서 론
급성 골수성 백혈병(acute myeloid leukemia)의 10%-15%를 차지하는 급성 전골수성 백혈병(acute promyelocytic leukemia, APL)은 15번과 17번 염색체의 전좌로 인한 promyelocytic leukemia (PML) 및 retinoic acid receptor alpha (RARA) 유전자의 결합으로 생성되는 단백질이 정상적인 골수 세포의 분화를 막아 발생한다[1]. 급성 전골수성 백혈병은 임상적으로는 출혈 경향성과 빠른 경과의 악화를, 혈액 검사에서는 Auer rod를 가지는 전골수세포가 보이는 것이 특징적이다[1]. 급성 전골수성 백혈병의 예후는 1980년대 후반 all-trans retinoic acid (ATRA)와 1990년대 후반 arsenic trioxide (ATO)의 도입 이후 급격히 향상되었다[2]. 하지만 발전된 치료에도 불구하고 5%-10% 환자들에서 재발한다고 알려져 있으며 대부분 첫 3년 이내에 발생한다[1]. 급성 전골수성 백혈병에서 골수 외 재발은 3%-5%로 보고 될 정도로 드물고, 가장 흔한 발생 위치는 첫 번째가 중추신경계이며 두 번째가 피부고[3], 외이도와 측두골에서 재발한 경우는 드물게 보고되고 있다.
저자들은 5년 전 급성 전골수성 백혈병 진단 이후 치료에도 불구하고 2차례의 재발 및 치료 이후 발생한 골수형성이 상증후군으로 혈액종양내과에 입원한 환자에서 이통 및 청력저하를 일으킨 우측 외이도 및 측두골의 병변에서 급성 전골수성 백혈병의 세 번째 재발 및 골수 외 침범을 확인한 1예를 경험하였고, 이를 공유하고자 보고하는 바이다.
증 례
고혈압, 당뇨의 기저질환이 있는 69세 남자가 급성 전골수성 백혈병 치료 이후 발생한 골수형성 이상증후군에 대해 본원 혈액종양내과에 입원 중 1주일 전부터 시작된 우측 이통, 청력저하로 이비인후과에 협진 의뢰되었다.
5년 전 발열에 대해 시행한 혈액검사에서 범혈구감소증 소견을 보여 골수검사 및 fluorescence in-situ hybridization 검사를 하였으며 t(15;17), PML/RARA 99.3%로 급성 전골수성 백혈병으로 진단되었다. 이에 본원 혈액종양내과에서 idarubicin 및 ATRA의 관해유도 및 3차례 공고요법 후 완전관해 판정을 받았으며 이후 ATRA 복용하며 유지요법 시행하였다. 재발 없이 추적 관찰 하던 중 2년 전 골수검사에서 재발이 확인되어 ATO로 관해유도 및 2차례 공고요법을 시행 받았으며, 1년 전 골수검사상 두 번째 재발이 확인되어 idarubicin 및 ATRA로 관해유도 및 1차례 공고요법을 시행 후 여동생으로부터 동종 말초혈액 조혈모세포 이식을 받았다. 상기 치료 6개월 뒤 시행한 골수검사에서 5%-10%의 골수아세포 소견을 보여 골수형성이상증후군이 확인되어 금번 입원하였다.
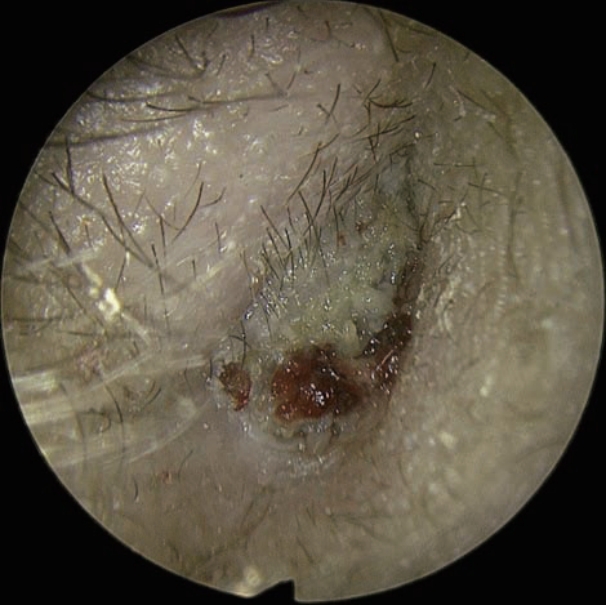
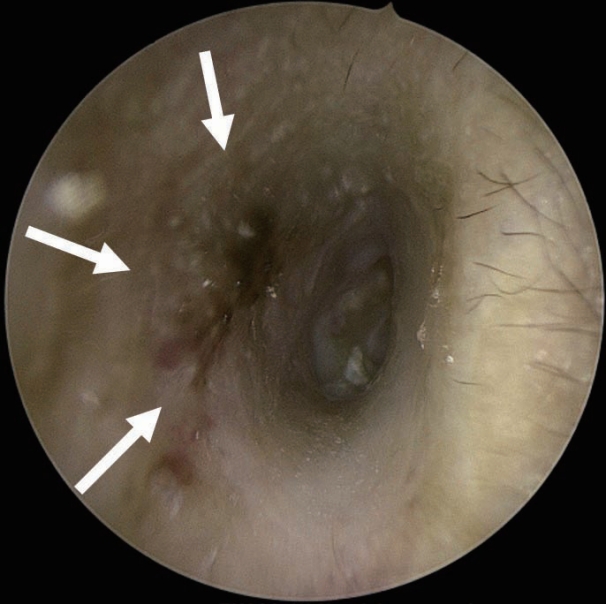
문진에서 우측 이통 및 청력저하를 호소하였으며 이충만감과 어지럼은 없었다. 내시경에서는 우측 외이도의 후방에서 기원한 종물이 확인되었으며 표면은 불규칙하였고 만졌을 때 쉽게 출혈되는 양상을 보였다(Fig. 1). 이로 인해 고막은 관찰할 수 없었다. 반대측의 귀에는 특이소견을 보이지 않았다.
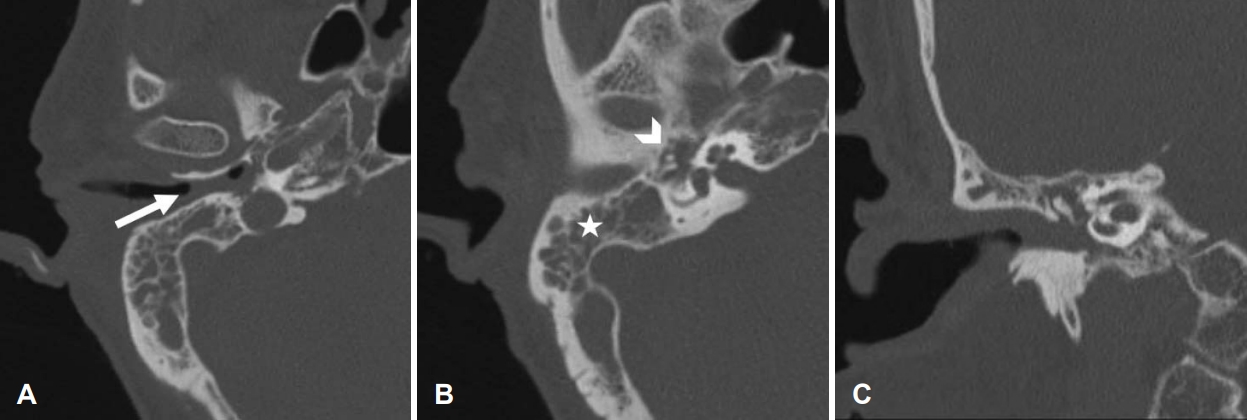
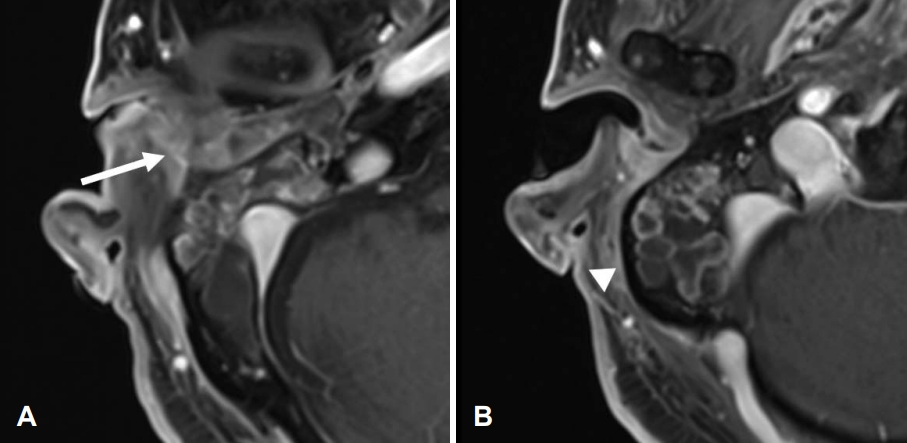
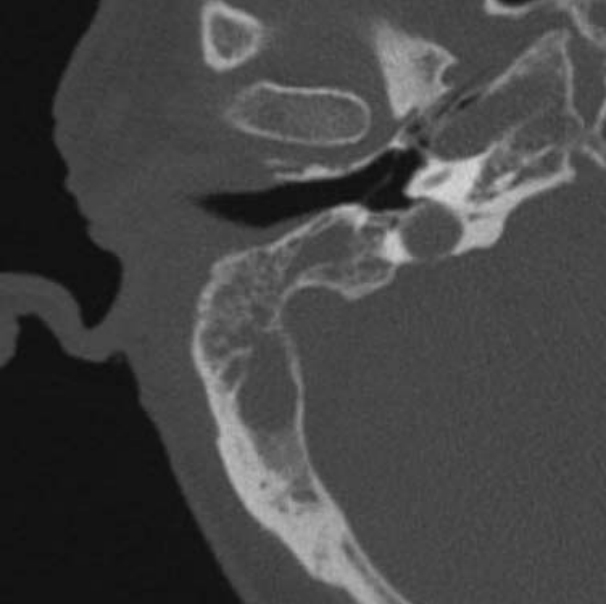
순음청력검사에서 우측 기도청력 88 dB, 골도청력 52 dB로 기도-골도차가 36 dB로 확인되었다. 고막 운동성 검사에서는 우측 B형이 확인되었다. 측두골 전산화단층촬영검사에서 우측 외이도 후벽, 중이, 유양동에 광범위한 연부조직 음영이 확인되며 주변 골미란은 동반되지 않았다(Fig. 2). T1 강조 측두골 자기공명영상검사에서도 마찬가지로 우측 외이도 후벽, 중이 및 유양동의 전반적인 조영증강 되는 연부조직 음영이 확인되었다(Fig. 3). 이에 대해 외이도 후벽의 종양 의심 하에 국소마취하 절제 생검을 시행하였다.
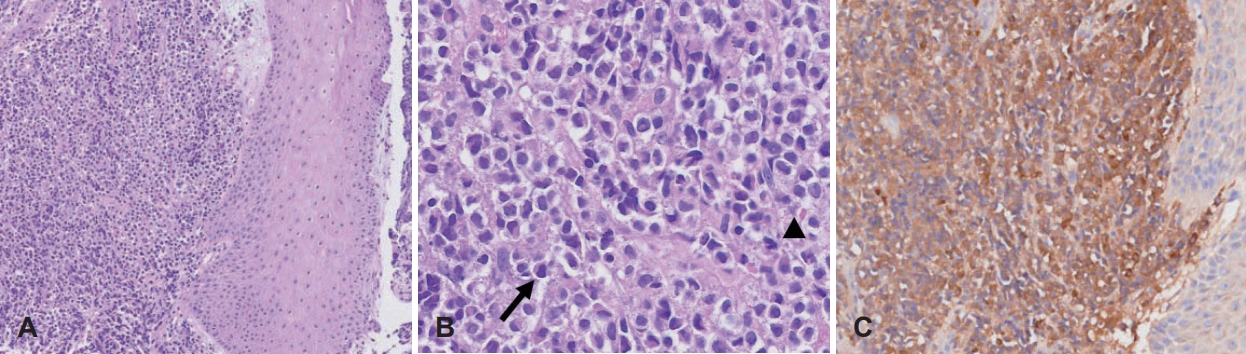
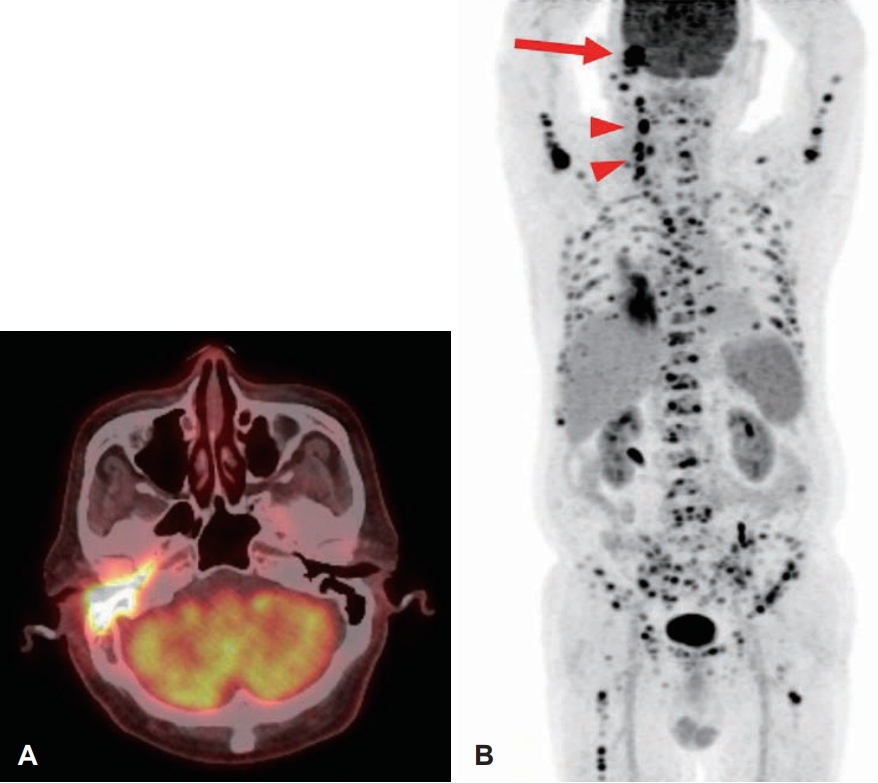
조직검사에서 광학 현미경 저배율(×100)상 외이도 진피 내로 염색질이 진한 세포들의 침윤이 관찰되며 고배율(×400)에서는 다양한 형태의 핵을 가지는 세포들이 관찰되었다. 세포 화학염색에서 myeloperoxidase 염색에 양성을 보였으며, 기존에 급성 전골수성 백혈병의 병력을 가지고 있는 점을 종합하여 보았을 때 백혈병 전골수아세포의 외이도 침윤으로 확인되었다(Fig. 4). 조직검사 결과 급성 전골수성 백혈병의 세번째 재발로 진단되었으며 골수 외 침범이 확인되어 양전자 방출 단층촬영검사를 시행하였고, 우측 외이도와 측두골 외에도 우측 경부 림프절의 골수 외 침범이 확인되었다(Fig. 5). 이에 대해 완화적 목적으로 ATRA와 ATO를 통해 관해유도 및 공고요법을 시행하기로 하였다.
고 찰
급성 골수성 백혈병에서 골수 외 침범은 10% 미만의 환자들에서 발생할 정도로 드물고 주로 French-American-British 분류상 M4, M5형에서 잘 생기며 중추신경계, 피부, 림프절 순으로 발생한다고 알려져 있다[4]. 이러한 골수 외 침범은 처음 질병이 생길 때 발생하는 것은 드물며, 대부분 재발하는 경우에 생기고 예후가 불량한 것으로 알려져 있다[5,6]. 이전 연구에 따르면 외이도를 침범하는 경우는 매우 적으며[7], 국내에서도 외이도 및 측두골을 침범한 보고는 드문 것으로 확인된다.
급성 전골수성 백혈병의 치료에는 다른 급성 골수성 백혈병의 치료와는 달리 vitamin A의 유사체인 ATRA를 사용한다[8]. 급성 전골수성 백혈병에서 PML/RARA fusion protein이 골수 세포의 분화를 막는데 ATRA가 이를 억제하여 정상적인 골수 세포의 분화를 유도하고 백혈병 세포의 사멸을 일으킨다[8]. 기존 급성 골수성 백혈병의 치료와 같이 항암치료만을 사용하였을 때는 완전관해율이 70%에 불과하였으나, 1986년 ATRA 치료가 도입된 이후 항암치료와 병행하는 요법을 통해 완전관해율이 90%-95%로 급격히 향상되었다[8]. 하지만 이러한 치료 효과와는 상반되게 ATRA 사용 이후 급성 전골수성 백혈병의 골수 외 침범이 더 많이 보고되고 있다고 한다[3,4,7]. 이에 대한 명확한 기전은 아직 밝혀지지 않았으나, 두 가지 가능한 가설들이 제시되었다. 첫 번째는 ATRA 도입 이후 생존율이 증가해 골수 외 침범의 빈도가 높아졌다는 것이다[3]. 두 번째는 ATRA 사용시 intercellular adhesion molecule-1, leukocyte adherence protein B (CD18)과 같은 부착인자의 발현 증가로 인해 피부, 림프절과 같은 골수 외 장기에 백혈병 세포들의 침윤이 증가하여 생긴다는 것이다[9]. 하지만 다른 연구에서는 ATRA 사용이 골수 외 재발의 위험성을 증가시키지 않는다는 보고도 있어[10] 이에 대해 추가적인 연구가 필요해 보인다. 이 외에도 골수 외 침범의 위험인자로 젊은 연령, 백혈구증가증, bcr3 PML/RARA 재배열이 제시되었다[11].
ATO의 명확한 기전은 밝혀지지 않았으나 ATO가 ubiquitin-proteasome pathway를 통해 PML/RARA fusion protein을 분해하여 치료 효과가 있다고 알려져 있다[12]. 급성 전골수성 백혈병의 골수 재발의 경우 ATO를 통한 치료가 효과적이라고 알려져 있으나[1], 골수 외 침범의 경우에는 아직까지 효과적인 치료에 대한 연구가 없다[4]. 하지만 ATO가 손톱, 머리카락, 피부와 같은 표피 조직에 잘 침착된다는 점을 통해 이러한 표피 조직의 골수 외 재발일 경우에는 치료 효과가 있을 것으로 예측된다[4]. 이외에도 방사선치료, 전신적 항암치료가 고려될 수 있으며 최근에는 ATRA보다 10배 효력이 있는 tamibarotene의 사용도 연구되고 있다[3].
본 증례에서는 이통, 청력저하를 일으킨 외이도 및 측두골에 생긴 급성 전골수성 백혈병의 골수 외 재발을 ATRA 및 ATO 병합요법을 통해 효과적으로 치료하였다. 급성 전골수성 백혈병의 과거력이 있는 환자에서 이통, 청력저하와 같은 이과적 증상을 호소하며 귀에 종양성 병변이 확인된다면 급성 전골수성 백혈병이 귀에 침범한 골수 외 재발일 가능성을 염두에 두고 조기에 조직검사를 통한 진단 및 치료가 필요할 것이라 생각된다.