코골이 또는 수면무호흡을 호소하는 한국 환자의 성별에 따른 임상양상 차이: 단일기관 연구
Age Adjusted Sex Differences in Clinical Features of Korean Patients With Snoring or Sleep Apnea: A Single-Center Study
Article information

Trans Abstract
Background and Objectives
Female are less likely to be diagnosed with obstructive sleep apnea (OSA) than male are and their symptoms are more likely to be overlooked because female usually show less typical classic symptoms of OSA, such as snoring, witnessed apnea, and daytime sleepiness. In this study, we identified sex effects among patients who complained of snoring or sleep apnea with adjusting for age.
Subjects and Method
This study design was retrospectively conducted to compare sex and age differences in 255 Korean patients complaining of snoring or sleep apnea by evaluating medical history, rhinomanometry, physical examination, and polysomnography.
Results
The sex difference in the apnea-hypopnea index decreased after 50 years of age. Female OSA patients complained of mild-to-moderate OSA with atypical symptoms. Male OSA patients showed Berlin questionnaire scores, retropalatal Muller maneuver grade, and high body mass index (BMI) as significant risk factors for OSA after adjusting for age. Female OSA patients showed retropalatal Muller maneuver grade and high BMI as significant risk factors. Berlin score was a typical risk factor in old male OSA patients.
Conclusion
Anatomical and hormonal factors were thought to be risk factors for OSA especially in females, but contrary to expectations, there were no risk factors in old females when adjusted for age. A careful approach should be taken to avoid overlooking sleep apnea in female.
Introduction
Obstructive sleep apnea (OSA) can be diagnosed using apnea-hypopnea index (AHI) or respiratory disturbance index(RDI) values of ≥15 events per hour in an asymptomatic patient or AHI or RDI ≥5 events per hour in a patient with symptoms or signs of disturbed sleep [1].
In the general population, the prevalence of OSA has been reported to range from 9% to 38% [2] and almost 1 billion people globally are estimated to be affected [3]. The prevalence of OSA is also known to be affected by many risk factors including age, sex, and weight [4]. Age is a very important risk factor. Although the prevalence of OSA peaks in middle age, the prevalence of sleep apnea is known to increase with age. It is also noted that the severity of sleep apnea decreases with age [5].
Besides age, OSA shows a unique clinical picture by sex. First, OSA is more common in male than female and the male-to-female ratio of OSA is usually estimated to range from 3:1 to 5:1 in the general population [6]. However, as age increases, this gap in OSA prevalence between males and females decreases because the prevalence of female OSA patients increases after menopause [7]. This may be associated with changes in the level of hormones such as progesterone or estrogen [8].
Second, the severity and symptoms of OSA patients differ by sex. In general, male have more severe OSA and female have less severe symptoms at all ages [9]. Male OSA patients complain more commonly of classic symptoms, such as sleepiness, snoring, or witnessed apnea. However, female OSA patients complain of atypical symptoms, such as insomnia or morning headache [10]. This is one of the reasons why female OSA patients are often undiagnosed.
Third, not only the symptoms were shown to differ with sex but differences were seen in polysomnographic data. Male OSA patients were found to have severe OSA with higher AHI values and higher supine AHI values than female OSA patients [11], but the rapid eye movement AHI values were reported to be higher in females [10].
Considering the above, it is important to understand the differences between male and female OSA patients and consider the differences in clinical features before and after menopause in female for proper diagnosis and treatment. However, no studies have examined the effects of menopause on OSA in a large Asian OSA patient group without adjusting age.
This study aimed to identify the differences in OSA risk factors by sex and the effect of menopause on OSA by analyzing OSA-related questionnaires scores, physical findings like tonsil size, palatal position, and Muller maneuver grade results using 2 age-matched sex groups after adjusting for age.
Subjects and Method
Data collection
This study was comprised of a sample of 255 patients in a single-center who complained of sleep apnea or snoring based on a retrospective review of medical records from January 2015 to May 2020. Demographic data such as age, medical history, smoking history, and comorbidities were also collected from the medical records. The medical records also include symptoms confirmed with yes/no such as morning headache, snoring, witnessed sleep apnea, mouth breathing, frequent night awakeness, difficulty in falling asleep and re-falling asleep, limb movement during sleep and daytime sleepiness/ fatigue/nap. All patients were administered the Berlin questionnaire, Epworth Sleepiness Scale (ESS) test, laryngoscope test, rhinomanometry, and overnight full-attended polysomnography (PSG) examination. Patients who failed to take overnight PSG examinations were excluded and 255 patients were finally included in the study.
The protocol for this study was approved by Institutional Review Committee, St. Vincent Hospital, the Catholic University, Suwon, Republic of Korea (VC20RISI0194).
Physical examination
All patients underwent physical examination including laryngoscopic examination in a sitting position. The tonsil size was evaluated on a 4-point scale by oral examination: none (0), small inside the tonsillar fossa (1+), laterally extending to the tonsillar pillar (2+), hypertrophic but to the midline. Not large (3+), large enough to touch the midline (4+). The positional relationship between palate and tongue was evaluated with a 4-point grade by Frieman’s modification of Mallampati classification [12].
The modified Muller’s maneuver evaluated the collapsibility of the pharyngeal wall with the patient’s nose and mouth completely closed and forced inspiration. The degree of obstruction was evaluated with the Fujita classification as follows [13]. type 1) upper pharyngeal obstruction, type 2) oropharyngeal and hypopharyngeal obstruction, type 3) hypopharyngeal obstruction [3].
Body composition parameters
Body mass index (BMI, kg/m2) was calculated by dividing the weight (kg) by the square of height (m). The neck, waist, and hip circumferences were measured by 2 nurses in our department.
Rhinomanometry
Active anterior rhinomanometry was used to measure the patient’s nasal resistance and patency. An experienced technician measured the patients’ nasal resistance and flow with the Rhinomanometrie 300 (ATMOS Medizin Technik GmbH & Co. KG, Lenzkirch, Germany). The nasal resistance was measured at each nostril by dividing the nasal pressure by the natural airflow (V). The nasal resistance (Pa/cm3/second) was calculated according to the Standardization Committee on Objective Assessment of the Nasal Airway recommendations [14].
PSG
Overnight full-attended PSG was performed with Rem-Logic-E ver.3.4.1 software and recorded with Embla N7000/ S7000 hardware (Embla Systems, Inc., Broomfield, CO, USA) at the sleep center of St. Vincent Hospital.
OSA was defined as an AHI or RDI value of ≥5 events per hour on an overnight full-attended PSG examination in a patient with symptoms or signs.
All PSG data were scored by the 2 sleep technicians and reviewed by the same sleep specialist. Sleep stages, respiratory events, arousals, movements, and sleep-related events index were scored according to the criteria in the American Academy of Sleep Medicine Scoring Manual version 2.4 [15]. The sleep specialist diagnosed the severity of OSA.
Statistical analysis
The data were presented as n (%) for categorical variables or mean value±standard deviation for continuous variables. The baseline variables were analyzed by independent t-test based on normality, Wilcoxon rank sum test, or chi-square test. The associations between OSA and independent variables were confirmed through univariable and multivariable logistic regression analysis. All data analyses were performed using the SPSS 20 (IBM Corp., Armonk, NY, USA). p<0.05 was considered statistically significant.
Results
The characteristics between male and female subjects
The data from 255 age-matched patients were analyzed retrospectively. According to the OSA severity, the subjects were divided into 4 subgroups, normal, mild, moderate, and severe subgroup. The numbers of male and female subjects in each subgroup are shown in Fig. 1. There were more female patients than male patients in normal (p=0.225), mild (p=0.452), and moderate OSA patients’ group (p=0.028), but more male patients had severe OSA patients’ group (p=0.001).
Prevalence of OSA group in male & female patients with snoring and sleep apnea. *p value<0.05 for difference. OSA, obstructive sleep apnea.
Although the mean age, ESS, and Berlin questionnaire results between the groups were not significantly different, smoking history and symptoms like witnessed sleep apnea, limb movement during sleep, and daytime sleepiness or fatigue were significantly different between the male and female subjects.
Many body composition parameters were significantly higher in the male group, such as neck, waist, and hip circumferences, the neck-to-height ratio, BMI, and total nasal resistance of under 75 pascals before or after mucosal constriction was significantly higher in female than male subjects.
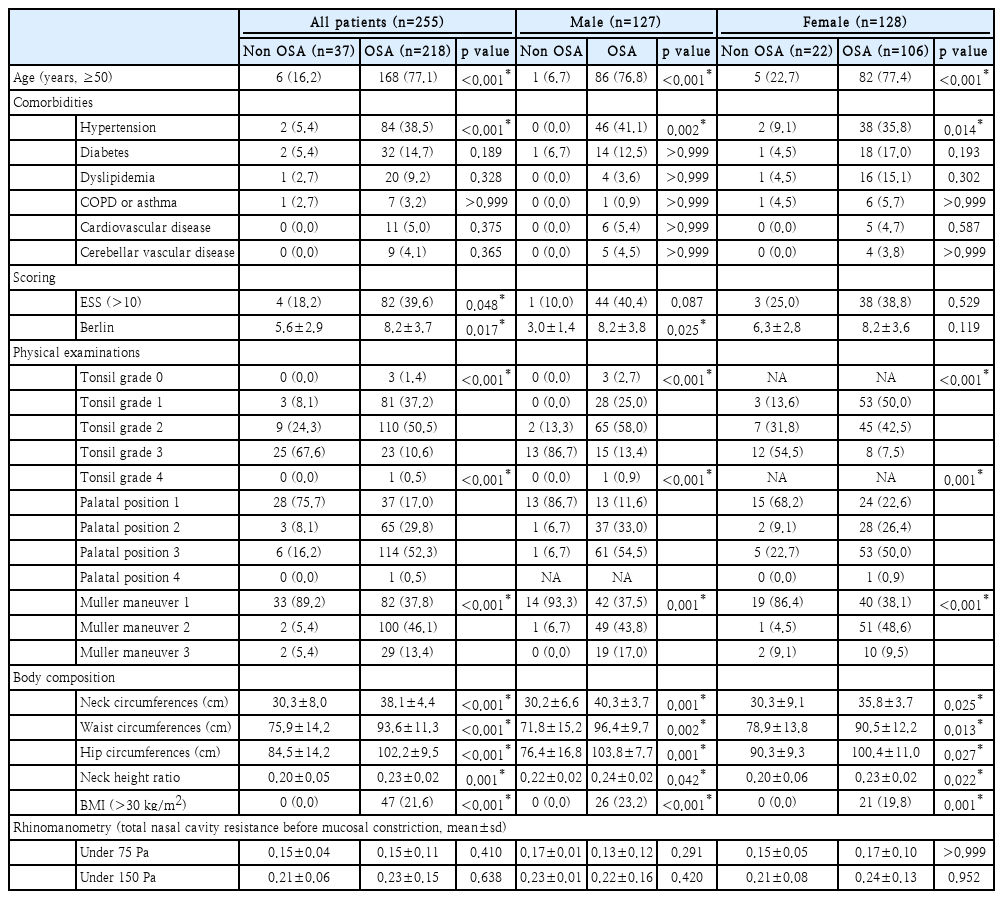
Different OSA risk factors between male and female patients
Table 1 presents the OSA risk factors in all subjects, the male group, and the female group. Age (older than 50 years), ESS and Berlin questionnaire results, and the results of the tonsil size, the palatal position and Muller maneuver were significantly different between the non-OSA and OSA sub-groups. Rhinomanometry results showed no significant difference between non-OSA and OSA subgroups for male as well as female patients in Table 1.
Associations between multiple factors and OSA (AHI or RDI ≥5)
The logistic regression results in Table 2 show that age (old-er than 50 years), hypertension, lower Muller maneuver grade, neck-height ratio, and BMI (>25 kg/m2) were highly related to OSA in all subjects. However, after adjusting for age, high Berlin scores (odds ratio [OR] 2.82, 95% confidence interval [CI] 1.11-7.18, p=0.030), Muller maneuver grade I (OR 8.97, 95% CI 1.37-58.68, p=0.022), and high BMI were highly related to OSA in the male OSA patients. In the female OSA patients, Muller maneuver grade I (OR 11.46, 95% CI 1.95-67.20, p=0.007) and morbid obesity with high BMI (≥30 kg/m2, OR 23.27, 95% CI 1.15-469.5, p=0.040) were highly related to OSA.
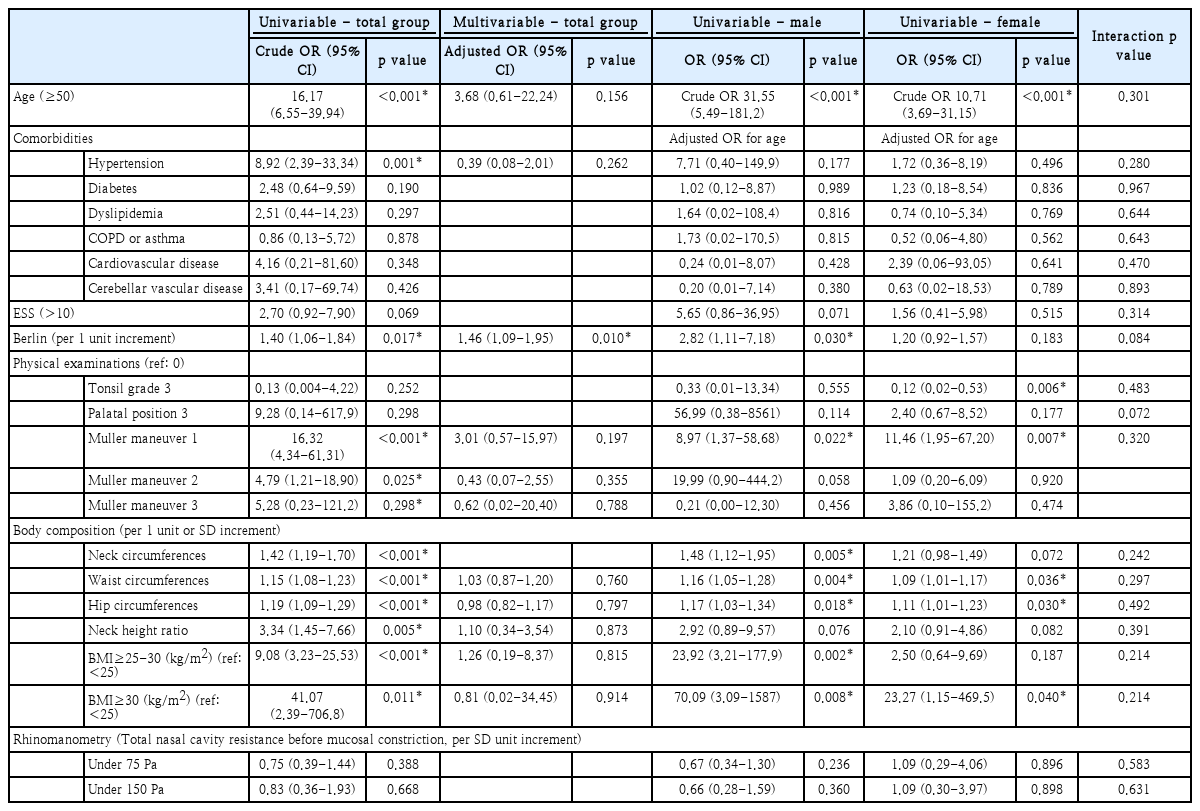
Univariable and multivariable logistic regression analyses of predictors of OSA (AHI or RDI ≥5)
In conclusion, there was no difference in risk factors for OSA between the male and female groups except for Berlin questionnaire scores, retropalatal Muller grade, neck circumference, and high BMI after adjusting for age.
OSA risk factors related to age in male and female OSA patients
In the Republic of Korea, the mean age of menopause is as early as 50 years old and so the age of 50 was used as the cut-off point between young and old patients to analyze the effect of menopause on OSA in female patients.
The significant association between multiple factors and sex according to 50 years old age is summarized in Table 3. After adjusting for age, only obesity was highly correlated with young male OSA patients. In the old male OSA patients, only high Berlin questionnaire scores were highly related to OSA. However, these factors are not significant risk factors in old and young female OSA patients.

Univariable logistic regression analyses by sex and interaction (sex×predictor) in the <50, ≥50 age group
Especially for age, the gap between the average AHI values in male and female subjects decreased after the age of 50 because the AHI values of older male OSA patients decreased and the AHI values of female OSA patients slightly but steadily increased (Fig. 2).

Comparison of AHI between male and female group according to the age groups. AHI, apnea-hypopnea index.
Discussions
This study aimed to analyze the differences in Korean male and female sleep-disordered breathing patients visiting a single-center according to sex and age and identify the association between OSA and sex-specific factors after adjusting for age. For this purpose, we used multiple parameters and results from the patient’s history, clinical features, and parameters, the evaluation with parameters like ESS and Berlin questionnaire scores, physical examinations, body composition, rhinomanometry, and PSG examinations.
In the general population, the prevalence of moderate-to-severe OSA is higher in male than in female after corrections for age and BMI [16]. Similar to previous studies [17], typical OSA symptoms like witnessed sleep apnea and daytime sleepiness were observed more in male patients with statistically significant differences in this study.
Age (≥50 years) and hypertension were significantly associated with OSA in both sexs but hypertension was not significantly related to OSA in male and female group after adjusting for age, contrary to previous studies [18].
The prevalence of female OSA seems to be sex hormone-dependent, so postmenopausal female are more likely to visit clinical practices for sleep-disordered breathing. However, our results showed that OSA was more prevalent in middle-aged male and female, contrary to other studies showing that OSA was more prevalent in elderly than middle-aged female [5]. This may be because postmenopausal women show less typical OSA symptoms than middle aged women. Postmenopausal women may have more changes in body composition affecting OSA than middle aged women. Similar to previous studies, our results also showed the prevalence of severe OSA was higher in male than in female [17].
In our study, the gap between the average AHI values for male and female OSA patients look similar to that from previous study. Other studies reported that the difference in AHI values between male and female OSA patients decreased after the ages of 60-62 years [19]. Perger, et al. [8] reported that the differences in OSA severity depending upon sex tended to be attenuated in postmenopausal patients and the prevalence of postmenopausal OSA patients increased. One possible explanation for this difference is obesity and fat distribution, which are affected by age and sex (by sex hormones) [20]. However, many studies have shown inconsistent results for the association of OSA with sex-related obesity. Some studies reported that BMI in male and female OSA patients was not very different [17], and other studies reported that the BMI of female OSA patients was higher than that of male OSA patients Some studies showed that male OSA patients were significantly younger than female patients and had lower BMI values. Our findings showed that the average age of the male and female patients was similar at around 49 years old, and the BMI was significantly higher in male patients. Both male and female OSA patients were significantly older than 50 years old. The logistic regression results showed that the OR for old age and high BMI in male OSA patients was greater than in female OSA patients. In particular, a high BMI from 25 to 30 kg/m2 was identified as a significant risk factor for OSA in young male OSA patients under the age of 50 after adjusting for age. A previous study demonstrated differences in neck fat deposition between males and females, which, together with the greater overall soft tissue loading in the airway of male, may be factors in the sex distribution of OSA [21].
After adjusting for age, only obesity and high Berlin questionnaire scores were significant risk factor for young male and old male OSA patients, respectively. Unlike previous studies, where anatomical and hormonal factors were thought to be risk factors for OSA, especially in female patients, when adjusting for age, there were no risk factors in elderly female patients. Non-anatomical factors like neuromuscular/respiratory dysfunction may be more important in female patients.
The ESS and Berlin questionnaires were very useful screening tools for sleepiness and OSA. Pataka, et al. [22] reported that the Berlin questionnaires scores in female OSA patients were relatively lower than in male patients and ESS did not differ between the sexs. In general, there were no sex differences in the prevalence of excessive daytime sleepiness scores of more than 10, but extreme daytime sleepiness scores of more than 16 were more prevalent in male OSA patients [23]. In our study, the Berlin questionnaire scores were identified as a significant risk factor for OSA especially in old male OSA patients with high OR.
Friedman, et al. [12] reported that big tonsils and uvula, a narrow oropharyngeal space, and low-lying soft palate were associated with OSA in obese patients. However, these pharyngeal structures may not play a significant role in patients with snoring because the success rate of uvulopalatopharyngoplasty is only 40.7% [24]. Wu, et al. [25] also reported that tonsil size, uvula, and soft palate redundancy in male and female OSA patients were not significant risk factors for OSA. Considering the above findings, the inconsistency of our results with the common beliefs that bigger tonsils might be closely related to OSA might suggest that anatomical factors play less-essential roles in OSA pathophysiology. Dynamic airway obstruction found by the Muller maneuver was significant in both sexs, which was different from the results of Wu, et al. [25] that a high retropalatal Muller grade was a significant risk factor in non-obese male OSA patients.
Neck and waist circumferences, and the associated ratios of male patients were larger than female patients with snoring or sleep apnea. Both male and female OSA patients had higher neck, waist, hip circumferences, and neck-height ratio then non OSA patients with statistical significance. These factors are also identified in univariable logistic regression as significant risk factors for OSA with low OR. However, after adjusting for age, no body compositional factor was significant risk factor for OSA in young and old group except BMI. Contrary to our results, Kang, et al. [26] and Amra, et al. [27] reported that anthropometric indices such as neck circumferences and waist circumferences were risk factors for OSA.
Multiple factors such as fat distribution, upper airway structure, and sex hormones have been reported to affect the prevalence of OSA by sex [28]. Thus, we hypothesized that females under and over the age of 50 years might show different body composition features because the mean age of menopause in the Republic of Korea is around the age of 50 years, which was not confirmed in our study.
In our study, there are no statistically significant differences in rhinomanometry results between normal and OSA, young-er and older female group. Avcı, et al. [29] also reported that there was no correlation between the nasal resistance measured by passive rhinomanometry, AHI, and other polysomnographic parameters. However, the correlation between nasal stuffiness and apnea severity has been described differently in several studies [30,31]. The importance of nasal stuffiness and apnea severity is unclear and needs further study.
This study had several limitations. First, a further prospective longitudinal study is required to identify the effects of OSA on the severity of variables such as ESS and Berlin questionnaire scores, and other physical findings. Second, a largescale further study enrolling more normal controls without OSA is required. Third, although the effect of menopause in the female group was considered in this study, it is necessary to confirm menopausal status through hormone level confirmation or history-taking for female OSA patients, and not simply assume menopausal status according to age. Lastly, the results of the ESS and Berlin questionnaire may vary de-pending upon the patient’s understanding of sleep symptoms and OSA.
In conclusion, we confirmed that severe OSA and typical OSA symptoms had a high prevalence in male patients, whereas mild-to-moderate OSA was more prevalent in the female patients in Korean population. The gap in average AHI values between male and female OSA patients was relatively high in patients under 50 years old and low in those over 50 years old. Multiple risk factors for OSA patients depending on sex and age were summarized in Fig. 3. There were no risk fac-tors in old female patients after adjusting age. Non-anatomical factors like neuromuscular/respiratory dysfunction may effect on risk factors for female OSA patients. Evaluation tools for OSA such as sleep-related questionnaires and physical examinations should be chosen depending upon the patient. Young female, young male, old female, and old male-specific screening tools for OSA could be helpful for early diagnosis and individualized treatment.
Multiple risk factors for OSA patients depending on sex and age from univariable logistic regression analysis with adjusting for age. *univariable logistic regression analysis, p<0.001.
Acknowledgements
Statistical consultation and analysis were performed by staff at the Department of Biostatistics of the Catholic Research Coordinating Center.
Notes
Author Contribution
Conceptualization: Chan-Soon Park, Jin-Hee Cho. Data curation: Min Ju Kang. Formal analysis: Jae Seong An. Investigation: Jae Seong An, Soo Ah Son. Methodology: Chan-Soon Park, Jin-Hee Cho. Project administration: Yun Jin Kang, Jin-Hee Cho. Software: Yun Jin Kang, Min Ju Kang. Supervision: Chan-Soon Park, Jin-Hee Cho. Validation: Yun Jin Kang. Visualization: Yun Jin Kang, Soo Ah Son. Writing—original draft: Yun Jin Kang. Writing—review & editing: Chan-Soon Park, Jae Seong An.