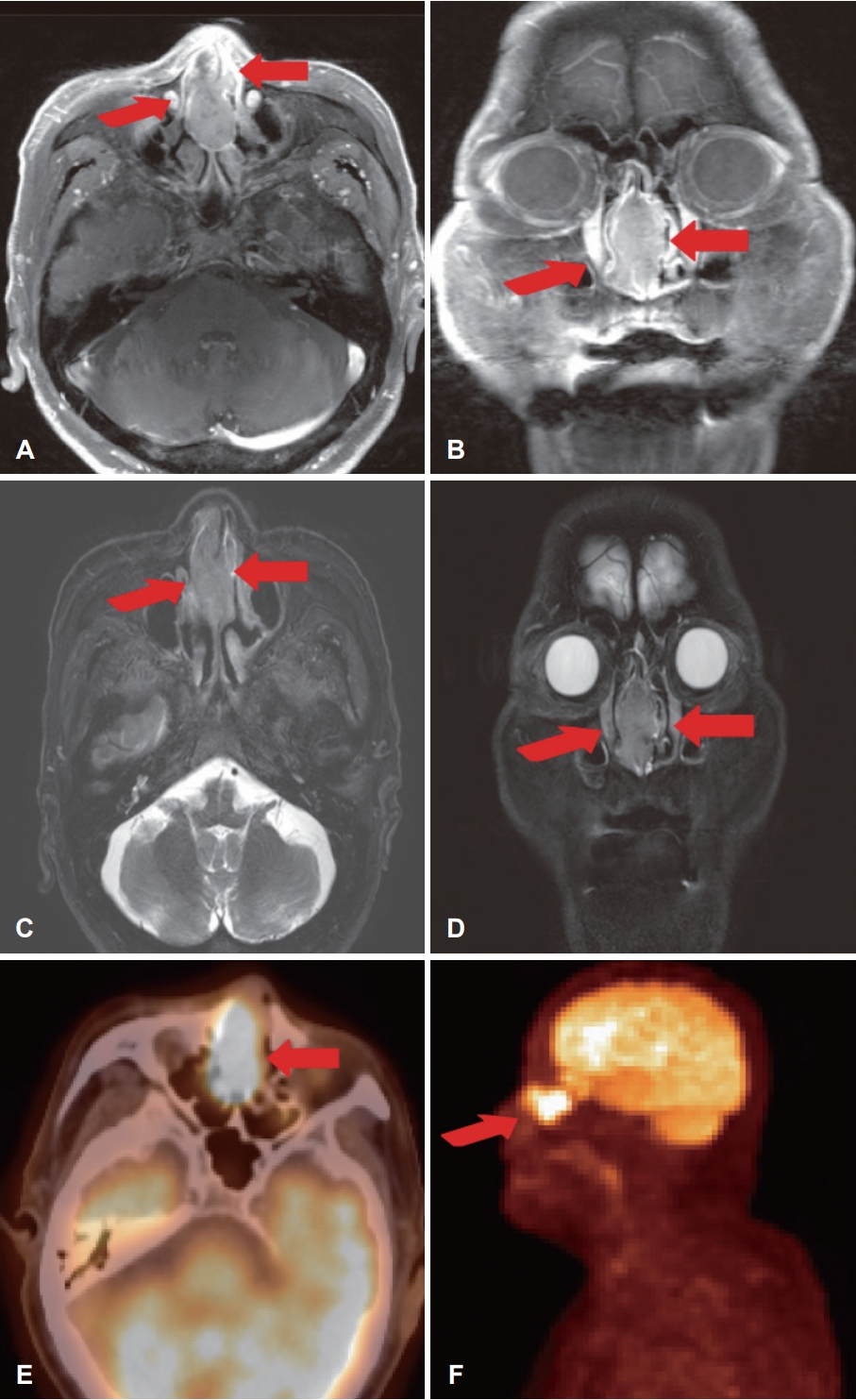
79м„ё лӮЁмһҗ нҷҳмһҗк°Җ 1лӢ¬ м „л¶Җн„° мӢңмһ‘лҗң мҡ°мёЎ 비нҸҗмғүмқ„ мЈјмҶҢлЎң лӮҙмӣҗн•ҳмҳҖлӢӨ. кё°м Җм§Ҳнҷҳмқҙ м—ҶлҠ” нҷҳмһҗмҳҖмңјл©°, 비лӮҙмӢңкІҪ кІҖмӮ¬м—җм„ң мҡ°мёЎ 비강 лӮҙм—җм„ң л¶Ҳк·ңм№ҷн•ң н‘ңл©ҙмқ„ к°Җм§Җкі мһҲлҠ” м„ нҷҚмғү мў…л¬јмқҙ к°Җл“қ мұ„мҡ°кі мһҲмңјл©° мўҢ측비강м—җм„ңлҠ” мў…л¬јмқҙ н•ҳ비갑к°ңмқҳ н‘ңл©ҙк№Ңм§Җ м ‘мҙүлҗҳм–ҙ мһҲлҠ” м–‘мғҒмңјлЎң кҙҖм°°лҗҳм—ҲлӢӨ(Fig. 1A and B). мў…м–‘мңјлЎң мқён•ң мЈјмң„ кіЁнҢҢкҙҙмқҳ м •лҸ„лҘј м •нҷ•н•ҳкІҢ нҢҢм•…н•ҳкё° мң„н•ҳм—¬ мҙ¬мҳҒн•ң л¶Җ비강 м»ҙн“Ён„°лӢЁмёөмҙ¬мҳҒм—җм„ңлҠ” 비мӨ‘кІ©мқҳ м—°кіЁл¶Җ분мқ„ мЈјлЎң м№ЁлІ”н•ҳлҠ” мҶҢкІ¬мқҙ кҙҖм°°лҗҳм—Ҳмңјл©°, 비мӨ‘кІ©мқҳ нӣ„л°ҳл¶ҖмҷҖ мғҒл¶ҖлҘј м°Ём§Җн•ҳлҠ” кіЁл¶Җм—җм„ңлҠ” кіЁнҢҢкҙҙ л°Ҹ м№ЁлІ”мҶҢкІ¬мқҖ кҙҖм°°лҗҳм§Җ м•Ҡм•ҳлӢӨ(Fig. 1C and D). мў…м–‘мқҳ м •нҷ•н•ң м№ЁлІ”л¶Җмң„лҘј нҢҢм•…н•ҳкё° мң„н•ҳм—¬ мӢңн–үн•ң л¶Җ비лҸҷ мһҗкё°кіөлӘ…мҳҒмғҒкІҖмӮ¬м—җм„ңлҠ” gadoliniumмқ„ мӮ¬мҡ©н•ң T1 к°•мЎ°мҳҒмғҒм—җм„ң к· м§Ҳн•ҳкІҢ мЎ°мҳҒмҰқк°•лҗҳлҠ” мў…л¬јмқҙ 비мӨ‘кІ©мқ„ м№ЁлІ”н•ҳкі мһҲлҠ” мҶҢкІ¬мқҙ кҙҖм°°лҗҳм—Ҳкі , лӢӨлҘё л¶Җмң„лЎңмқҳ м№ЁлІ”мқҖ нҷ•мқёлҗҳм§Җ м•Ҡм•ҳлӢӨ(Fig. 2A and B). T2 к°•мЎ°мҳҒмғҒм—җм„ңлҠ” 비мӨ‘кІ©мқ„ м№ЁлІ”н•ҳкі мһҲлҠ” м ҖмӢ нҳёмқҳ к°•лҸ„лҘј кҙҖм°°н• мҲҳ мһҲм—ҲлӢӨ(Fig. 2C and D). мӢ мІҙкІҖ진мғҒ кІҪл¶Җм—җм„ң мҙүм§ҖлҗҳлҠ” мў…л¬јмқҖ м—Ҷм—Ҳкі , м „мӢ м–‘м „мһҗлӢЁмёөмҙ¬мҳҒ мҳҒмғҒм—җм„ң мҡ°мёЎ 비강мқҳ мў…л¬јмҷё кі лҢҖмӮ¬м„ұ лі‘ліҖмқҖ м—Ҷм–ҙ м „мӢ м „мқҙлҠ” кҙҖм°°лҗҳм§Җ м•Ҡм•ҳлӢӨ(Fig. 2E and F).
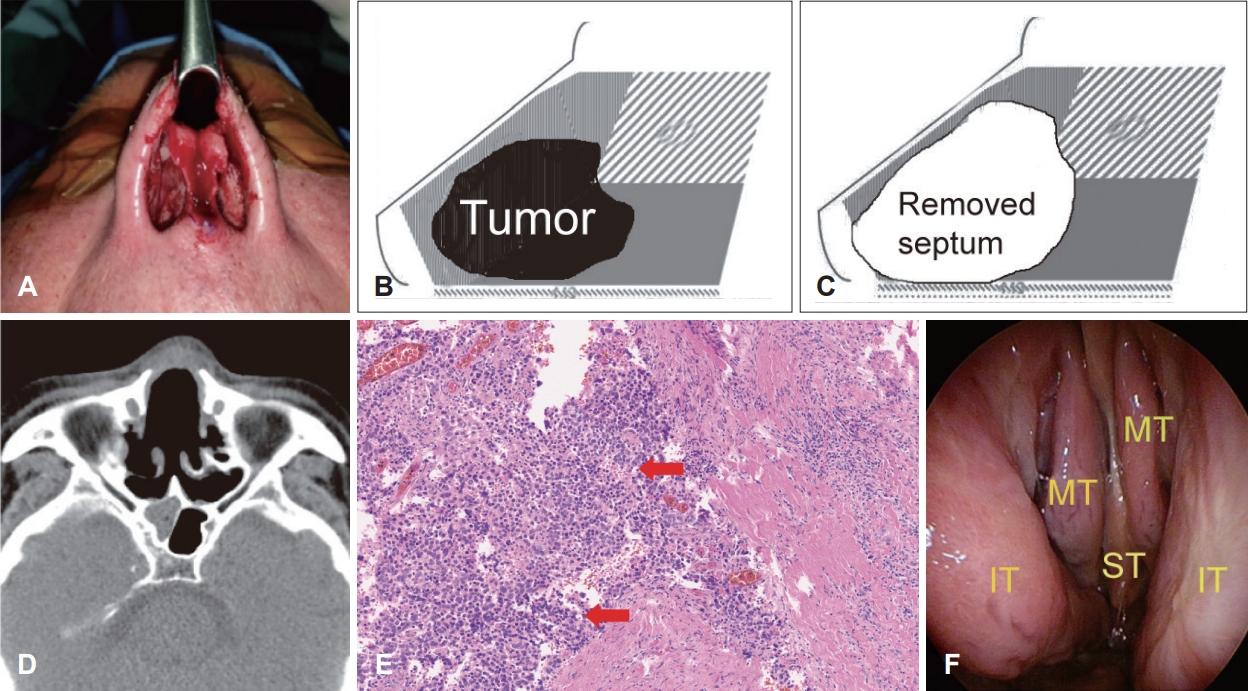
мҷёлһҳм—җм„ң мӢңн–үн•ң мЎ°м§ҒкІҖмӮ¬мғҒ мӨ‘분нҷ”нҳ•мқҳ нҺёнҸүм„ёнҸ¬м•”мқҙ 진лӢЁлҗҳм—ҲлӢӨ. мқҙм—җ мҷ„м „м Ҳм ңлҘј мң„н•ҙ м „мӢ л§Ҳм·Ён•ҳм—җ 비주м—җ м—ӯVм Ҳк°ң(inverted V shape incision)лҘј н•ң лӢӨмқҢ л§үм—°кіЁн”јнҢҗ(mucoperichodnrium flap)мқ„ л“Өм–ҙ мҳ¬лҰ¬кі 비мқөм—°кіЁкіј мҷёмёЎл№„м—°кіЁмқҳ м „мһҘмқ„ л…ём¶ңмӢңмј°лӢӨ(Fig. 3A). к·ё лӢӨмқҢ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң мў…м–‘мқҳ м№ЁлІ”л¶Җмң„лҘј нҷ•мқён•ҳкі 3-4 mm м •лҸ„мқҳ м Ҳм ңм—°мқ„ мң м§Җн•ҳл©ҙм„ң мў…м–‘мқ„ м ңкұ°н•ҳмҳҖлӢӨ(Fig. 3B and C). мҲҳмҲ мӢң нҷ•мқёлҗң мў…м–‘мқҳ м№ЁлІ”л¶Җмң„лҘј мҡ”м•Ҫн•ҳл©ҙ л№„м „м •мқҙлӮҳ мҷёмёЎ 비연골л¶Җмң„мқҳ м№ЁлІ”мқҖ м—Ҷм—Ҳмңјл©°, 비мӨ‘кІ©л¶Җмң„м—җ көӯн•ңлҗҳм–ҙ мһҲм—ҲлӢӨ. к°ҖлҠҘн•ң н•ң L-strutмқҳ м§Җм§ҖмғҒнғңлҘј мң м§Җн•ҳлҸ„лЎқ 비мӨ‘кІ©мқҳ мў…м–‘мқ„ м ңкұ°н• мҲҳ мһҲм—ҲлӢӨ. мҲ нӣ„ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң нҺёнҸүмғҒн”јм•”мқҳ лі‘кё°лҠ” American Joint Committee on Cancer (AJCC) 8thм—җ л”°лҘҙл©ҙ T1N0M0, stage 1лЎң нҢҗлӢЁлҗҳм—ҲлӢӨ.
мЎ°м§Ғн•ҷм Ғ кІҖмӮ¬мғҒ мҷёлһҳм—җм„ң мӢңн–үн•ң мЎ°м§ҒкІҖмӮ¬мҷҖ л§Ҳм°¬к°Җм§ҖлЎң мӨ‘분нҷ”нҳ• нҺёнҸүм„ёнҸ¬м•”мңјлЎң 진лӢЁлҗҳм—Ҳмңјл©° м Ҳм ңл©ҙмқҖ мқҢм„ұмқҙм—Ҳкі , лі‘лҰ¬мҶҢкІ¬м—җм„ң нҳҲкҙҖмқҙлӮҳ мӢ кІҪм„ёнҸ¬мқҳ м№ЁлІ”м—җ лҢҖн•ҙм„ңлҠ” м–ёкёүн•ҳм§Җ м•Ҡм•ҳлӢӨ(Fig. 3E). мҲ нӣ„ 1лӢ¬м§ё л°©мӮ¬м„ м№ҳлЈҢ(200 Gy/30 fractions)лҘј мӢңн–үн•ҳмҳҖмңјл©° мҲ нӣ„ 2л…„ лҸҷм•Ҳ 1-2лӢ¬ к°„кІ©мңјлЎң 추м Ғ кҙҖм°°н•ң кІ°кіј мҲ нӣ„ 2л…„мқҙ м§ҖлӮң нҳ„мһ¬к№Ңм§Җ мһ¬л°ңмҶҢкІ¬кіј мҷёл№„мқҳ нҳ•нғң мҰү, м•ҲмһҘмҪ”мҷҖ к°ҷмқҖ нҳ•нғңн•ҷм Ғ ліҖнҷ”лҠ” кҙҖм°°лҗҳм§Җ м•Ҡм•ҳлӢӨ(Fig. 3D and F).
кі м°°
비мӨ‘кІ©м—җм„ң л°ңкІ¬лҗҳлҠ” м•…м„ұмў…м–‘мқҖ л№„м „м •мқҙлӮҳ л¶Җ비лҸҷм—җм„ң л°ңмғқн•ң м•”мў…мқҙ 비мӨ‘кІ©мңјлЎң нҢҢкёүлҗҳм–ҙ л°ңкІ¬лҗҳлҠ” кІҪмҡ°к°Җ нқ”н•ҳкі , 비мӨ‘кІ© мһҗмІҙм—җм„ң мӣҗл°ңм„ұмңјлЎң л°ңмғқн•ң м•”мў…мқҖ л§Өмҡ° л“ңл¬јлӢӨ. 비мӨ‘кІ©м—җм„ң л°ңмғқн•ҳлҠ” м•”мў…м—җм„ңлҠ” нҺёнҸүм„ёнҸ¬м•”мқҙ к°ҖмһҘ л§ҺлӢӨ[7]. мқҙмҷҖк°ҷмқҙ нқ¬мҶҢм„ұ л•Ңл¬ём—җ AJCC 분лҘҳлІ•м—җм„ңлҠ” лҸ…мһҗм Ғмқё лі‘кё°к°Җ м—Ҷмқҙ 비л¶Җ비лҸҷ м•…м„ұмў…м–‘мқҳ н•ҳл¶ҖлӢЁмң„лЎң 분лҘҳлҗҳкі мһҲлӢӨ[1,8].
비нҸҗмғү, л°ҳліөлҗҳлҠ” 비м¶ңнҳҲ, нҳ№мқҖ 비루 л“ұмқ„ лҸҷл°ҳн•ҳлҠ” 비염과 к°ҷмқҖ 비нҠ№мқҙм Ғмқё мҰқмғҒмқҙ лӮҳнғҖлӮҳкё° л•Ңл¬ём—җ 비мӨ‘кІ©мқҳ м•…м„ұ мў…м–‘мқҳ 진лӢЁмқҖ мһҗмЈј м§Җм—°лҗҳлҠ” кІҪн–Ҙмқҙ мһҲлӢӨ[7]. лӮҙмӢңкІҪ кІҖмӮ¬к°Җ 진лӢЁм—җ л§Өмҡ° мӨ‘мҡ”н•ҳл©°, 비мӨ‘кІ©м—җм„ң л°ңнҳ„лҗҳлҠ” м•…м„ұмў…м–‘мқҳ лӮҙмӢңкІҪ мҶҢкІ¬мқҖ м ңмқј нқ”н•ң кІғмқҙ нҳ№лҚ©м–ҙлҰ¬лЎң л°ңкІ¬лҗҳлҠ” кІҪмҡ°мқҙкі , к·ё лӢӨмқҢ м җл§үк¶Өм–‘мңјлЎң л°ңкІ¬лҗҳлҠ” кІҪмҡ°к°Җ нқ”н•ҳлӢӨ. м„ё лІҲм§ёлЎң л§ҺмқҖ мҳҲлҠ” 비мӨ‘кІ©мІңкіөмқҳ мғҒнғңлЎң л°ңкІ¬лҗҳлҠ” кІҪмҡ°мқҙл©°, 진лӢЁ л°Ҹ м№ҳлЈҢк°Җ м§Җм—°лҗң кІҪмҡ°м—җлҠ” мҷёл№„к°Җ ліҖнҳ•лҗң мғҒнғңлЎң л°ңкІ¬лҗҳкё°лҸ„ н•ңлӢӨ[1,2,7,9,10]. нҠ№нһҲ м§ҖмҶҚм Ғмқё м җл§үмқҳ лі‘ліҖмқҙ мҪ”л”ұм§ҖлЎң лҚ®нҳҖмһҲкұ°лӮҳ к°„н—җм Ғмқё 비м¶ңнҳҲмқҙ мһҲлҠ” кІҪмҡ° 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң м•”мў…мқ„ мқҳмӢ¬н•ҙм•ј н•ңлӢӨ[11]. ліё мҰқлЎҖм—җм„ңлҠ” лӢӨлҘё мҰқмғҒ м—Ҷмқҙ 비нҸҗмғүмқҙ л°ңмғқн•ҳм—¬ лӮҙмӣҗн•ҳмҳҖкі , лӮҙмӢңкІҪ кІҖмӮ¬кІ°кіј мҡ°мёЎ 비강мқ„ мҷ„м „нһҲ нҸҗмҮ„н•ҳкі мһҲлҠ” мў…м–‘лҚ©м–ҙлҰ¬лЎң л°ңкІ¬лҗҳм—ҲлӢӨ. мқҙмҷҖ к°ҷмқҖ м җл§үмҶҢкІ¬мқҙ лӮҙмӢңкІҪ кІҖмӮ¬ мӢңм—җ л°ңкІ¬лҗҳл©ҙ мЎ°м§ҒкІҖмӮ¬лЎң к°„лӢЁн•ҳкІҢ 진лӢЁлҗ мҲҳ мһҲлӢӨ. 비мӨ‘кІ© мІңкіөкіј м—°кҙҖлҗҳм–ҙ л°ңкІ¬лҗҳлҠ” кІҪмҡ°м—җлҠ” мІңкіөмЈјмң„ м җл§үмқҙ л¶Ҳк·ңм№ҷн•ң нҳ•нғңлҘј лқ„кұ°лӮҳ мІңкіөнҒ¬кё°к°Җ м җм җ мҰқк°Җн•ҳлҠ” кІҪмҡ° мІңкіөмЈјмң„ м җл§үмқҳ мЎ°м§Ғ кІҖмӮ¬к°Җ н•„мҲҳм ҒмқҙлӢӨ[1].
Janik л“ұ[12]мқҳ ліҙкі м—җ мқҳн•ҳл©ҙ 비л¶Җ비강мқҳ лӢӨлҘё л¶Җмң„м—җм„ң л°ңмғқн•ң нҺёнҸүмғҒн”јм•”ліҙлӢӨ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң нҺёнҸүмғҒн”јм•”мқҖ мһ„нҢҢм Ҳм „мқҙмңЁмқҙ лҶ’лӢӨкі н•ҳкі мһҲлӢӨ. л”°лқјм„ң м»ҙн“Ён„°лӢЁмёөмҙ¬мҳҒмқҙ кІҪл¶Җ лҰјн”„м Ҳ м „мқҙ л°Ҹ мӣҗл°ңл¶Җмң„мқё 비мӨ‘кІ©мқ„ нҸ¬н•Ён•ң 비л¶Җ비강мқҳ м№ЁлІ” л°Ҹ кіЁнҢҢкҙҙ м •лҸ„лҘј нҢҢм•…н•ҳкё° мң„н•ҙ н•„мҡ”н•ҳл©°, мһҗкё°кіөлӘ…мҳҒмғҒмҙ¬мҳҒмқҖ м—°л¶ҖмЎ°м§Ғ м№ЁлІ”м •лҸ„ л°Ҹ л‘җк°ңк°• лӮҙ м№ЁлІ”м •лҸ„лҘј нҢҢм•…н•ҳкё° мң„н•ҙ мӮ¬мҡ©н• мҲҳ мһҲлӢӨ. ліёлЎҖм—җм„ң мӢңн–үн•ң м»ҙн“Ён„°лӢЁмёөмҙ¬мҳҒмқ„ нҸ¬н•Ён•ң мҳҒмғҒкІҖмӮ¬м—җм„ң лӢӨлҘё л¶Җмң„лЎңмқҳ м „мқҙлҠ” л°ңкІ¬лҗҳм§Җ м•Ҡм•„ мӣҗл°ңл¶Җмң„мқҳ мў…м–‘мқ„ 비мӨ‘кІ©мқ„ нҸ¬н•Ён•ҳм—¬ м ңкұ°н•ҳкІҢ лҗҳм—ҲлӢӨ.
비мӨ‘кІ©м—җм„ң л°ңмғқн•ң м•…м„ұмў…м–‘мқҳ м№ҳлЈҢл°©лІ•мқҖ мҷёкіјм Ғ м Ҳм ң, л°©мӮ¬м„ м№ҳлЈҢ, нҳ№мқҖ ліөн•©м№ҳлЈҢк°Җ к¶Ңмң лҗңлӢӨ[7]. лӮҙмӢңкІҪмқҙ лҸ„мһ…лҗң мқҙнӣ„ мў…л¬јмқҳ нҒ¬кё°к°Җ мһ‘мқҖ мҙҲкё° лӢЁкі„м—җм„ңлҠ” лӮҙмӢңкІҪмқ„ мқҙмҡ©н•ң м Ҳм ңмҲ мқҙ к°ҖлҠҘн•ҳкі мҡ°мҲҳн•ң м№ҳлЈҢкІ°кіјлҘј ліҙм—¬мЈјкі мһҲлӢӨ[7]. лӮҙмӢңкІҪмқ„ мқҙмҡ©н•ң мҲҳмҲ лІ•мқҖ мҲ мһҗк°Җ н•ңмҶҗмңјлЎңл§Ң мҲҳмҲ мқ„ н•ҙм•ј н•ҳкі , 1 cm мқҙмғҒмқҳ нҒ° лі‘ліҖмқ„ м ңкұ°н•ҳкұ°лӮҳ мЎ°мһ‘н•ҳлҠ” кІҪмҡ°м—җлҠ” м ңм•Ҫмқҙ л”°лҘёлӢӨ. лҳҗн•ң лі‘ліҖмқҳ м•һмӘҪл§Ңмқҙ ліҙмқҙкё° л•Ңл¬ём—җ нҒ¬кё°к°Җ нҒ° лі‘ліҖмқҳ кІҪмҡ° мҷ„м „н•ң м Ҳм ңк°Җ нһҳл“Ө мҲҳ мһҲлӢӨ. л”°лқјм„ң мў…м–‘мқҳ мң„м№ҳмҷҖ нҒ¬кё°м—җ л”°лқј лӢӨм–‘н•ң мҲҳмҲ м Ғ м ‘к·јл°©лІ•мқҙ мӮ¬мҡ©лҗ мҲҳ мһҲлӢӨ[6]. 비мӨ‘кІ©мқҳ м „л°ҳл¶Җм—җ мң„м№ҳн•ң мў…м–‘мқҖ мҷёмёЎл№„мқөм Ҳк°ң м ‘к·јлІ•мңјлЎң м ‘к·јмқҙ к°ҖлҠҘн•ҳл©° 비мӨ‘кІ©мқҳ нӣ„л°ҳл¶Җм—җ мң„м№ҳн•ң мў…м–‘мқҳ кІҪмҡ°лҠ” кө¬мҲңн•ҳм Ҳк°ң(sublabial incision)лҘј н•ң нӣ„ Caldwell-Luc м ‘к·јлІ•мқ„ нҶөн•ҳм—¬ м ңкұ°н• мҲҳ мһҲлӢӨ. 비강мқҳ н•ҳл¶ҖмҷҖ 비мӨ‘кІ©мқ„ м№ЁлІ”н•ң мў…м–‘мқҳ кІҪмҡ° 비мқөм Ҳк°ңмҷҖ кө¬мҲңм Ҳк°ңлҘј нҶөн•ҳм—¬ м ңкұ°к°Җ к°ҖлҠҘн•ҳлӢӨ. л§Өмҡ° нҒ° мў…м–‘мқҙ 비мӨ‘кІ©кіј 비강мқҳ мҷёмёЎлІҪкіј н•ҳл¶ҖлҘј м№ЁлІ”н•ң кІҪмҡ°лҠ” Weber-Ferguson м Ҳк°ңлІ•мқҙ мӮ¬мҡ©лҗ мҲҳ мһҲлӢӨ[6].
비мӨ‘кІ©м—җ л°ңмғқн•ң мў…м–‘мқҳ мҷёкіјм Ғ м Ҳм ңмқҳ лӘ©м ҒмқҖ 충분н•ң м Ҳм ңм—° мқҢм„ұмқ„ нҷ•ліҙн•ҳл©ҙм„ң мў…м–‘мқ„ мҷ„м „н•ҳкІҢ м ңкұ°н•ҳлҠ” кІғмқҙкі , кё°лҠҘм ҒмңјлЎң нҳ№мқҖ м„ұнҳ•м ҒмңјлЎң л§ҢмЎұн• л§Ңн•ң кІ°кіјлҘј м–»кё° мң„н•ҙ мҷёл№„мқҳ нҳ•нғңн•ҷм Ғ мқҙмғҒмқ„ мһ¬кұҙн•ҳлҠ” кІғмқҙлӢӨ. ліёлЎҖм—җм„ңлҠ” 비мӨ‘кІ©мқҳ м—°кіЁл¶ҖмҷҖ кіЁл¶ҖлҘј кҙ‘лІ”мң„н•ҳкІҢ м№ЁлІ”н•ң нҺёнҸүмғҒн”јм•”мқ„ м ңкұ°н•ҳкі кё°лҠҘн•ҷм Ғ нҳ№мқҖ нҳ•нғңн•ҷм Ғ мқҙмғҒмқ„ мһ¬кұҙн• лӘ©м ҒмңјлЎң мҷёл№„м ‘к·јлІ•мқ„ мқҙмҡ©н•ҳкІҢ лҗҳм—ҲлӢӨ. мҷёл№„м ‘к·јлІ•мқҖ мҲҳмҲ мӢңм•јлҘј 충분н•ҳкІҢ нҷ•ліҙн•ҳлҠ” кІғмқ„ к°ҖлҠҘн•ҳкІҢ н•ҳмҳҖкі , 비мӨ‘кІ©мқҳ мғҒл¶ҖмҷҖ м „л°©мқҳ 비주л¶Җмң„м—җм„ң 비мӨ‘кІ©мқ„ мң м§Җн•ҳлҸ„лЎқ L-strutмқ„ ліҙмЎҙн•ҳлҸ„лЎқ м Ҳм ңм—° мқҢм„ұмқ„ нҷ•ліҙн•ҳл©ҙм„ң мў…м–‘мқ„ м ңкұ°н•ҳкІҢ лҗҳм—ҲлӢӨ. мҲ нӣ„ л°©мӮ¬м„ м№ҳлЈҢлҘј н•ҳмҳҖкі мҲ нӣ„ 2л…„мқҙ м§ҖлӮң нҳ„мһ¬к№Ңм§Җ нҺёнҸүмғҒн”јм•”мқҳ мһ¬л°ңмқҖ кҙҖм°°лҗҳм§Җ м•Ҡм•ҳлӢӨ.
м Җмһҗл“ӨмқҖ мҪ”л§үнһҳмңјлЎң лӮҙмӣҗн•ң нҷҳмһҗм—җм„ң мҳҒмғҒмқҳн•ҷм Ғ кІҖмӮ¬мҷҖ 비мҷём ‘к·јлІ•мқ„ мқҙмҡ©н•ң мҲҳмҲ м Ғ м№ҳлЈҢ л°Ҹ мЎ°м§ҒкІҖмӮ¬лҘј нҶөн•ҙ 비мӨ‘кІ©м—җм„ң л°ңмғқн•ң нҺёнҸүмғҒн”јм•” 1мҳҲлҘј м№ҳн—ҳн•ҳмҳҖкё°м—җ л¬ён—Ң кі м°°кіј н•Ёк»ҳ ліҙкі н•ҳлҠ” л°”мқҙлӢӨ.