연속으로 시행한 등골 수술 100예의 원인 질환과 청력 결과 분석
Analysis of Causative Disorders and Hearing Improvement in 100 Consecutive Stapes Surgeries
Article information

Trans Abstract
Background and Objectives
Stapes surgery has been widely used to improve the conductive hearing loss caused by stapedial fixation. The purpose of this study is to evaluate the causes of stapedial fixation using audiological results of 100 stapes surgeries.
Subjects and Method
We reviewed the medical records of 100 consecutive stapes surgeries between June 2011 and December 2022. A total of 100 ears from 86 patients were included and the patient age ranged from 6 to 80 years. Hearing improvements of pure-tone thresholds were defined as successful when air-bone gap (ABG) was reduced to 20 dB or less, and as excellent when ABG was reduced to within 10 dB.
Results
The causative diseases of stapedial fixation were otosclerosis (n=74, 74%), ossicular anomaly (n=19, 19%) and chronic otitis media (n=7, 7%). Overall, the pre-operative bone-conduction thresholds/air-conduction thresholds (BC/AC) thresholds were 32±14/58±18 dB HL and ABG were 26±11 dB while the postoperative BC/AC thresholds were 29±15/36±18 dB HL and ABG were 7±8 dB. The postoperative ABG was excellent in 77% and successful in 93%. The postoperative ABG was excellent in 82.4% and successful in 97.3% of otosclerosis, excellent in 78.9% and successful in 89.5% of ossicular anomaly, and excellent in 14.3% and successful in 57.2% for chronic otitis media. ABG significantly improved less in revision cases than in primary otosclerosis cases (p=0.006).
Conclusion
Stapes surgery is an effective method to improve hearing for various types of stapedial fixation. There was a difference in the degree of hearing improvement according to causative disorders.
서 론
등골 고정(stapedial fixation)은 선천적 혹은 후천적으로 나타날 수 있으며, 선천성 질환인 경우 다른 이소골 또는 내이 기형과 동반되거나 단독으로 발생한다. 후천적으로 등골 고정을 일으키는 원인 질환으로는 이경화증, 고실경화증 혹은 만성 중이 질환에서 염증 후 신생골 형성 등이 있다. 성인에서 등골 고정을 유발하는 가장 흔한 질환인 이경화증은 서양에서는 사후 부검 결과 약 2.5%-6.4%의 유병률이 보고되었다[1]. 1950년대 Shea [2]가 이경화증 환자에서 등골절제술(stapedectomy)을 시행한 이후 현대적 술식이 고안되었고 성공적인 청력 호전 결과가 입증되어 널리 사용되고 있다. 저자는 이경화증, 선천성 등골 고정을 포함한 이소골 기형 및 만성 중이 질환 등 여러 원인 질환으로 인한 등골 고정이 확인된 전음성 난청 환자에서 10년 이상 기간 동안 총 100귀에 대해 등골 수술을 적용, 상당한 청력 회복 및 술식의 안정성을 경험하여 등골 수술의 청각학적 결과를 분석하고 원인 질환 및 술식에 따른 청각 예후를 살펴보고자 한다.
대상 및 방법
2011년 6월부터 2021년 12월까지 교신 저자 1인(HJP)에 의해 등골 수술을 받은 100귀(86명)를 대상으로 하여 의무기록을 통해 후향적으로 분석하였다. 원인 질환의 진단, 수술 전후 청력변화 양상, 술식의 양상, 사용된 인공 삽입물(piston wire)의 길이 및 수술 후 합병증 등에 대하여 조사하였다. 남자는 29명(37귀, 37%), 여자는 57명(63귀, 63%)이었으며, 환자의 나이는 6세부터 80세까지로 평균 연령은 41.6세였다. 좌우 각각 50귀가 포함되었다(Table 1).
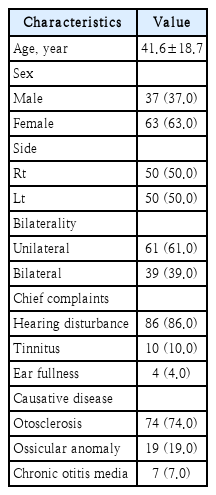
Clinical characteristics (n=100)
수술 전 환자의 병력 청취 및 측두골 전산화단층촬영 검사 소견, 수술 중 이소골의 형태, 등골의 운동성을 직접 확인하여 원인 질환을 진단하였다. 환자의 병력상 출생시부터 청력 저하를 동반한 경우 선천성 등골 고정에 합당한 것으로 판단하였으며, 정상 청력을 가졌던 성인이 서서히 진행하는 양상의 청력 저하를 호소하고 수술 중 등골의 운동성이 떨어져 있는 것이 확인되는 경우 이경화증으로 진단하였다. 또한 만성 중이염 진단하 과거에 유양동 삭개술 및 이소골 성형술을 시행한 이후 지속적인 전음성 난청을 보이는 환자에서 탐색적 고실 개방술 후 등골 고정이 확인된 경우 등골 수술이 시행되었다.
모든 환자는 국소마취하에 현미경을 이용하여 수술하였다. 이내접근(endaural approach) 후 고실외이도 피판(tympanomeatal flap)을 거상하고 등골 족판 및 등골근건의 충분한 노출을 위해 골성 외이도 후상방의 일부를 제거하였다. 미세가위(microscissors)를 이용하여 등골근건을 절제하고, crurotomy scissors 혹은 CO2 레이저를 이용하여 등골 후각을 절제하였다. 이어서 등골 전각을 골절시키고 등골의 상부 구조(suprastructure)를 제거하였다. 피스톤 와이어를 고정시킬 침골 장각 혹은 추골병의 내측부터 등골족판까지의 길이를 측정한 뒤, 이 길이에 등골 족판의 두께 및 전정 내로 진입할 길이를 고려하여 0.3-0.5 mm를 더한 값을 삽입물 길이(prosthesis length)로 사용하였다(Fig. 1). Skeeter drill을 이용하여 등골 족판에 개창술을 가한 후, 미리 길이를 재단해 둔 피스톤 와이어를 개창 부위에 위치시키고 침골 장각 또는 추골병 등에 crimper를 이용하여 고정하였다. 등골 족판의 개창술 부위를 연조직(soft tissue)을 이용하여 밀봉시켜 외림프액의 유출을 예방하였다. 고실외이도 피판을 복원 후 환자의 주관적 청력 호전을 확인하고 외이도를 젤폼(gelfoam)으로 채운 후 수술을 종료하였다.
Measuring the length of piston wire prosthesis (PWP). A: Measure the distance (①) from the medial side of the position (incudal long process or malleolar handle, marked with asterisk), where the PWP is to be fixed, to the stapes footplate to the stapedial footplate. B: The distance (②) indicates the sum of the thickness of the stapes footplate and the depth of insertion into the vestibule, which is approximately 0.3–0.5 mm, depending on the thickness of the footplate. The ‘prosthesis length’ (③) is determined by adding ② to ①. (①+②=③). The distance (④) means the diameter of the prosthesis.
대한이비인후과학회지에 발표된 수술 후 청력 결과 보고 표준 지침에 따라 수술 전후 청력 변화는 0.5, 1, 2, 3 kHz 네 주파수에서의 순음청력역치를 이용하여 계산하였다[3]. 3 kHz 골도청력역치를 측정하지 않은 경우 2 kHz와 4 kHz의 평균을 구하여 3 kHz를 대신하였다. 수술 후 결과 평가는 수술 후에 시행한 마지막 순음청력검사에서 기도골도청력차가 20 dB 이내인 경우를 성공적 청력 호전(successful hearing improvement), 10 dB 이내인 경우를 훌륭한 청력 호전(excellent hearing improvement)으로 정의하였다[4]. 수술 후의 골도청력역치가 수술 전의 골도청력역치보다 15 dB 이상 악화되었을 경우에 골도청력의 악화로 정의하였다. t-test 및 one-way ANOVA를 이용하여 p<0.05인 경우 통계적으로 유의하다고 판정하였다. 이 연구는 서울아산병원 Institutional Review Board의 승인을 받은 후 진행되었다(IRB No. 2022-0984).
결 과
본 연구에는 우측 귀 50예, 좌측 귀 50예가 포함되었으며, 총 39귀에서 양측성 전음성 난청을 보였다. 원인 질환으로 이경화증 74귀, 선천성 등골 고정을 포함한 이소골 기형 19귀, 만성 중이염 7귀가 확인되었다. 환자의 주증상은 난청이 가장 흔했으며(86%), 그 외 이명(10%), 이충만감(4%) 등을 호소하였다(Table 1). 술후 첫 청력검사는 평균적으로 수술 후 6주차에 시행되었으며, 최종 추적 관찰 기간은 평균 69.5±8.0주였다.
술식 및 인공 삽입물의 특징
93귀에서 등골절개술(stapedotomy)을 시행하였으며, 등골절개술을 시행하기 어렵거나 수술 중 우연히 등골 족판이 절제된 경우 등에서 총 7귀의 등골절제술(stapedectomy)이 시행되었다(Table 2). 술식에 따른 청력 호전 정도를 비교하였을 때 등골절개술을 시행한 그룹은 19.3±11.7 dB, 등골절제술을 시행한 그룹은 10.4±13.2 dB의 기도골도청력차의 변화를 보였으며 통계적으로 유의한 차이는 보이지 않았다.
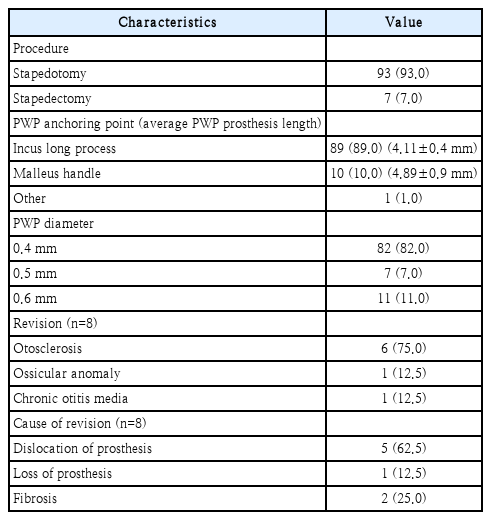
Surgical procedures and postoperative course (n=100)
총 89귀에서 침골 장각에 피스톤 와이어를 고정하였으며, 10귀에서 추골병에 삽입물을 고정하였다(Fig. 2). 피스톤 와이어의 길이는 피스톤을 거는 고리(hook) 부분을 제외한 길이(prosthesis length)를 기준으로 측정하였을 때 침골 장각에 고정한 경우 평균 4.11±0.4 mm, 추골병에 고정한 경우 평균 4.89±0.9 mm가 사용되었으며, 피스톤의 직경은 최소 0.4 mm부터 최대 0.6 mm가 사용되었고 평균 직경은 0.43 mm였다(Table 2). 수술 전후 기도골도청력차의 변화는 침골 장각에 고정한 경우 18.1±11.8 dB, 추골병에 고정한 경우 24.4±13.0 dB였으며, 피스톤 와이어의 고정 위치에 따른 청력 호전의 정도는 통계적으로 유의한 차이를 보이지 않았다. 만성 중이염으로 이전에 개방공동 유양동 삭개술 및 이소골 성형술을 시행받은 1예에서, 추골 및 침골이 모두 소실된 상태로 확인되어 피스톤 와이어의 고리 부분을 고정하기 위해 연골판(cartilage plate)을 제작하였다. 피스톤 와이어를 등골 족판 개창 부위에 위치시키고, 고리 부분이 고정된 상태의 연골판을 고막 피판 내측에 위치시켰다(Fig. 3). 이 증례에서도 수술 전 기도골도청력차가 40 dB에서 수술 후 17.5 dB로 감소하여 성공적인 결과를 보여주었다.

Incus and malleo-stapedotomy. A: According to the measured length, cut the piston wire prosthesis (PWP) (marked with red arrow) with 11th blade on the special cutting block. B: Intraoperative microscopic finding of left ear ‘incus stapedotomy.’ PWP is in place, fixed at the long process of incus (I, incus). C and D: ‘Malleo-stapedotomy’ in the left ear. If necessary, carefully bend the angle of the hook and fix it to the handle of the malleus (M, malleus). E: The shaft of PWP (marked with black arrow) should be placed perpendicular to the stapes footplate. F: Finally seal the stapedotomy opening with soft tissue (marked with black arrowheads).
Stapedotomy in a patient with chronic otitis media. As a result of previous tympanomastoidectomy (open cavity), the malleus and incus were missing, and the stapes footplate was fixed. To keep the piston wire prosthesis (PWP) in the stapedotomy site and the tympanic membrane, preventing it from being deeply inserted into the vestibule inadvertently, a cartilage plate (marked with black arrow) was prepared. A: PWP was inserted into stapedotomy opening through a hole in the cartilage plate. B: The hook of PWP and the cartilage plate was merged, and the cartilage was put under tympanomeatal flap.
수술 전후의 순음청력검사 결과
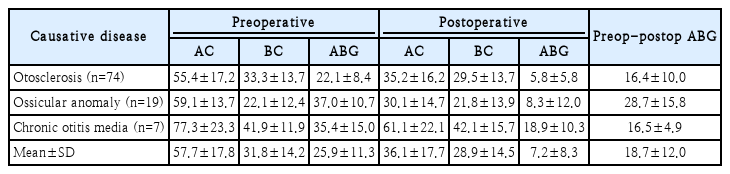
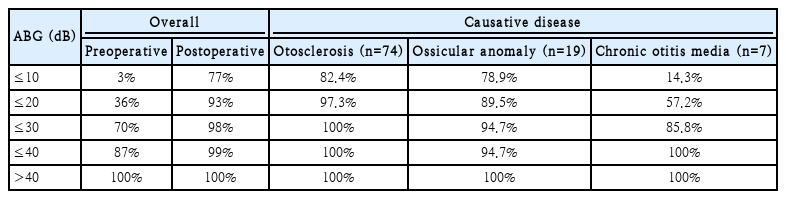
수술 전 골도 및 기도 청력 역치는 각각 31.8±14.2, 57.7±17.8 dB HL이었으며 기도골도청력차는 25.9±11.3 dB였다. 수술 후 마지막 추적 관찰 시 시행한 순음청력검사 결과, 골도 청력 역치는 28.9±14.5 dB HL, 기도 청력 역치는 36.1±17.7 dB HL이었으며 기도골도청력차는 7.2±8.3 dB였다. 평균 기도골도청력차는 18.7±12.0 dB 호전되었다(Table 3). 수술 후 기도골도청력차가 10 dB 이내로 감소한 훌륭한 청력 호전은 전체의 77%, 20 dB 이내로 감소한 성공적인 청력 호전은 전체의 93%에 해당하였다(Table 4). 난청의 양측성 여부와 청력 호전 정도에는 통계적으로 유의한 영향이 없었다. 수술 후 평균 6주차에 시행된 최초 청력 검사 결과와 최종적으로 시행한 청력 검사 결과를 비교하였을 때, 기도 및 골도 청력에 통계적으로 유의한 차이는 보이지 않았다(p=0.339, 0.666) (Fig. 4).
Preoperative and postoperative hearing results
Cumulative percentage of postoperative ABG (%)
Change of preoperative and postoperative air-conduction (AC) and bone-conduction (BC) pure-tone thresholds average over time. AC and BC pure-tone thresholds before and after the stapes surgery. The first follow-up examination was performed on average at 6 weeks after surgery. There was significant postoperative improvement of AC thresholds, preoperative average 57.6 dB to 36.8 dB. In the last pure-tone audiometry, at about 70 weeks after surgery, the AC hearing threshold levels were maintained without deterioration.
원인 질환에 따라 청력 호전 정도의 차이가 있는지 알아보았을 때 이소골 기형 그룹에서 기도골도청력차가 28.7±15.8 dB 호전되어 가장 큰 변화를 보였으며, 이는 이경화증 및 만성 중이염 그룹과 통계적으로 유의한 차이가 있었다(p<0.05) (Table 3). 수술 후 기도골도청력차가 20 dB 이내인 경우는 이경화증 그룹 97.3%, 이소골 기형 그룹 89.5%, 만성 중이염 그룹 57.2%로 만성 중이염 그룹인 경우가 가장 예후가 좋지 않았다(Table 4).
이경화증 그룹에서의 청력 호전 정도를 주파수별로 살펴보았을 때, 500 Hz에서 24.5 dB, 1 kHz에서 24.3 dB, 2 kHz에서 16.5 dB, 3 kHz에서 15.7 dB 만큼 네 주파수 모두에서 기도청력역치가 호전되었고, 골도 청력은 500 Hz를 제외한 나머지 세 주파수에서 수술 후 통계적으로 유의하게 호전되었다(p<0.05) (Fig. 5).
Preoperative and postoperative hearing threshold of otosclerosis cases (n=74). The results of the hearing test were analyzed in the patients with otosclerosis, which accounted for most of the cases. Postoperative air-conduction (AC) threshold was improved by 20 dB on average, statistically significantly at all frequencies including 0.5, 1, 2, and 3 kHz. Bone-conduction (BC) level was significantly improved at 2 kHz.
수술 후 합병증
선천성 등골 고정 의증하 등골절개술을 시행한 1예(1%)에서 수술 후 6주차에 시행한 첫 추적 관찰 시에 골도 청력이 수술 전보다 15 dB 이상 악화되었는데, 수술로 인해 기도골도청력차가 호전되어 병측의 수술 전 기도청력검사 결과와 수술 후 기도청력검사 결과가 차이가 나지 않아 최종 청력의 변화를 보이지 않았다. 환자는 수술 직후 어지럼 등 특이 증상을 호소하지 않았으며, Weber test상 병측으로 편측화되어 서서히 진행되어 초기에 발견되지 못한 난청으로 생각되었다.
2예(2%)에서 수술 후 보존적 치료에도 불구하고 어지럼 증상이 지속되어 각각 수술 후 5일차, 9일차에 탐색적 고실 개방술을 시행하였다. 외림프 누공이 의심되어 피스톤 와이어를 위치시킨 등골 족판의 개창 부위를 확인 후 연부 조직 등으로 보강하고 피스톤 와이어의 위치를 조정한 뒤 수술을 종료하였다. 수술 이후 환자들은 증상 호전되어 정상 퇴원하였고 기도골도청력차는 두 증례에서 모두 10 dB 이내로 감소하여 성공적인 청력 호전을 보였다.
등골수술 재수술
총 8귀는 재수술로서 등골 절개술이 시행되었다(Table 2). 이경화증 환자에서 일차 수술 및 재수술의 결과를 비교하였을 때, 수술 전후 기도골도청력차의 변화는 일차 수술 시 17.3±9.7 dB, 재수술 시 5.7±6.2 dB로 통계적으로 유의하게 재수술 시에 청력의 호전 정도가 감소하는 결과를 보였다(p=0.006) 재수술을 시행하기 전 평균 기도골도청력차는 20.6 dB였으며, 재수술 이후 최종 추적 관찰 시 기도골도청력차가 10 dB 이내인 경우가 5귀(62.5%), 20 dB 이내인 경우가 6귀(80%)였다. 재수술을 시행한 요인을 살펴보면 다음과 같다. 5귀(62.5%)에서 이전에 삽입한 피스톤 와이어가 헐거워져 있거나 부적절한 위치에서 확인되었으며, 1귀(12.5%)에서는 이전에 삽입한 피스톤 와이어가 소실되어 자연 배출된 상태로 생각되었다. 2귀(25%)에서 피스톤 와이어와 등골 족판 주위에 섬유화가 관찰되었다(Table 2).
고 찰
본원에서 지난 10년간 시행된 100예의 등골 수술의 결과를 분석하였을 때, 93%에서 기도골도청력차가 20 dB 이내인 성공적 청력 호전을 보여 이전에 시행된 대규모 연구들과 비슷한 결과를 보였다[5,6]. 전음성 난청의 원인 질환이 만성 중이염인 경우와 재수술인 경우에 환자의 청력 예후가 통계적으로 유의하게 나빴다. 한편, 난청의 양측성 여부와 술식의 종류(등골절제술과 등골절개술), 피스톤의 고정 위치(침골 장각과 추골병)는 청력 예후에 영향을 주지 않았다. 평균 약 70주의 추적 관찰을 시행하였을 때, 수술 후 최초 시행한 청력 검사와 최종적으로 시행한 청력 검사에서 기도골도청력차의 유의한 악화는 보이지 않고 호전된 상태를 유지하는 것으로 나타났다. 이는 숙련된 전문가가 등골 수술을 시행한 경우 장기간 추적 결과는 안정적으로 유지되는 것으로 보고된 바와 일치하였다[7].
등골 고정을 일으키는 원인으로는 선천성 등골 고정, 이경화증, 고실경화증 등이 있으며, 이 중 이경화증이 가장 흔한 원인 질환으로 알려져 있다. 이경화증에서의 등골 수술의 청력 호전 결과에 대한 국내의 연구들에 따르면 수술 후 기도골도청력차가 10 dB 이내인 경우는 64%-80%, 20 dB 이내인 경우는 67%-100%로 보고되었으며[3,8,9], 해외 연구 결과들에서는 10 dB 이내로 호전되는 경우를 약 76%-94%로 발표하였다[6,10,11]. 본 연구에서 이경화증 환자들의 수술 후 최종 청력 검사 결과를 분석하였을 때 기도골도청력차는 10 dB 이내 82%, 20 dB 이내 97%로 이전의 연구들과 비교하여 유사한 결과를 보였다.
등골 수술의 술식에 따른 결과에 대한 비교 연구는 다양하게 보고되었다. 등골절개술과 등골 절제술의 효과를 비교한 일부 발표들에서는 두 술식의 청력 호전 효과 및 합병증 발생률에 차이가 없다고 하였다[7,12]. 한편 등골절제술을 시행한 경우에 등골절개술을 시행한 경우보다 더 나은 기도 청력의 호전을 보고한 국내의 연구도 있었다[13]. 반면에 등골절개술을 시행하였을 때 고주파에서의 청력 호전 효과 및 장기간 청력의 안정성이 더 뛰어나다는 결과들이 보고되기도 하였다[14,15]. Cheng 등[16]이 그동안 발표된 두 술식의 결과를 비교한 여러 논문들을 요약하여 분석한 결과에 따르면 두 술식은 모두 전음성 난청의 해결에 효과적이고 안정적인 방법이나, 등골절개술이 특히 고주파에서의 청력 호전 효과가 좋고 합병증의 발생률이 낮기 때문에 일차 치료법으로 추천된다고 하였다. 저자 또한 등골절개술을 기본 술식으로 시행하고 있으며, 본 연구에서는 두 술식을 시행한 그룹 사이의 청력 호전 정도에 유의한 차이는 나타나지 않았다.
만성 중이염의 후유증으로 동반될 수 있는 고실경화성 등골 고정(tympanosclerotic stapes fixation)에 대한 처치 방법은 크게 두 가지로, 첫째로 등골 주위의 고실경화반(tympanosclerotic plaque)을 제거하여 등골 고정을 해소하는 것과 두 번째로 등골 수술이 있다. 적절한 술식에 대한 논란은 있으나, 전자의 경우 등골에 대한 조작으로 인한 술후 감각신경성 난청의 발생 가능성, 부유 족판(floating footplate), 외림프누공 형성 등의 합병증 가능성이 비교적 높은 것으로 보고되어 등골 절개술 혹은 등골 절제술이 추천된 바 있다[11]. 그러나 만성 중이염 환자에서는 중이강이 환기가 원활한 상태로 안정적으로 유지되는 경우에만 제한적으로 등골 수술을 고려할 수 있다[17]. 본 연구에서 이경화증, 이소골 기형 그룹과 비교하였을 때 만성 중이염 환자에서 수술 후 기도골도 청력차가 20 dB 이내인 경우는 57.2%로 낮은 청력의 호전을 보였으며 이는 약 50%-70%로 성공률을 보고한 이전의 연구 결구들과 유사하다[11,18].
소아에서 전음성 난청을 일으키는 선천성 등골 고정 또는 연소성 이경화증(juvenile otosclerosis)은 병리적으로는 서로 다른 질환이나, 소아에서 유사한 임상 양상을 보이면서 소아 등골 수술의 적응증이 되는 대표적인 질환들이다. 소아에서 철저한 병력 청취와 객관적, 연속적인 청력 검사는 불가능하여 두 질환을 명확히 감별하기는 어려우나 자세한 병력을 통해 선천적인지 진행성 난청인지를 확인하고, CT의 전형적인 이경화증 소견 혹은 수술 중 소견을 통해 원인 질환 추정이 가능하다. 본 연구에서는 18세 미만의 환자 총 17예를 포함하였고, 등골 족판 고정 14예, 이경화증 3예로 판단되었다. 선천성 이소골 기형 중 가장 흔한 형태인 등골 족판 고정은 2020년 미국에서 시행된 인구 기반 연구에 따르면 유병률이 약 100000명당 0.28명으로 보고되었다[19,20]. 원인 질환에 무관하게 소아의 등골 수술은 안전하고 효과적인 술식으로 알려져 있으며[21], 이전의 연구들에 따르면 연소성 이경화증 환아에서 선천성 등골 고정의 경우보다 등골 고정 수술의 결과가 더 좋은 것으로 보고되었다[22,23]. 등골 수술을 시행하기 적합한 소아의 연령은 최소 5세 이상, 어음인지역치가 35 dB 이상이고 기도골도청력차가 30 dB인 경우로 제시된 바 있다[24].
등골 수술의 가장 중요한 합병증으로 감각 신경성 난청의 발생이 있으며, 다양한 이전의 연구들에 따르면 0.5%-4.8%에서 발생하는 것으로 보고된다[5,13,25]. 본 연구에서도 1예(1%)에서 수술 후 감각 신경성 난청이 발생하였으나 기도골도청력차의 호전으로 인해 기도 역치의 차이를 보이지는 않았다. 이외에 등골 수술 이후 약 70%의 환자는 일시적인 어지러움을 호소하기도 하며, 수술 2-3일 이내에 보존적인 치료로 대부분 호전된다[26]. 등골 수술 이후 지속적 혹은 지연성으로 발생하는 어지럼의 경우 외림프 누공, 피스톤의 전정 내 진입 등을 의심할 수 있으며, 후자를 예방하기 위해서는 수술을 시행할 때 등골 족판 내측 0.2 mm 이내로 진입할 수 있도록 섬세한 길이 조절이 필요하다. 수술 후 5일 이상 어지럼 증상이 지속된 2예에서 탐색적 고실 개방술을 시행하여 등골 족판 개창 부위를 보강한 후 어지럼 증상 호전 및 청력의 성공적인 호전을 경험하였다. 수술 이후 7일 이상 어지럼 증상이 지속될 때 골도 청력에 나쁜 영향을 줄 수 있음이 보고된 바[27], 등골 수술 이후 환자의 어지럼 증상 여부를 면밀히 확인함과 더불어 증상 발생 시 적절한 개입이 이루어질 수 있도록 해야 한다.
등골 수술 재수술의 성공률은 경험이 많은 전문가가 시행한 경우에도 40%-70% 정도로, 일차 수술로 시행한 경우보다 상당히 낮은 결과가 보고되고 있으며, 수술 후 감각신경성 난청 혹은 어지럼 등의 합병증 발생 비율이 높은 것으로 보고되었다[28,29]. 본 연구에서도 재수술 이후 기도골도청력차가 10 dB 이내인 경우가 62.5%, 20 dB 이내인 경우가 80%로 기존 연구 결과와 유사하게 나타났다. 등골 수술의 재수술은 상당 기간의 경과 관찰 이후에 결정하게 되는데, 조절이 되지 않는 어지럼 혹은 안면 마비와 같은 응급 수술의 적응증이 아니라면 일차 수술 이후에 20 dB 이상의 기도골도청력차가 지속될 때 고려하게 된다. 일차 수술 이후 좋은 청력 결과를 보이던 환자에서 악화를 보이는 경우, 피스톤 위치의 변화, 동반된 침골 장각의 침식 및 육아조직, 섬유화의 형성 등을 의심할 수 있으며 실제로 본 연구에서 재수술의 요인을 확인하였을 때, 이전 수술 시 삽입한 이식물의 위치 변화가 가장 흔하게 확인되었다. 최근 150명의 등골 수술 재수술을 시행한 환자를 대상으로 한 연구에서 청력 결과에 영향을 주는 요인이 일차 수술 후 청력 호전 여부인 것으로 보고되었다[29]. 즉 일차 수술 이후에도 청력 결과가 나쁜 경우 재수술 후에도 나쁠 가능성이 높다는 것으로, 이는 등골 고정 이외의 요인이 동반되어 있을 가능성을 고려해야 함을 의미한다. 일차 수술 직후부터 충분한 기도골도청력차의 감소를 보이지 않는다면 등골 고정 이외에 제3의 창(third window) 혹은 추골의 강직 등 전음성 난청을 일으킬 수 있는 다른 요인이 동반되어 있는지를 확인해야 한다[30].
본 연구는 국내에서 비교적 드문 질환인 이경화증 74예와 더불어 이소골 기형 및 만성 중이염 환자에서 등골 수술을 적용, 청각 예후를 비교 분석한 연구로서 의의가 있을 것으로 생각한다. 본 연구의 제한점으로는 증례 수가 충분하지 않아 구체적인 수술 후 경과 시기별 청력 검사에 대한 분석은 시행하지 못한 점이다. 향후 지속적인 데이터 수집을 통해 등골 수술 후 환자의 청력 변화 양상에 대한 장기적 추적 관찰이 가능할 것으로 기대된다.
Acknowledgements
None
Notes
Author Contribution
Conceptualization: Hong Ju Park. Data curation: Se Eun Yi, Jun Yong Go. Formal analysis: Yun Ji Lee, Sang Hun Lee. Investigation: Sang Hun Lee, Seung Cheol Ha. Methodology: Hong Ju Park. Project administration: Sang Hun Lee. Supervision: Hong Ju Park. Validation: Hong Ju Park. Visualization: Yun Ji Lee, Dong Kyu Lee. Writing—original draft: Yun Ji Lee, Sang Hun Lee. Writing—review & editing: Yun Ji Lee, Hong Ju Park.