ΉΕε Έκι
Nuclear protein in testis midline carcinoma (NMC)ΈΛΦ ΊΟ╕ΊΠΚΉΕ╕ΊΠυΉΧΦΉζα ΈπνΉγ░ Ά│╡Ά▓σΉιΒΉζ╕ ΊΧε ΉΧΕΉλΖΉε╝Έκε, nuclear protein in testis (NUT) ΉειΉιΕΉηΡΉζα ΉΩ╝ΉΔΚΉ▓┤ ΉηυΈ░░ΉΩ┤ΉζΕ ΊΛ╣ΉπΧΉε╝Έκε ΊΧεΈΜν[1]. ΈΝΑΈ╢ΑΈ╢ΕΉζα Ά▓╜Ήγ░ΉΩΡΉΕε bromodomain-containing protein 4 (BRD4)-NUT fusion oncogene ΊαΧΊΔεΉζα ΉηυΈ░░ΉΩ┤ΉζΕ Έ│┤Ήζ┤Έσ░, BRD3, nuclear receptor binding SET domain protein 3 (NSD3) ΈΥ▒Ήζα ΉειΉιΕΉηΡ Έ│ΑΉζ┤ΈΠΕ Ά░ΑΈΛξΊΧε Ά▓ΔΉε╝Έκε ΉΧΝΈινΉι╕ ΉηΙΈΜν[2]. Ήζ╝Έ░αΉιΒΉζ╕ ΊΟ╕ΊΠΚΉΕ╕ΊΠυΉΧΦΉλΖΉζα Έ│╡ΉηκΊΧε ΊΧ╡ΊαΧΆ│╝ΈΛΦ ΈΝΑΉκ░ΉιΒΉε╝Έκε NMCΈΛΦ t(15;19) ΉηυΈ░░ΉΩ┤Ήε╝Έκε ΈΝΑΊΣεΈΡαΈΛΦ Ά░ΕΈΜρΊΧε ΊΧ╡ΊαΧΉζΕ Έ│┤Ήζ╕ΈΜν. MidlineΉζ┤Έζ╝ΈΛΦ ΉγσΉΨ┤ΈΛΦ NMCΆ░Α Ήμ╝Έκε Ές╕ ΉνΣΉΧβΉζα ΊΧ┤Έ╢ΑΊΧβΉιΒ Έ╢ΑΉεΕΉΩΡΉΕε Έ░εΉΔζΊΧαΆ╕░ ΈΧΝΈυ╕ΉΩΡ ΉΓυΉγσΈΡαΉΩΙΉε╝Έσ░, ΊζΚΈ╢Α(51%), ΈΣΡΆ▓╜Έ╢Α(41%), Ά│ρΈ╢Α Έ░Π ΉΩ░Ήκ░ΉπΒ(6%)ΉΩΡΉΕε Έ░εΉΔζΊΧεΈΜν[1-3]. ΉπΕΈΜρΉζΑ Ά░ΕΈΜρΊΧαΆ▓ΝΈΛΦ NUT proteinΉΩΡ ΈΝΑΊΧε ΊΧ╡ Έσ┤ΉΩφΈ░αΉζΣΉζΕ Ά┤ΑΉ░░ΊΧαΈΛΦ Ά▓ΔΉζ┤Έσ░, ΉλΖΉΨΣ ΉειΉιΕΉηΡΈξ╝ ΊΛ╣ΉιΧΊΧαΆ╕░ ΉεΕΊΧε Ή╢ΦΆ░ΑΉιΒΉζ╕ ΉΩ░Ά╡υΈΥνΉζ┤ Ά╢ΝΉηξΈΡαΉπΑΈπΝ ΊΧΕΉΙαΉιΒΉζ╕ Ά▓ΔΉζΑ ΉΧΕΈΜΙΈΜν. ΉαΙΊδΕΈΛΦ ΉλΜΉπΑ ΉΧΛΉΧΕ ΊΠΚΆ╖ι ΉΔζΉκ┤Ά╕░Ά░ΕΉζΑ 6.7Ά░εΉδΦΈκε Έ│┤Ά│ιΈΡαΉΩΙΉε╝Έσ░, Ή┤ΙΆ╕░Ήζα ΊΧφΉΧΦΈ░σΉΓυΉΕι Έ│╡ΊΧσΉγΦΈ▓ΧΉΩΡΈΛΦ Έ░αΉζΣΉζ┤ ΉηΙΉε╝ΈΓα ΈΝΑΈ╢ΑΈ╢ΕΉζα Ά▓╜Ήγ░ΉΩΡΉΕε ΉηυΈ░εΊΧαΈσ░ Ήζ┤ΊδΕΉζα Ή╣αΈμΝΉΩΡΈΛΦ Έ░αΉζΣΉζ┤ ΉλΜΉπΑ ΉΧΛΉζΑ Ά▓ΔΉε╝Έκε ΉΧΝΈινΉι╕ ΉηΙΈΜν[3].
ΉΧΕΉπΒΆ╣ΝΉπΑ NMCΈΛΦ ΈΥεΈυ╝Ά▓Ν Έ│┤Ά│ιΈΡαΆ│ι ΉηΙΉε╝Έσ░ ΊΛ╣ΊηΙ ΊδΕΈΣΡΉΩΡ Έ░εΉΔζΊΧε NMCΈΛΦ ΉπΑΆ╕ΙΆ╣ΝΉπΑ 8ΉαΙΆ░Α Έ│┤Ά│ιΈΡαΉΩΙΈΜν. Έ│╕ ΉιΑΉηΡΈΥνΉζΑ Ή▓τ ΉΙαΉΙι ΊδΕ Ά▓╜Έ╢Α ΈΜρΉΙε ΈΗΞΉΨΣΉε╝Έκε ΉπΕΈΜρΈΡαΉΩΙΉε╝ΈΓα ΈΣΡ Έ▓ΙΉπ╕ ΉΙαΉΙιΉΩΡΉΕε ΊδΕΈΣΡ ΊΟ╕ΊΠΚΉΕ╕ΊΠυΉΧΦΉλΖ Ά▓╜Έ╢ΑΉιΕΉζ┤Έκε ΊβΧΉζ╕ΈΡαΉΩΙΆ│ι, Ή╢ΦΆ░ΑΈκε ΉΜεΊΨΚΊΧε Ά▓ΑΉΓυΉΔΒ NMCΈκε ΉπΕΈΜρΈΡε ΉοζΈκΑΈξ╝ Έ│┤Ά│ιΊΧαΆ│ιΉηΡ ΊΧεΈΜν.
Ήοζ ΈκΑ
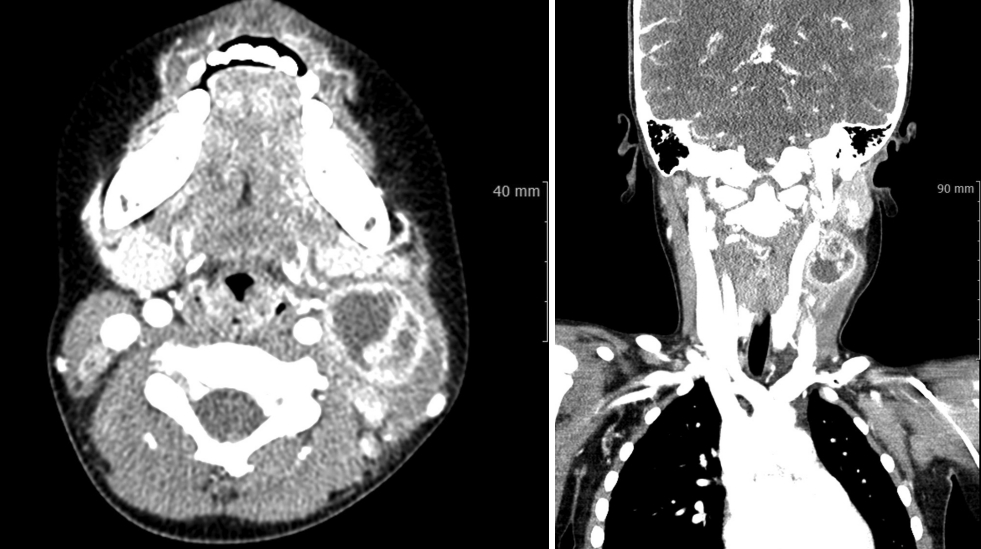
ΊΛ╣Ήζ┤ Ά│╝Ά▒░ΈιξΉζ┤ ΉΩΗΈΛΦ 4ΉΕ╕ ΈΓρΊβαΉζ┤ ΈΓ┤ΉδΡ 4Ήζ╝ ΉιΕΈ╢ΑΊΕ░ ΈπΝΉι╕ΉπΕ ΉλΝΉ╕κ ΉΧΖΊΧαΈ╢ΑΉζα ΉλΖΉ░╜ΉζΕ Ήμ╝ΉΗΝΈκε ΈΓ┤ΉδΡΊΧαΉαΑΈΜν. Ήβ╕ΈηαΉΩΡΉΕε ΉΜεΊΨΚΊΧε ΉΜιΉ▓┤Ά▓ΑΉπΕΉΔΒ ΉλΝΉ╕κ ΉΧΖΊΧαΈ╢ΑΉΩΡ ΈΦ▒ΈΦ▒ΊΧαΆ▓Ν ΈπΝΉι╕ΉπΑΈΛΦ ΉλΖΈυ╝Ήζ┤ Ή┤ΚΉπΕΈΡαΉΩΙΆ│ι Έ░εΉπΕΉζ┤ ΈΠβΈ░αΈΡαΉΩΙΉε╝Έσ░ Έ░εΉΩ┤ΉζΑ ΉΩΗΉΩΙΈΜν. Ά╡υΆ░Χ ΉΜεΉπΕ ΉΔΒΉΩΡΉΕε ΊΛ╣Ήζ┤ ΉΓυΊΧφΉζΑ Έ░εΆ▓υΈΡαΉπΑ ΉΧΛΉΧαΉε╝Έσ░ ΊδΕΈΣΡΈΛΦ ΊβαΉΧΕΉζα ΊαΣΉκ░Ά░Α ΉΨ┤ΈινΉδΝ Ά▓ΑΉΓυΊΧαΉπΑ Ές╗ΊΧαΉαΑΈΜν. ΈπΡΉ┤ΙΊαΙΉΧκΆ▓ΑΉΓυΉΔΒ Έ░▒ΊαΙΆ╡υ ΉΙαΉ╣αΈΛΦ 15310Ά░ε/mm3, C-Έ░αΉζΣΉΕ▒ ΈΜρΈ░▒ ΉΙαΉ╣αΈΛΦ 1.25 mg/dLΉαΑΈΜν. ΉιΕΉΓ░ΊβΦΈΜρΉ╕╡Ή┤υΉαΒΆ▓ΑΉΓυ(CT)ΉΩΡΉΕε ΉλΝΉ╕κ Ά▓╜Έ╢Α(Level III)ΉΩΡ 3.0├Ω2.8├Ω2.3 cmΉζα Ήκ░ΉαΒ ΉοζΆ░ΧΉζ┤ Ήηα ΈΡαΉπΑ ΉΧΛΈΛΦ Έ╢ΑΈ╢ΕΉζΕ ΈΠβΈ░αΊΧε, ΉιΕΈ░αΉιΒΉε╝Έκε Ήκ░ΉαΒ ΉοζΆ░ΧΉζ┤ Ήηα ΈΡαΈΛΦ ΈΜνΈ░εΉΕ▒ Ά▓σΈ▓╜ΉζΕ Ά░ΑΉπΕ ΉλΖΈυ╝Ήζ┤ Ά┤ΑΉ░░ΈΡαΉΩΙΉε╝Έσ░ Ήζ┤Ήβ╕ΉΩΡ ΉΨΣΉ╕κ Ά▓╜Έ╢ΑΉΩΡ ΈΜνΈ░εΉΕ▒Ήζα ΉηΕΊΝΝΉΕι Έ╣ΕΈΝΑΆ░Α Ά┤ΑΉ░░ΈΡαΉΩΙΈΜν(Fig. 1). Ήζ┤ΉΩΡ ΉηΕΊΝΝΉΕι ΈΗΞΉΨΣΉε╝Έκε ΉπΕΈΜρΊΧαΆ│ι ΉΙαΉΙι ΉΜεΊΨΚΊΧαΉαΑΆ│ι ΈΜνΈθΚΉζα ΈΗΞΉζ┤ Έ░░ΉΧκΈΡαΉΩΙΈΜν. Ήκ░ΉπΒ Ά▓ΑΉΓυ Ά▓░Ά│╝ΉΔΒ ΉΩ╝ΉοζΉζΕ ΈΠβΈ░αΊΧε ΈΗΞΉΨΣΉε╝Έκε ΉπΕΈΜρΈΡαΉΩΙΈΜν.
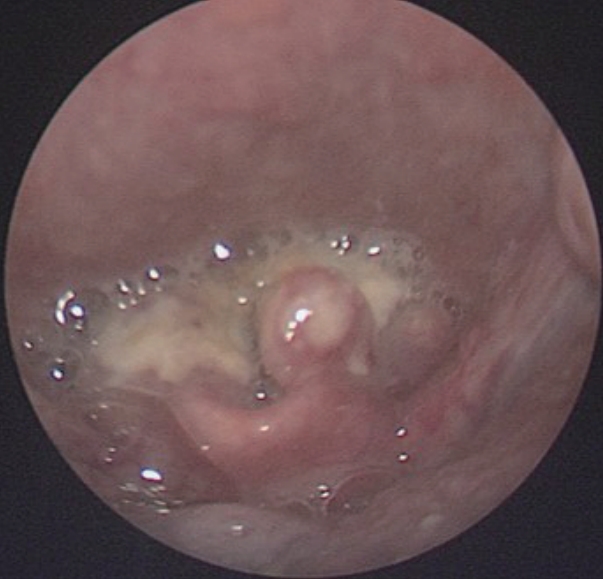
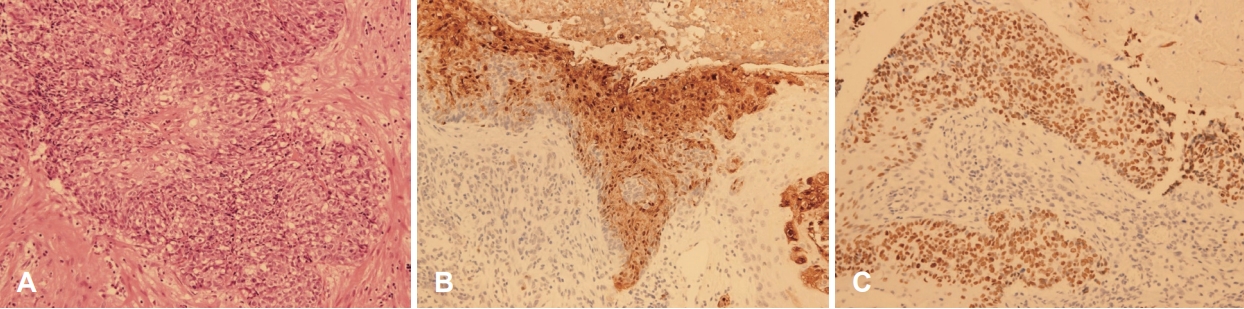
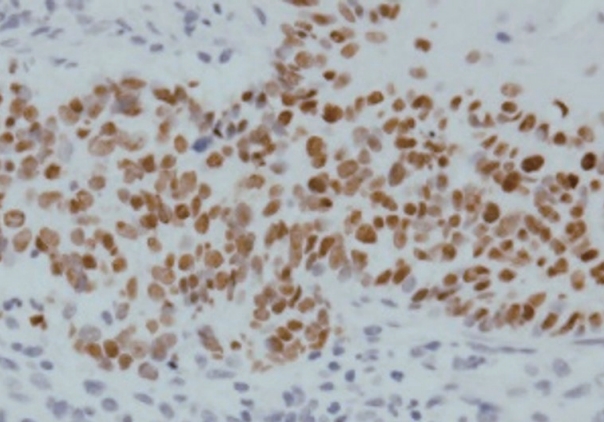
ΊΘ┤ΉδΡ Ήζ┤ΊδΕ Ά▓╜Ά│╝ Ά┤ΑΉ░░ΊΧαΈΞα ΉνΣ ΉΙαΉΙι 1Ά░εΉδΦ ΈΤνΈ╢ΑΊΕ░ Ήγ░Ή╕κ Ά▓╜Έ╢Α ΉλΖΈυ╝Ήζα ΊΒυΆ╕░ ΉοζΆ░ΑΈξ╝ Έ│┤ΉΩυ ΈΜνΉΜε ΉιΕΉΓ░ΊβΦΈΜρΉ╕╡Ή┤υΉαΒ Ά▓ΑΉΓυΈξ╝ ΉΜεΊΨΚΊΧαΉαΑΉε╝Έσ░, Ήζ┤ΉιΕΉζα Ή┤υΉαΒΆ│╝ Έ╣ΕΆ╡ΡΊΧαΉαΑΉζΕ ΈΧΝ Ήγ░Ή╕κΉΩΡ ΉηΙΈΞα ΉηΕΊΝΝΉΕιΈΥνΉζα ΊΒυΆ╕░Ά░Α ΉοζΆ░ΑΊΧαΉαΑΆ│ι ΈΝΑΈ╢ΑΈ╢Ε Έ╢ΑΈ╢Ε Ά┤┤ΉΓυΈξ╝ ΈΠβΈ░αΊΧαΉαΑΈΜν. Ήζ┤ΉβΑ ΊΧρΆ╗α Ήζ┤ΉιΕΉΩΡΈΛΦ Έ│┤Ήζ┤ΉπΑ ΉΧΛΈΞα ΊδΕΈΣΡΉζα ΉλΖΈυ╝Ήζ┤ CTΉΩΡΉΕε Ά┤ΑΉ░░ΈΡαΉΩΙΉε╝Έσ░(Fig. 2), ΊδΕΈΣΡΈΓ┤ΉΜεΆ▓╜ΉΔΒ ΉλΝΉ╕κ ΊδΕΈΣΡ ΉΔΒΈ╢ΑΉΩΡ ΈΣξΆ╖╝ ΈςρΉΨΣΉζα ΉλΖΈυ╝Ήζ┤ ΊβΧΉζ╕ΈΡαΉΩΙΈΜν(Fig. 3). ΊδΕΈΣΡ ΉλΖΈυ╝Ήζα ΉπΕΈΜρΉζΕ ΉεΕΊΧ┤ ΊδΕΈΣΡΈψ╕ΉΕ╕ΉΙαΉΙι Ήκ░ΉπΒΆ▓ΑΉΓυ Έ░Π Ήγ░Ή╕κ Ά▓╜Έ╢Α ΉηΕΊΝΝΉΕι ΉιΙΉιεΉΙιΉζΕ ΉΜεΊΨΚΊΧαΉαΑΉε╝Έσ░ ΊδΕΈΣΡΉΩΡΉΕεΈΛΦ Έ╢ΕΊβΦΆ░Α ΉΧΙ ΉλΜΉζΑ ΊΟ╕ΊΠΚΉΔΒΊΦ╝ΉΕ╕ΊΠυΉΧΦ(squamous cell carcinoma, poorly differentiated), Ά▓╜Έ╢Α ΉηΕΊΝΝΉΕιΉΩΡΉΕεΈΛΦ ΉιΕΉζ┤ΉΕ▒ ΊΟ╕ΊΠΚΉΔΒΊΦ╝ΉΕ╕ΊΠυΉΧΦ ΉΗΝΆ▓υΉζΕ Έ│┤ΉαΑΈΜν. Έσ┤ΉΩφΉκ░ΉπΒΊβΦΊΧβΆ▓ΑΉΓυ Ά▓░Ά│╝ P40Ά│╝ P16ΉΩΡ ΉΨΣΉΕ▒, Epstein-Barr virus (EBV)ΉΩΡ ΉζΝΉΕ▒ Έ░αΉζΣΉζΕ Έ│┤ΉαΑΈΜν(Fig. 4). ΉΙαΉΙι ΊδΕ MRIΉβΑ PET Ά▓ΑΉΓυΈξ╝ ΉΜεΊΨΚΊΧαΉαΑΉε╝Έσ░ ΊδΕΈΣΡ Έ░Π ΉΨΣΉ╕κ Ά▓╜Έ╢ΑΈο╝ΊΦΕΉιΙΉΩΡ hot uptakeΆ░Α Ά┤ΑΉ░░ΈΡαΈΓα ΉδΡΆ▓σ ΉιΕΉζ┤Έξ╝ ΉΜεΉΓυΊΧαΈΛΦ ΉΗΝΆ▓υΉζΑ Ά┤ΑΉ░░ΈΡαΉπΑ ΉΧΛΉΧαΈΜν. Έ│ΣΈουΆ│╝ΉΩΡΉΕε Ή╢ΦΆ░ΑΈκε NUT midline carcinomaΉΩΡ ΈΝΑΊΧε Έ╢ΕΉηΡΈ│ΣΈου Ά▓ΑΉΓυΈξ╝ ΉπΕΊΨΚΊΧαΉαΑΆ│ι NUT positiveΈκε NUT midline carcinomaΈκε ΉπΕΈΜρΈΡαΉΩΙΈΜν(Fig. 5). Ήζ┤ΊδΕ ΊΧφΉΧΦΈ░σΉΓυΉΕι Ή╣αΈμΝΈΛΦ ΊΔΑΈ│ΣΉδΡΉε╝Έκε ΉιΕΉδΡΊΧαΉΩυ ΉπΕΊΨΚΊΧαΉαΑΉε╝Έσ░ 16Ά░εΉδΦ ΈΤν ΉΓυΈπζΊΧαΉαΑΈΜν.
Ά│ι Ή░░
ΉΔΒΈ╢Α Ία╕Ίζκ-ΉΗΝΊβΦΆ╕░ ΉΔΒΊΦ╝ΉΩΡΉΕε Έ░εΉΔζΊΧαΈΛΦ ΈΝΑΈ╢ΑΈ╢ΕΉζα ΉΧΦΉλΖΉζΑ ΊΟ╕ΊΠΚΉΔΒΊΦ╝ΉΧΦΉλΖΉε╝Έκε, conventional typeΉζ┤ΈΓα variant type ΈςρΈΣΡΉΩΡΉΕε ΊζκΉΩ░Ήζ┤ΈΓα ΉζΝΉμ╝Ά░Α Ά┤ΑΈιρΉζ┤ ΉηΙΈΛΦ Ά▓ΔΉε╝Έκε ΉΧΝΈινΉι╕ ΉηΙΈΜν. Έ░ΦΉζ┤ΈθυΉΛνΈΥνΈΠΕ Ήζ┤ΈθυΊΧε ΉΧΖΉΕ▒ΉλΖΉΨΣΉζα Έ░εΉΔζΉΩΡ ΉΩφΊΧιΉζΕ ΊΧαΈΛΦΈΞ░ Ήζ╕Ά░ΕΉειΈΣΡΉλΖΈ░ΦΉζ┤ΈθυΉΛν(human papillomavirus, HPV)ΉβΑ ΉΩκΉΛνΊΔΑΉζ╕-Έ░Φ Έ░ΦΉζ┤ΈθυΉΛν(EBV)Ά░Α Ήζ┤ΉΩΡ ΊΠυΊΧρΈΡεΈΜν. Ά╖╕ΈθυΈΓα Έ│╕ ΉοζΈκΑΉζα ΊβαΉηΡΈΛΦ ΉΗΝΉΧΕΈκε Ήζ┤ΈθυΊΧε ΉεΕΊΩαΉγΦΉζ╕ΈΥνΆ│╝ΈΛΦ Ά┤ΑΆ│ΕΆ░Α ΉΩΗΉΩΙΈΜν. ΈαΡΊΧε Έ░εΈ│Σ ΉΩ░Έι╣ ΈαΡΊΧε 4ΉΕ╕Έκε Ήζ╝Έ░αΉιΒΉζ╕ ΊδΕΈΣΡΉΧΦΉζα Έ░εΈ│Σ ΉΩ░Έι╣Ήζα Έ▓ΦΉεΕΉΩΡΉΕε Έ▓ΩΉΨ┤ΈΓα ΉηΙΈΜν. Ή▓αΉζΝΉΩΡΈΛΦ NMCΆ░Α ΉΗΝΉΧΕ ΈαΡΈΛΦ ΉιΛΉζΑ ΉΕ▒Ήζ╕ΉΩΡΉΕε Έ░εΉΔζΊΧαΈΛΦ Ά▓ΔΉε╝Έκε Ήμ╝Έκε Έ│┤Ά│ιΈΡαΉΩΙΉε╝ΈΓα, Ή╡εΆ╖╝ΉΩΡΈΛΦ NMCΉζα Έ░εΉΔζΉζΑ ΉΕ▒Έ│ΕΉΩΡ ΉΔΒΆ┤ΑΉΩΗΉζ┤ ΉΜιΉΔζΉΧΕΈ╢ΑΊΕ░ 80ΈΝΑΆ╣ΝΉπΑ Ά│ιΈξ┤Ά▓Ν Έ░εΉΔζΈΡαΈΛΦ Ά▓ΔΉε╝Έκε ΉΧΝΈινΉι╕ ΉηΙΈΜν[4]. ΈΣΡΆ▓╜Έ╢Α ΉαΒΉΩφΉζα poorly differentiated Ία╣ΉζΑ undifferentiated carcinomaΈκε ΊβαΉηΡΈΥνΉζα ΉηΕΉΔΒΈ│ΣΈουΊΧβΉιΒ ΊΛ╣ΉΕ▒ Έ░Π NUT expressionΉζΕ Έ╢ΕΉΕζΊΧε ΉΩ░Ά╡υΉΩΡΉΕε, Ή┤ζ 362ΈςΖ ΉνΣ 4ΈςΖ(1.1%)Ήζ┤ NUT-specific monoclonal antibodyΉΩΡΉΕε strong nuclear expressionΉζΕ Έ│┤ΉαΑΉε╝Έσ░, Ήζ┤ΈΛΦ ΈςρΈΣΡ Έ╢ΑΈ╣ΕΈΠβΉΩΡΉΕε Έ░εΉΔζΊΧε ΉλΖΉΨΣΉζ┤ΉΩΙΈΜν. 4ΈςΖ ΉνΣ 1ΈςΖΉζ┤ ΉιΛΉζΑ ΈΓρΉΕ▒(29ΉΕ╕)Ήζ┤ΉΩΙΉε╝Έσ░ ΈΓαΈρ╕ΉπΑΈΛΦ 50-60ΈΝΑΈκε ΊβΧΉζ╕ΈΡαΉΩΙΈΜν[5].
ΊδΕΈΣΡΉΩΡ Έ░εΉΔζΊΧε NMCΈΛΦ Ά╖╣ΊηΙ ΈΥεΈυ╝ΉΨ┤ ΊαΕΉηυΆ╣ΝΉπΑ Έ░εΊΣεΈΡε Ά▓ΔΉζΑ 8ΉαΙΉζ┤Έσ░, Έ│╕ ΈΖ╝Έυ╕Ήζα ΉοζΈκΑ 1Ά▒┤ΉζΕ Ή╢ΦΆ░ΑΊΧαΉΩυ Ήζ┤ΈΥνΉζα ΉηΕΉΔΒΈ│ΣΈουΊΧβΉιΒ ΊΛ╣ΉΕ▒ΉζΕ ΉιΧΈουΊΧαΉαΑΈΜν(Table 1) [4,6-9]. 9ΈςΖ ΉνΣ ΈΓρΉΕ▒Ήζ┤ 5ΈςΖ, ΉΩυΉΕ▒Ήζ┤ 4ΈςΖΉζ┤Έσ░ ΊΠΚΆ╖ι ΉπΕΈΜρ ΉΩ░Έι╣ΉζΑ 29.4ΉΕ╕Ήζ┤ΈΜν. Έ░εΈ│Σ ΉεΕΉ╣αΈΛΦ supraglottisΆ░Α 5ΈςΖΉε╝Έκε Ά░ΑΉηξ ΈπΟΉΧαΈΜν. ΈΝΑΈ╢ΑΈ╢ΕΉζα ΉοζΈκΑΉΩΡΉΕε ΉΙαΉΙιΉζΕ ΉΜεΊΨΚΊΧαΉαΑΉε╝ΈΓα Έ│╕ ΉοζΈκΑΉΩΡΉΕεΈΛΦ Έ│┤Ία╕ΉηΡΉβΑ Ή╣αΈμΝ Έ░σΈ▓ΧΉΩΡ ΈΝΑΊΧε ΉΔΒΈΜ┤ ΊδΕ ΉΙαΉΙιΉζΑ ΉΜεΊΨΚΊΧαΉπΑ ΉΧΛΆ╕░Έκε Ά▓░ΉιΧΊΧαΉαΑΈΜν.
ΈΣΡΆ▓╜Έ╢ΑΉλΖΉΨΣΉΩΡΉΕε NMCΈΛΦ ΈπνΉγ░ ΈΥεΈυ╝Ά▓Ν Έ░εΉΔζΊΧαΉπΑΈπΝ ΉΔΒΈ╢Α ΉΗΝΊβΦ-Ία╕ΊζκΆ╕░Ά│ΕΈΓα Έ╢ΑΈ╣ΕΈΠβΉζα poorly differentiated Ία╣ΉζΑ undifferentiated carcinomaΈκε ΉλΒΊηΝΈΜνΈσ┤ Έυ┤ΉΜεΊΧι ΉΙα ΉΩΗΈΛΦ ΉΙαΉνΑΉζα ΉειΈ│ΣΈξιΉζΕ Έ│┤Ήζ┤ΈψΑΈκε, ΉζαΉΜυΉζ┤ ΈΡαΈΛΦ Ά▓╜Ήγ░ΉΩΡΈΛΦ NUTΉΩΡ ΈΝΑΊΧε immunohistochemistry (NUT IHC)Έξ╝ ΉΜεΊΨΚΊΧαΈΛΦ Ά▓ΔΉζ┤ Έ░ΦΈηΝΉπΒΊΧι Ά▓ΔΉζ┤ΈΜν[5]. Ή╡εΆ╖╝ΉΩΡΈΛΦ ΈςρΈΥι poorly differentiated non-cutaneous carcinomasΉΩΡΉΕε squamous differentiationΉζα ΉειΈυ┤ΉΩΡ ΉΔΒΆ┤Α ΉΩΗΉζ┤ NMCΉζα Ά░ΑΈΛξΉΕ▒ΉζΕ Έ░░ΉιεΊΧαΆ╕░ ΉεΕΊΧαΉΩυ NUT IHCΈξ╝ ΉΜεΊΨΚΊΧαΈΛΦ Ά▓ΔΉζΕ Ά╢ΝΆ│ιΊΧαΆ╕░ΈΠΕ ΊΧεΈΜν[10]. ΈαΡΊΧε ΈΓαΉζ┤ΉβΑ ΊζκΉΩ░ΉειΈυ┤ΈΛΦ NMCΉζα Ά░ΑΈΛξΉΕ▒ΉζΕ Έ░░ΉιεΊΧαΈΛΦΈΞ░ ΉΓυΉγσΈΡαΉΨ┤ΉΕεΈΛΦ ΉΧΙΈΡαΈσ░, glandular differentiationΉζΕ Έ│┤Ήζ┤ΈΛΦ ΉλΖΉΨΣΆ│╝ HPVΉβΑ EBVΉβΑ Ά░βΉζΑ viral etiologyΈΛΦ NMCΉβΑ Ά┤ΑΈιρΉζ┤ ΉΩΗΉε╝ΈψΑΈκε Έ░░Ήιε ΉπΕΈΜρΉΩΡ Ήζ┤ΉγσΊΧι ΉΙα ΉηΙΈΜνΈΛΦ ΉΩ░Ά╡υΆ▓░Ά│╝ΈΠΕ ΉηΙΈΜν[10].
NMCΉζα ΉπΕΈΜρΉζΑ ΊΧ╡ΊαΧ Έ╢ΕΉΕζΉζΕ ΊΗ╡ΊΧ┤ t(15;19) ΉηυΈ░░ΉΩ┤ΉζΕ Έ│┤ΉΩυΉμ╝ΈΛΦ Ά▓ΔΉε╝Έκε Ή╢σΈ╢ΕΊΧαΉπΑΈπΝ, NUT Έ░Π BRD4 ΉειΉιΕΉηΡΉΩΡ ΈΝΑΊΧε fluorescence in situ hybridization Ά▓ΑΉΓυΈΠΕ Ά░εΈ░εΈΡαΉΨ┤ ΉηΙΈΜν[11]. Ή╡εΆ╖╝ ΉΩ░Ά╡υΉΩΡΉΕε ΉΚ╜Ά▓Ν ΉΓυΉγσΊΧι ΉΙα ΉηΙΈΛΦ ΉπΕΈΜρ Ά▓ΑΉΓυΈξ╝ Ά░εΈ░εΊΧαΆ╕░ ΉεΕΊΧ┤ NUTΉΩΡ ΈΝΑΊΧε ΈΜρΉζ╝ ΊΧφΉ▓┤Έξ╝ ΉΔζΉΓ░ΊΨΙΆ│ι, Ήζ┤Ά▓ΔΉζ┤ IHCΉΩΡ ΉζαΊΧ┤ NUT Έ░εΊαΕΉζΕ Ά░ΡΉπΑΊΧαΈΛΦ Ά▓ΔΉζΕ ΊβΧΉζ╕ΊΧαΉαΑΈΜν. ΈΝΑΉκ░ Ήκ░ΉπΒΉζΕ ΊΠυΊΧρΊΧε ΉΩ░Ά╡υΉΩΡΉΕε NUT ΈΜρΉζ╝ ΊΧφΉ▓┤ΈΛΦ NMCΉζα ΉπΕΈΜρΉΩΡ ΉηΙΉΨ┤ 100%Ήζα ΊΛ╣Ήζ┤ΈΠΕΉβΑ 87%Ήζα Έψ╝Ά░ΡΈΠΕΈξ╝ Ά░ΑΉπΑΈΛΦ Ά▓ΔΉε╝Έκε ΊβΧΉζ╕ΈΡαΉΩΙΈΜν[12].
NMCΉζα Ή╣αΈμΝΉΩΡ ΉηΙΉΨ┤, ΉΧΕΉπΒΆ╣ΝΉπΑ ΊΣεΉνΑ Ή╣αΈμΝΈ▓ΧΉΩΡ ΈΝΑΊΧε consensusΈΛΦ ΉΩΗΉε╝Έσ░ ΊΧφΉΧΦΊβΦΊΧβΉγΦΈ▓Χ, Έ░σΉΓυΉΕιΉγΦΈ▓Χ, ΉΙαΉΙιΉζΕ ΊΠυΊΧρΊΧαΈΛΦ ΈΜνΉνΣ ΉιΣΆ╖╝Έ▓ΧΉζ┤ ΉηΕΉΔΒΉιΒΉε╝Έκε ΉΓυΉγσΈΡαΆ│ι ΉηΙΈΜν. ΉΙαΉΙιΉζ┤ Ά░ΑΈΛξΊΧε ΉΔΒΊβσΉζ┤Έζ╝Έσ┤ ΉΙαΉΙιΉζΕ ΉΜεΊΨΚΊΧαΈΛΦ Ά▓ΔΉζ┤ ΉαΙΊδΕΉΩΡ Ά╕ΞΉιΧΉιΒΉζ╕ ΉαΒΊΨξΉζΕ Έψ╕Ή╣αΈΛΦΈΞ░, 40ΈςΖΉζα ΈΣΡΆ▓╜Έ╢Α NMC ΊβαΉηΡΆ╡░ΉζΕ ΊΠυΊΧρΊΧε ΉΩ░Ά╡υΉΩΡΉΕε 2ΈΖΕ ΉΔζΉκ┤ΉερΉζΑ 30%ΉαΑΉε╝Έσ░, Ή┤ΙΆ╕░ΉΩΡ Ά╖╝Ή╣αΉιΒ ΉιΙΉιεΉΙιΉζΕ ΉΜεΊΨΚΊΧαΆ│ι Έ│┤Ήκ░ ΊΧφΉΧΦΈ░σΉΓυΉΕιΉγΦΈ▓ΧΉζΕ ΉΜεΊΨΚ Έ░δΉζΑ 3ΈςΖΉζ┤ Ά░ΒΆ░Β 35, 72, 78Ά░εΉδΦ ΉΔζΉκ┤ΊΧρΉε╝ΈκεΉΕε ΉηξΆ╕░ ΉΔζΉκ┤ΉηΡΆ░Α ΈΡαΉΩΙΈΜν[13]. Cisplatin, taxanes, alkylating agentΈξ╝ Ήζ┤ΉγσΊΧε ΊΧφΉΧΦΈ░σΉΓυΉΕι Έ│╡ΊΧσΉγΦΈ▓ΧΉζ┤ Ή▓αΉζΝΉΩΡΈΛΦ Έ░αΉζΣΉζ┤ ΉηΙΉε╝ΈΓα ΈΝΑΈ╢ΑΈ╢ΕΉζα Ά▓╜Ήγ░ΉΩΡΉΕε ΉηυΈ░εΊΧαΈσ░ Ά╖╕ Ήζ┤ΊδΕΉζα Ή╣αΈμΝΉΩΡΈΛΦ Έ░αΉζΣΉζ┤ ΉλΜΉπΑ ΉΧΛΉζΑ Ά▓ΔΉε╝Έκε ΉΧΝΈινΉι╕ ΉηΙΈΜν[14,15]. Ή╡εΆ╖╝ uniform ΊΧε ΉειΉιΕΉιΒ Έ│ΑΉζ┤Έξ╝ Έ░ΦΊΔΧΉε╝Έκε ΊΧε targeted therapyΆ░Α ΉΗΝΆ░εΈΡαΆ│ι ΉηΙΈΜν. BRD-NUT fusion protein sequenceΈΛΦ ΊΟ╕ΊΠΚΉΕ╕ΊΠυΈκεΉζα Έ╢ΕΊβΦΈξ╝ ΈπΚΈΛΦ Ά▓ΔΉε╝Έκε ΉΧΝΈινΉι╕ ΉηΙΆ│ι, Ήζ┤ΉΩΡ ΈΦ░Έζ╝ BRD-NUTΈξ╝ ΉΨ╡ΉιεΊΧαΈσ┤ ΊΟ╕ΊΠΚΉΕ╕ΊΠυ Έ╢ΕΊβΦΆ░Α ΉειΈΠΕΈΡαΈσ░, Ά▓░Ά╡φ ΉλΖΉΨΣ ΉΕ╕ΊΠυΈΥνΉζΑ ΉΕ▒ΉηξΉζΕ ΈσΙΉ╢ΦΆ│ι Ίε┤Έσ┤ ΉΔΒΊΔεΉζα ΊΟ╕ΊΠΚΉΕ╕ΊΠυΈκε Έ╢ΕΊβΦΈΡαΆ▓Ν ΈΡεΈΜν. Ήζ┤ΈθυΊΧε Έ░εΆ▓υΉζ┤ ΉΔΙΈκεΉγ┤ Ή╣αΈμΝΉζα Ά░ΑΈΛξΉΕ▒ΉζΕ ΉΩ┤ΉΩΙΆ│ι bromodomain and extraterminalmotif inhibitorΉβΑ histone deacetylase inhibitorsΆ░Α ΊαΕΉηυ Ήζ┤ΉγσΈΡαΆ│ι ΉηΙΈΜν[5].
Έ│╕ ΉοζΈκΑΈΛΦ 4ΉΕ╕ ΉΗΝΉΧΕΉΩΡΉΕε NMCΆ░Α ΊδΕΈΣΡΉΩΡ Έ░εΉΔζΊΧαΉΩυ Ά▓╜Έ╢Α Έο╝ΊΦΕΉιΙ ΉιΕΉζ┤Ά░Α ΈΡε Ήζ┤ΊδΕ Έ░εΆ▓υΈΡε ΈΥεΈυ╕ ΉοζΈκΑΉζ┤ΈΜν. NMCΉζα ΈΓχΉζΑ ΉειΈ│ΣΈξι Έ░Π Έ╣ΕΊΛ╣Ήζ┤ΉιΒΉζ╕ ΉηΕΉΔΒΉΨΣΉΔΒΉζΕ Ά│ιΈινΊΧ┤ Έ│┤ΉΧαΉζΕ ΈΧΝ, Ά░ΡΈ│ΕΉπΕΈΜρΉε╝Έκε NMCΈξ╝ ΉΔζΆ░ΒΊΧαΈΛΦ Ά▓ΔΆ│╝ Ήζ╝Έ░αΉιΒΉε╝Έκε ΉΜεΊΨΚΊΧαΈΛΦ Έ│ΣΈουΉκ░ΉπΒΊΧβΉιΒ Ά▓ΑΉΓυ Ά▓░Ά│╝Έξ╝ ΊΗ╡ΊΧ┤ΉΕε NMCΈξ╝ ΉπΕΈΜρΊΧαΈΛΦ Ά▓ΔΉζΑ ΉΨ┤ΈινΉγ┤ Ήζ╝Ήζ┤ΈΜν. Έ│╕ ΉοζΈκΑΈξ╝ ΊΗ╡ΊΧ┤ΉΕε ΊδΕΈΣΡ Έ░Π ΈΣΡΆ▓╜Έ╢ΑΉΩΡ Έ░εΉΔζΊΧαΈΛΦ ΊΟ╕ΊΠΚΉΕ╕ΊΠυΉΧΦΉλΖ Έ░Π Έψ╕Έ╢ΕΊβΦΉΧΦΉλΖΉζα Ά▓╜Ήγ░ΉΩΡ NUT Έσ┤ΉΩφΉκ░ΉπΒΊβΦΊΧβΆ▓ΑΉΓυΈξ╝ ΉΜεΊΨΚΊΧαΈΛΦ Ά▓ΔΉζ┤ ΉζαΈψ╕Ά░Α ΉηΙΉζΝΉζΕ ΉΧΝ ΉΙα ΉηΙΈΜν.