구강 내시경 갑상선 수술의 이점 및 한계점
Benefits and Limitations in Transoral Endoscopic Thyroidectomy
Article information

Trans Abstract
Transoral endoscopic thyroidectomy (TOET) is the recent remote access approach which leaves no cutaneous scar in the body. It has advantages in minimize the surgical dissection, could perform total thyroidectomy and central lymph node dissection easily under a good surgical view. TOET has gained popularity in both the East and Western countries since the first large series report by Dr. Anuwong in 2016. In this article we described and critically analyze the indications and contraindications, advantages and limitations, landmarks for recurrent laryngeal nerve and strategies for superior pole dissection in transoral thyroidectomy.
서 론
지난 30년간 갑상선 수술에 있어 최소 침습적인 수술의 일환으로 내시경 및 로봇 수술이 개발되어왔다. 하지만 복부나 흉부와 다르게 경부는 구조적으로 미세 침습 수술이 적용되기 힘들다. 갑상선암은 여성들에게 많이 생기며 상대적으로 좋은 예후로 수술 후 삶의 질에 대하여 관심이 많은 편이다. Choi 등[1]에 의하면 갑상선 수술 후 생긴 경부의 상처가 삶의 질의 유의미한 저하와 관련이 있다고 보고하였다. 실제로 갑상선 수술을 받은 환자의 약 20% 정도가 경부 상처로 인하여 사회생활 등의 불편감을 호소하였고, 10% 정도의 환자들은 성형 수술 등을 고려하는 것으로 보고된 바 있다[2]. 경액와 접근법(transaxillary approach), 양측 액와-유방 접근법(bilateral axillo-breast approach), 후이개 접근법(retroauricular approach) 등 다양한 내시경 및 로봇 수술 방법들이 소개 되었지만 긴 절개선, 광범위한 피판 거상, 긴 수술 시간 등으로 기존의 수술에 비해 침습도가 높음에 대한 비판이 있었다[3-5]. 특히 이러한 수술 방법은 비만도가 상대적으로 높은 서양에서 높은 침습도 및 관련된 합병증으로 인해 적극적으로 도입되지 못했다. 구강 내시경 갑상선 수술(transoral endoscopic thyroidectomy vestibular approach)은 2016년 Anuwong [6]의 보고 후 적극적으로 도입되기 시작한 방법으로, 다른 내시경 수술 방법에 비해 절개선과 갑상선과의 거리가 짧아 덜 침습적인 점, 피부 절개선이 없어 미용적으로 우수한 점, 가운데로 접근하여 양측 갑상선 수술이 용이하다는 점 등으로 각광받는 수술 방법이다. 기존의 내시경 수술 방법들이 상대적으로 아시아 국가들 위주에서만 시행된 반면, 구강 내시경 갑상선 수술은 서양 국가들 및 아시아 외의 여러 국가들에서도 많이 시행되고 있다. 본 종설에서는 이 수술 방법의 장점, 단점 및 여러 고려할 점들에 대하여 문헌 고찰 등을 통하여 정리해보고자 한다.
본 론
구강 내시경 갑상선 수술의 적용
구강 내시경 갑상선 수술의 안정성 및 우수한 결과 보고들에도 이 수술법이 어디까지 적용될 수 있는지에 대한 논의들이 있다. 물론 수술의 적응증은 술자의 경험 정도에 따라 달라질 수 있으나 일반적으로 적용되고, 저자가 사용하는 적응증은 먼저 흉터가 없는 수술을 받고자 하는 강한 욕구가 전제되어야 하며, 1) 갑상선의 최대 장경은 10 cm 이하, 2) 양성 결절 또는 여포성 종양의 경우 크기 6 cm 이하, 3) 고분화 갑상선암의 경우 크기 2 cm 이하이다. 금기가 되는 적응증은 1) 측경부 임파선 전이, 2) 갑상선 외 침윤이 있는 경우, 3) 미분화 또는 저분화 갑상선암인 경우, 4) 경부 수술의 기왕력이 있다[7,8]. 종양이 큰 경우 입으로 검체를 꺼내기가 힘든 부분이 있어, 겨드랑이에 절개를 넣어 빼는 방법, 입술의 중앙 절개 부위를 확장하여 빼는 방법, 양성인 경우 검체를 몇 조각으로 나눠서 빼는 방법이 있다[9,10]. Wu 등[11]은 악성 결절이 2 cm 이상인 경우 검체를 꺼낼 때 종양이 분절되어 정확한 병기를 알기 어려워 이러한 경우 겨드랑이 절개를 넣어 빼는 방법을 권고한 바 있다.
앞서 언급하였듯이 수술의 적응증은 술자의 경험의 정도에 따라 다를 수 있다. 중앙 임파선 전이가 있는 경우 기존의 보고들에서 수술의 금기증으로 많이 언급이 되었으나, 이 수술의 특성상 위에서 아래를 보며 접근하기 때문에 오히려 중앙 임파선 절제술(central neck dissection)이 용이할 수 있다[7]. 출혈 경향이 있으며 갑상선이 큰 그레이브스병(Graves’ disease)에서도 고식적인 경부 접근법과 비교하여 합병증 차이가 없어 안전한 방법으로 보고되기도 하였다[12]. 갑상선 외침윤이 있는 경우 금기증으로 언급하였으나, 갑상선의 전방에 위치한 피대근(strap muscle)에 침범이 있는 경우는 구강 내시경 접근법을 이용하여 절제하는 데 어려움은 없다. 하지만 갑상선의 후방 부위인 기관, 식도, 갑상연골 등에 침범이 의심되는 경우는 수술에 제한이 있어 술전에 면밀한 초음파를 통한 평가가 중요하다. 또한 초음파를 통하여 갑상선의 크기, 갑상선 협부(isthmus)의 두께, 갑상선 상엽의 범위 등을 파악하면 수술 시 도움이 된다. 구강 내시경 접근법을 통한 잔존 갑상선 절제술(completion thyroidectomy)은 첫 번째 수술 후 2-3주 이내에는 특별한 어려움 없이 시행 가능하며, 그 이후에 시행해야 하는 경우에는 수술 6개월 이후에 하는 것이 좋을 것으로 권고되나 보고는 미미하다[13,14].
경액와 접근법 및 양측 액와-유방 접근법이 비만도가 높은 서양에서 적용하기 어려웠던 반면, 구강 내시경 갑상선 수술은 비만도가 수술 시간 및 합병증에 영향을 주지 않는다고 보고되어 적용범위가 넓어졌다고 볼 수 있다[15,16]. 하지만 초보자의 경우 종양이 갑상선의 상엽에 있는 경우 내시경의 수술 시야가 좁고, 기구의 충돌이 잦아 수술에 제한이 될 수 있으므로 이 부위에 악성결절이 있는 경우 피하는 것이 좋다. 또한 환자의 외모상 턱이 많이 돌출되어 있으며 피하지방이 매우 적어 피부가 얇게 만져지는 환자는 술후 피판(flap) 관련된 합병증 가능성이 높아 저자의 경우 선호하지 않는 적응증이다. 또한 남성의 경우 갑상연골이 돌출되어 있어 수술 시야에 제한을 주고 피하 지방이 적어 내시경 기구를 조작하기가 여성에 비하여 어려워 초보자의 경우 적절한 적응증이 아니다. Table 1에서 구강 내시경 수술의 적응증 및 초보자가 시행하기에 이상적인 환자에 대하여 정리했다.

Indications for transoral endoscopic thyroidecomy
구강 내시경 갑상선 수술의 이점 및 한계점
기존의 내시경 접근법들이 피부 절개를 눈에 띄지 않는 곳에 숨기는데 반해 구강 내시경 접근법은 구강 점막에 절개를 하여 피부절개가 없는 유일한 방법이다. 실제로 여러 보고들을 통하여 다른 내시경 접근법들보다 환자들이 미용적으로 더 만족함을 알 수 있었다[17,18]. 하지만 구강 내시경 접근법은 입술 및 하악 부위를 통하여 접근하는 방법으로 수술 후 이 부위에 합병증이 생긴다면 미용적으로 치명적인 결과를 초래할 수 있다. 유의해야 할 미용 관련 합병증으로는 외측 입술 점막 찢김, 얼굴 부위 멍듦, 턱 부위 함몰, 입술 움직임 비대칭, 턱 부위 피부 천공 및 턱밑 부위에 밴드 형성이 있다(Fig. 1). 특히, 턱 부위 함몰, 턱밑 부위에 밴드 형성은 수술 후 시간이 지나도 호전되지 않고 지속되는 경우가 있다. 이러한 합병증은 거상된 피부 피판이 얇아서 생기는 경우가 많기 때문에 피판을 하악의 골막하 공간으로 하악의 하연까지 거상시키면 피판이 두꺼워져 이를 예방할 수 있다[19]. 또한 술후 조기에 환자에게 목 운동 교육 및 권장 시 턱밑 부위에 밴드 형성 등의 수술 부위 유착을 완화시켜주는 방법이다. 수술 후 입술 움직임의 비대칭을 보이는 경우도 있는데, 이는 입술 부위의 상처 치유과정 중의 일시적인 현상으로 보인다[18].

Intraoperative and postoperative photo. A: The incision in the oral vestibule. B: Excellent cosmesis taken 1 week after surgery. C: Skin ecchymosis and bruising. D: Skin dimpling on chin. E: Band formation under the chin.
구강 내시경 갑상선 수술은 양측 수술 즉, 갑상선 전절제술이 가능하다는 장점이 있다. 이는 양측 액와-유방 접근법과 같이 중앙에서 접근하는 방법이기 때문이다. 구강 내시경 갑상선 수술이 상대적으로 시간이 긴 편이지만, 구강 내시경 접근법으로 전절제술을 하는 경우, 편측 수술과 비교해서 수술 시간이 20-30분 정도만 추가적으로 필요한 것으로 보고되어 갑상선 전절제술 대상 환자에서 여러 내시경 갑상선 수술 중 더욱 추천된다고 볼 수 있다[20].
내시경 갑상선 수술 방법 중에 구강 내시경 접근법이 수술 시행 공간(working space)이 가장 좁아 통증이 적으며 최소 침습적인 수술이라는 장점이 있는데 반해, 수술 시간을 비교한 보고들에서 다른 내시경 접근법에 비해 오히려 수술 시간이 긴 것으로 보고되었다[18]. 이는 양측 구강 점막으로 삽입되는 내시경 수술 기구가 턱 부위에서 피봇(pivot)을 형성하며 움직이게 되어 기구 움직임이 제한되는 측면에 기인한 면이 있다. 그러므로 수술 초반 외측 투관침(trocar)을 삽입 시 적절한 각도로 삽입하는 것이 중요하다. 또한 수술 시행 공간이 상대적으로 좁기 때문에 긴 내시경 수술 기구가 움직이는데 다른 내시경 접근법에 비해 제한되는 측면도 있다. 그러므로 초심자의 경우 수술 시행 공간을 표준대로 외측으로는 양측 흉쇄유돌근(sternocleidomastoid muscle, scm)까지, 아래로는 흉골절흔(sternal notch)까지 노출시켜 수술하는 것이 좋으며, 익숙한 술자의 경우 수술 시행 공간을 줄여 수술 후 통증, 출혈, 장액의 형성을 줄일 수도 있다.
2018년도 Anuwong 등[21]이 425명의 구강 내시경 갑상선 수술 환자에 대한 경험을 보고하며 이 방법이 안전하고 용이한 방법으로 소개하였다. 하지만 이 보고에서 갑상선암 환자의 비율은 6% 정도로 미미하여 전 세계적으로 유병률이 높아지고 있는 갑상선암 치료 유용성에 대해서는 의문이 있었다. 이후 한국 등에서 갑상선암에서도 안전하게 수술할 수 있음이 보고되었으나 아직은 장기간 연구가 부족하다. Ahn과 Yi [22]는 구강 내시경 접근법 및 고식적인 경부 접근법으로 갑상선전절제술을 시행받은 환자들을 대상으로 수술 후 자극 갑상선글로불린(stimulated thyroglobulin, sTg)을 측정하였 는데, sTg가 1.0 ng/mL 미만인 비율이 두 그룹 간에 차이가 없었으며 이는 수술의 완전성(completeness)이 비슷하다고 볼 수 있다. 앞서 언급하였듯이 초기에는 갑상선암에 대한 안전성이 확립되지 않아 중앙 임파선 절제술의 안전성에 대해 서도 보고가 적었다. Wang 등[23]은 80명의 구강 접근법 환자와 매칭을 통해 선정한 80명의 경부접근법 환자에서 중앙임파선 절제술 결과를 분석하였는데, 절제된 림프절수, 수술 시간 및 합병증 모두 차이가 없음을 보고하였다. 구강 내시경 접근법은 위에서 아래를 보며 접근하기 때문에 흉골 및 쇄골에 의한 시야장애가 없어 고식적인 경부접근법에 비해 절제 림프절 수가 오히려 더 많다고 보고한 문헌도 있다[7]. 이러한 점들을 고려했을 때 구강접근법을 이용한 중앙 임파선 절제술은 안전하며 용이한 방법으로 생각된다(Fig. 2).
Intraoperative view. A: Performing left central neck dissection. B: After completing central neck dissection showing wide view of the lower neck (arrows: recurrent laryngeal nerve). ST, sternothyroid muscle; T, trachea.
구강 내시경 접근법에서도 반회후두신경 손상이 발생할 수 있으며 현재까지 보고된 바에 따르면 고식적인 경부 접근법 및 다른 내시경 접근법과 비교했을 때 반회후두신경 손상 비율은 비슷하다[20,21]. 하지만 구강 내시경 접근법 특성상 위에서 아래로 박리를 해야하며, 신경을 근위부 즉, 후두 입구부(laryngeal entry point)에서 찾아야 하는 점이 다른 접근법과 다른 점이다. 보통 갑상선절제술 시 반회후두신경을 찾기 위한 표식(landmark)들이 있는데, 구강 내시경 접근법에서는 아직 반회후두신경을 찾기 위한 표식들이 정리되어 있지 않아 저자의 경험 및 문헌들을 참고하여 정리하였다(Table 2). 먼저, 상부 부갑상선(superior parathyroid gland)은 갑상선 상극 부위의 배측(ventral aspect)에 변이가 없이 위치가 일정한 편이다. 구강 내시경 접근법에서 먼저 상극 박리를 하면 상부 부갑상선이 노출되게 되는데, 반회후두신경은 대부분이 상부 부갑상선의 내측에 위치하게 된다(Fig. 3A). 두 번째로, 반회후두신경과 제1기관륜(tracheal ring)과의 관계에 대하여 분석한 보고에 따르면, 반회후두신경은 제1기관륜 위치에서 항상 기관(trachea)의 수직 높이의 중간 아래에 위치하며, 좌측 반회후두신경은 우측에 비해 보다 더 하방 깊이 위치한다고 분석하였다[24]. 구강 내시경 접근법은 반회후두신경을 후두 입구부에서 찾기 때문에 이 해부학적 보고가 도움이 된다(Fig. 3B and C). 셋째로, Zuckerkandl 결절(Zuckerkandl’s tubercle, ZT)은 갑상선의 측면 경계에서 외측 후방으로 가장 돌출된 부위로 전체 갑상선 환자의 70% 이상에서 존재하는 것으로 알려져 있다. 반회후두신경과 ZT와의 관계에 대하여 분석한 메타분석에 따르면, 약 85%에서 반회후두신경은 ZT의 후내측(posteromedial)에 위치하는 것을 보고하였다[25]. ZT는 구강 내시경 접근법에서 반회후두신경을 노출 시 흔히 노출되는 구조물이기에 중요한 표식이 된다(Fig. 3D). 이러한 중요한 지표들이 구강 내시경 접근법에서 반회후두신경을 찾는데 도움이 되지만, 반회후두신경의 변이들(신경이 후두 진입 전에 분지되는 경우(extralaryngeal branch), 비회귀성 반회후두신경(non-recurrent laryngeal nerve), goiter 등에 의하여 신경이 비뚤어져 있는 경우(distorted nerve)가 있어 항상 주의를 요한다. 또한, 수술 중 신경모니터링(intraoperative neuromonitoring)이 추가적인 기구 사용에 대한 비용은 들지만 신경을 찾는 유용한 방법이다[18]. 마지막으로, 갑상선 상극 박리는 앞서 언급한 것처럼 위에서 아래를 보는 내시경의 각도 및 기구의 충돌 등으로 상대적으로 어려운 편이다[26]. 이에 상극 박리를 보다 쉽게 하기 위한 방법에 대하여 Table 3에 정리하였다.
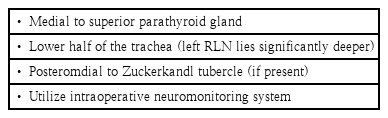
Landmarks and strategies to identify RLN
Identification of RLN. A: RLN lies medial to superior parathyroid gland. B: Left RLN lies deep in the lower half of the trachea. C: Right RLN lies in the lower half of the trachea. D: RLN lies posteromedial to the Zuckerkandl tubercle. Arrows: RLN. SPG, superior parathyroid gland; T, trachea; ZT, Zuckerkandl tubercle; RLN, recurrent laryngeal nerve.
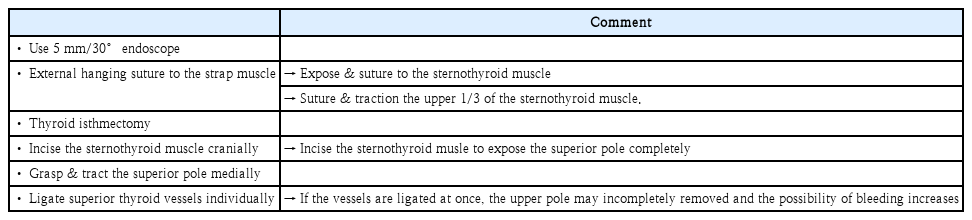
Strategies for superior pole dissection
결 론
구강 내시경 접근법은 가장 최신의 갑상선 수술법으로 피부의 절개선 없이 양측 갑상선 절제술을 쉽게 할 수 있으며 기존의 내시경 접근법들과 비교해 덜 침습적인 수술법이다. 전 세계적으로도 많이 보급되어지고 있지만, 수술 시 생길 수 있는 합병증 및 기술적인 한계점들이 있다. 현재도 이 수술법은 내시경 및 내시경 기구의 발전, 로봇 수술의 적용 등으로 한계점들을 극복해나가고 있다. 특히 본 논문에서는 기술적인 한계를 극복하기 위한 방법들을 기술하였다. 더 나아가, 안전한 수술을 위하여 의사들을 위한 교육 프로그램 및 가이드라인의 개발 등이 필요하며 향후 갑상선 수술의 최선의 선택이 될 것으로 기대한다.
Acknowledgements
This paper was supported by Fund of Biomedial Research Institute, Jeonbuk National University Hospital.