개방동 유양돌기 절제술에서 탈회된 골기질을 이용한 유양동성형술의 안정성 및 유용성 검증: 탐색적 연구
Safety and Efficacy of Mastoidoplasty With Demineralized Bone Matrix in Canal Wall Down Mastoidectomy: A Pilot Study
Article information

Trans Abstract
Background and Objectives
The canal wall down mastoidectomy brings changes in the anatomy of the external auditory canal (EAC), causing potential problems, such as accumulated crust, vertigo attacks, and difficulties in wearing hearing aids (HAs). The objective of this study is to evaluate the safety and efficacy of mastoidoplasty using the demineralized bone matrix (DBM) to obliterate the mastoidectomized cavity and reconstruct EAC.
Subjects and Method
Medical records of patients with chronic otitis media with or without cholesteatoma who received mastoidoplasty using DBM by a single surgeon at Seoul St. Mary’s hospital between 2014 and 2021 were reviewed retrospectively.
Results
A total of 27 patients were included in this study. None of the patients showed any recurrence of cavity problem, wound infection, or any other complications during their follow-up period of 13.07±37 months. The average air and bone conduction hearing level of pure tone audiometry showed no significant change after surgery (p=0.50, p=0.54, respectively). Five patients indicated for hearing rehabilitation could adopt canal type HAs after surgery; six patients used completely-in-the canal type HAs, and one patient used in-the-canal type HAs. None of the patients using HAs complained of acoustic feedback or any other problem in wearing HAs.
Conclusion
Mastoidoplasty using DBM seems to be a very safe and effective surgical procedure that shows functionally acceptable EAC for hearing rehabilitation with canal type HAs and demonstrates no specific complication.
서 론
유양돌기절제술의 목적은 병변의 제거와 중이강의 해부학적 구조를 재건하는 것이다. 개방동 유양돌기절제술(canal wall down mastoidectomy, CWDM)은 폐쇄동 유양돌기절제술(canal wall up mastoidectomy)보다 잔존하는 진주종을 발견하기 쉽고 재발률을 낮출 수 있다는 장점이 있다[1-3]. 하지만 CWDM은 외이도의 생리학적 구조 유지에 어려움이 있고 공동 문제를 야기할 수 있다는 문제가 존재하며, 보청기 착용의 문제, 온도와 압력 변화로 인한 어지럼 등의 문제를 동반한다[4]. CWDM 후 발생하는 문제를 보완하기 위해 외이도의 후벽을 재건하거나 유양동을 폐쇄하는 여러 술식이 보고되었으며, 주로 근육, 골막, 연골, 골분, 지방, hydroxyapatite 등을 이용한 방법이 있다[5-10]. 국소 피판을 사용한 경우 일부에서 공동을 완전히 메우지는 못하여 수술 후 결손이 발생하며, 유리 피판을 사용하였을 때는 치유 기간이 길고 염증이 관찰되는 경우가 존재하였다[11].
탈회된 골기질(demineralized bone matrix, DBM) (Grafton Putty, 2.5 cc; Medtronic, Memphis, TN, USA)은 동종이식 골의 항원성을 낮추기 위해 탈회 과정을 거친 골 충전재로, 골 형성 단백질(bone morphogenic protein)을 활성화시켜 골전도 및 골유도현상을 야기하여 결손 부위를 보강하는 데 사용되고 있다[12].
본 저자는 DBM을 이용하여 외이도 변형과 공동 문제를 보완하는 새로운 유양동성형술(mastoidoplasty)을 고안하여 CWDM 환자에게 적용하였고, 본 연구에서 DBM을 이용한 유양동성형술의 효과와 안전성을 평가하여 보고하고자 한다.
대상 및 방법
대 상
2014년 4월부터 2021년 4월까지 서울성모병원에서 1명의 술자(S.N.P.)에게 DBM을 이용한 유양동성형술을 시행 받은 27명의 환자를 대상으로 후향적 연구를 시행하였고, 서울성모병원 임상시험심사위원회(Institutional Review Board, IRB)의 승인 후 진행되었다(IRB No. KC19RESI0772). 27명의 환자 중 최초 수술로 CWDM와 DBM을 이용한 유양동성형술을 동시에 시행한 환자는 6명이었고, 이전 수술 후 재수술한 경우는 21명이었다. 남자가 8명, 여자가 22명이었고 환자의 평균 연령은 58.63±10.14세, 평균 추적 관찰 기간은 10.30±15.32개월이었다. 병리 소견상 진주종성 중이염이 확인된 경우가 12예, 비진주종성 중이염이 15예였다. 각 환자에 대한 임상 소견은 Table 1에 기술하였다.

Summary of the patients who underwent mastoidoplasty with DBM
수술 방법 및 안전성, 유효성 검증
모든 환자는 교신 저자에게 수술을 시행 받았다. 수술 방법은 전신마취하에 후이개 피부에 절개선을 넣고 피판을 올렸다. 측두근막을 통상적인 방법으로 채취한 뒤 L자 형태로 후골막을 절개하여 하부 기반 골막 피판(inferiorly based periosteal flap)을 얻었다. 고실성형술 및 개방형 유양돌기절제술을 시행하여 중이강과 유양동의 병변을 제거하였다. 이후 유양동성형술을 위해 하부 기반 골막 피판의 전방 경계에 절개를 하여 전방의 후이개 연조직 피판과 분리시켜 하부 기반의 길쭉한 피판을 만들고(Fig. 1A), 이 피판의 첨단을 상고실부에 넣어 유양동의 일부를 폐쇄하고 후방 외이도의 윤곽을 만들었다(Fig. 1B). 후방 외이도 윤곽을 유지시키고 강화하기 위해 흡수성 봉합사를 이용하여 위치된 피판의 상부와 하부를 전방의 후이개 연조직 피판에 봉합하였다(Fig. 1C). 이후 피판 뒤쪽으로 남은 유양동 공동의 용적을 생리식염수를 이용하여 측정하였다. 남은 유양동 공동에 들어가는 생리식염수의 양을 측정하여 그 양만큼 DBM을 넣어 유양동을 완전히 폐쇄하였다(Fig. 1D). 골막 피판의 앞쪽 남아있는 고실외이도 피판의 피부 사이에 측두근막을 추가로 삽입하고 외이도 크기와 모양을 최대한 정상에 가깝게 성형함으로써 유양동 성형술을 완료하고 외이도 팩킹을 하였고, 후이개 피부를 봉합한 후 수술을 마쳤다.
Intraoperative photo of mastoidoplasty with DBM after CWDM. A: Incision was made in the anterior edge of the inferior based periosteal flap to make a longitudinal inferior based flap with an apex (black arrow). B: The apex of the inferior based periosteal flap (black arrow) was rotated so that the length of the flap (white arrow) can reconstruct posterior EAC and the apex can obliterate the epitympanum. C: The inferior based periosteal flap was sutured inferiorly and superiorly with vicryl 3-0 to the anterior soft tissue flap to maintain the shape of EAC reconstruction. D: DBM (asterisk) was inserted posterior to the inferior based periosteal flap (white arrow) to completely obliterate the mastoid cavity. DBM, demineralized bone matrix; CWDM, canal wall down mastoidectomy; EAC, external auditory canal.
이소골성형술이 필요한 경우 수술 중 소견을 고려하여 동시 또는 단계적 수술(staged ossiculoplasty)을 결정하였다. 본 연구에서 일차 수술로 이소골성형술을 동시에 시행한 경우는 18예, 계획된 이차 수술로 이소골성형술을 시행한 경우는 4예, 이소골성형술을 시행하지 않은 경우는 5예였다.
본 술식의 안전성과 유효성을 확인하고자 모든 환자의 외래 방문시 이내시경을 이용하여 수술 부위를 관찰 및 기록하였고, 양안 현미경으로 고막 및 외이도를 관찰하고 순음청력검사를 시행하였다. 공동 문제, 술후 이루 등의 합병증과 수술 전, 후 기도-골도 청력 차이, 술후 청력 개선 여부에 대해 조사하였고 술후 보청기를 활용한 청각 재활 시의 순응도를 확인해 보았다. 순음청력검사 중 기도 청력 결과는 1995년 ‘The Guidelines of the Committee on Hearing and Equilibrium of the AAO & HNS’ 기준에 따라 기도 순음청력역치를 500 Hz, 1 kHz, 2 kHz, 3 kHz의 산술평균으로 하였다.
통계 분석은 SPSS software (ver. 24.0; IBM Corp., Armonk, NY, USA) 이용하였고, p-value가 0.05 미만인 경우 통계학적으로 유의한 것으로 간주하였다. 각 자료의 평균은 중앙값과 표준편차로 표기하였다.
결 과
DBM을 이용한 유양동성형술 이후 평균 14개월 이상의 추적 관찰 기간 동안 수술을 받은 27명의 환자 모두에게서 술후 감염, 후이개부 염증 또는 피부 함몰, 유양동과 피부 간의 루 등의 합병증은 관찰되지 않았고 외이도의 형태가 비교적 잘 유지되었다(Fig. 2). 추적 관찰 중 3예에서 시행한 측두골 단층촬영에서도 외이도 변형을 유발할 만한 DBM의 손실은 관찰되지 않았고 외이도의 형태 및 유양동 폐쇄는 비교적 잘 유지됨을 확인하였으며, 결과적으로 술후 공동 문제를 호소한 환자는 없었다(Fig. 3).

Postoperative endoscopic findings of the patients who received mastoidoplasty with DBM. A: A 57-year-old female after revision Lt. CWDM and mastoidoplasty with DBM. B: A 49-year-old female after revision Rt. CWDM and mastoidoplasty with DBM. C: A 48-year-old female after Rt. CWDM and mastoidoplasty with DBM, ossiculoplasty. D: A 74-year-old female after Rt. CWDM and mastoidoplasty with DBM, ossiculoplasty. DBM, demineralized bone matrix; CWDM, canal wall down mastoidectomy.
CT scans of the mastoid cavity before and after mastoidoplasty with DBM. A: Huge mastoidectomized cavity after previous CWDM and before mastoidoplasty with DBM. B: One year after mastoidoplasty with DBM showing reconstructed EAC with minimized mastoid cavity. DBM, demineralized bone matrix; EAC, external auditory canal.
수술 전 평균 골도역치는 36.53±21.94 dB였고 수술 후 평균 골도역치는 36.85±21.48 dB로, 유의미한 통계학적 차이는 없었다(p=0.54). 수술 전 평균 순음청력역치와 기도-골도 청력 차이는 각각 58.61±21.36 dB와 22.08±14.37 dB였다. 수술 후 평균 순음청력역치와 기도-골도 청력 차이는 각각 55.37±21.13 dB와 18.52±11.83 dB로, 수술 후 기도-골도 청력 역치의 향상 양상은 관찰 되었으나 유의미한 통계학적 차이는 없었다(p=0.22, p=0.21).
유양동성형술 후 청각 재활이 필요한 7명의 환자는 수술 부위 귀에 외이도형 또는 귓속형 보청기를 착용하였다(Table 2). 보청기를 착용한 환자의 보청기 착용 시점은 수술 후 3개월에서 15개월(평균 6.7±4.4개월)이었으며, 보청기 착용 중 되먹임 현상, 외이도염의 문제는 관찰되지 않았고, 불편감이나 다른 문제로 인해 보청기 사용을 중단한 경우는 한 예도 없었다.
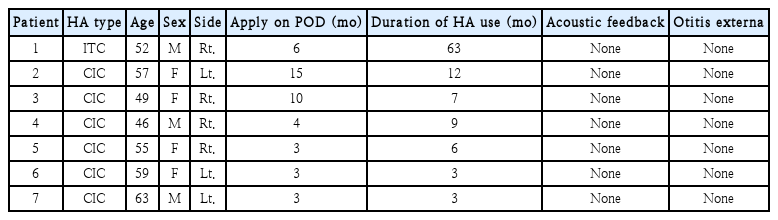
Clinical data of the patients wearing canal type HA after mastoidoplasty with demineralized bone matrix
고 찰
CWDM은 진주종이 동반된 만성 중이염에서 병변을 제거하기 용이하고 재발을 낮추는 데 유리한 수술 방법이나, 외이도 형태의 변화, 공동의 문제 등을 유발할 수 있다. 이러한 단점을 보완하기 위해 외이도 재건 및 유양동 폐쇄하고자 하는 여러 술식이 시도되어 왔다[9,13-16]. Lee 등[17]은 유양동을 지방으로만 폐쇄시 체내 삽입한 지방이 시간이 지남에 따라 약 50% 정도 체적이 감소할 수 있다고 하였다. Weit 등[18]은 hydroxylapatite로 외이도 후벽을 재건하여 90% 이상에서 외이도는 유지되었으나, 일부 환자에서 implant 노출로 외이도성형술 시행 또는 implant 제거를 시행하였다고 보고하였으며, Ikeda 등[19]은 외이도 후벽의 재건 후 일부 환자에서 흡수 및 결손이 발생하였다고 보고하였다. Sioshansi 등[20]은 골분을 이용한 유양동 폐쇄시 약 95%의 환자에서 잘 유지되었으나, 유양동 골피질로부터 충분한 골분을 획득하지 못하는 경우 또한 고려해야 한다고 하였다. 외이도 재건 및 유양동 폐쇄에서 가장 고려해야 할 것으로는 공동을 충분히 메울 수 있는지와, 장기간 추적 관찰 시에 감염 등의 합병증이 없으면서 유양동 폐쇄 용적의 유지 여부이다. 본 연구에서는 골막 피판과 측두근막을 활용하여 외이도 벽을 만들고 CWDM를 시행한 후 남은 유양동 용적에 대하여 DBM을 이용하여 폐쇄함으로써 자가 조직의 사용을 최소화하면서 유양동 폐쇄를 효과적으로 할 수 있음을 확인하였다. 모든 환자에서 수술 후 감염, 염증, DBM의 과도한 흡수로 인한 후이개 피부 함몰이나 외이도의 변형 등이 관찰되지 않아 DBM을 활용한 유양동성형술은 안정한 방법임을 확인할 수 있었다. 또한, 본 연구에서 17예 환자는 이전 CWDM 수술 후 발생한 이루나 공동 문제 혹은 외이도형의 보청기를 활용한 청각재활을 원하여 DBM을 이용한 유양동성형술을 시행하였고. 수술 후 감염, 공동 문제 등 합병증 없이 만족할 만한 결과를 보여주었기에 본 술식은 매우 안전한 술식으로 판단된다.
CWDM를 받은 후 여전히 난청을 지닌 환자의 청각 재활을 고려할 때 술후 발생한 외이도 용적의 증가는 귓속형 보청기 장착에 제약을 가져오고 이로 인해 보청기 선택이 제한적일 수 밖에 없다[21]. 일반적으로 CWDM 후 환자들의 청각 재활을 위해서는 귀걸이(behind-the-ear)형의 보청기 장착을 통해 피드백 발생을 최소화할 수 있으나 미용적인 문제로 환자들이 착용을 거부하는 경우가 많다는 문제점이 있었다. DBM을 통한 유양동 성형술을 시행할 경우 외이도 후벽을 재건하여 외이도형 또는 귓속형 보청기(completely-in-the canal [CIC], in-the-canal [ITC]) 착용이 가능함을 확인할 수 있었고, 실제 본 연구에서 보청기를 처방한 7명의 환자 모두 문제없이 만족하며 보청기를 착용하였다. COVID-19으로 인한 마스크 착용으로 인해 귓바퀴에 거는 귀걸이형 보청기의 경우 미용적 문제 이외에도 보청기 착용의 불편감이 커 환자들의 보청기 착용 순응도가 낮을 수 있는데, CWDM를 받은 환자에게 귓속형 보청기 장착이 가능하게끔 하는 DBM을 활용한 유양동성형술의 술기는 코로나 시기에 청각재활 관점에서도 그 유용성이 더욱 높을 것으로 판단한다. 본 연구의 제한점은 후향적 연구이고 대상자 수가 부족하며, 장기 추적 관찰 연구가 추가적으로 필요할 것으로 판단된다. 또한 다른 재료를 활용한 유양동성형술과의 비교 연구가 아니므로 DBM의 우월성을 입증하지는 못하였다. 향후 본 연구의 제한점을 해결하고 유양동성형술의 유용성과 효과를 검증하기 위한 전향적 무작위대조군연구가 필요할 것으로 생각된다.
결론적으로, DBM을 통한 유양동 성형술은 CWDM 환자에게 외이도 후벽을 재건하여 공동의 문제를 방지하는 안전하고 효과적인 술식으로 판단한다. 아울러 술후 청각재활이 필요한 환자들에게 보청기 선택에 있어 CIC, ITC와 같은 귓속형 보청기를 착용할 수 있게 함으로써 고령화 시대에 대상 환자들의 보청기를 통한청각 재활 용이성을 높일 수 있으리라 기대된다.
Acknowledgements
None
Notes
Author Contribution
Conceptualization: Yeonji Kim, Jae Sang Han, Jae-Hyun Seo, So Yong Park, Shi Nae Park. Data curation: Jae Hong Han, Yeonji Kim, Celeste Ann Chua. Formal analysis: Yeonji Kim, Jae Sang Han, Jae-Hyun Seo, So Yong Park, Shi Nae Park. Methodology: Jae Sang Han, Shi Nae Park. Project administration: Shi Nae Park. Resources: Yeonji Kim. Software: Yeonji Kim. Supervision: Yeonji Kim, Jae Sang Han, Jae-Hyun Seo, So Yong Park, Shi Nae Park. Writing—original draft: Jae Hong Han. Writing—review & editing: Yeonji Kim, Shi Nae Park.