상악동 저류낭종의 치료 전략
Abstract
Retention cysts are commonly found in the maxillary sinus and are discovered incidentally on imaging studies. Obstruction of the ducts of the seromucous glands of the paranasal sinus lining is thought to induce the development of retention cysts. Since retention cysts are asymptomatic and tend to degenerate, they do not require definite treatment. However, in clinical practice, surgical treatment is often performed without clear indications. Retention cysts need to be surgically managed when accompanied with relevant clinical symptoms or with obstruction of the natural ostium, or when involving the ostiomeatal complex or the infraorbital nerve. Endoscopic sinus surgery has become the surgical procedure of choice for removing retention cyst. Therefore, it is important for rhinologists to understand the nature and behavior of this pathology so that unnecessary surgical intervention could be avoided.
Key words: Maxillary sinus ㆍ Retention cyst ㆍ Surgery
서 론
부비동 점막은 상피세포층, 기저막과 점막하고유층으로 구성되며 점막하고유층에는 분비선(장액선, 점액선), 혈관과 신경 등이 분포한다. 임상적으로 부비동 점막에서 (점액)저류낭종(mucous retention cyst)이라고 불리는 병변이 흔하게 발견되는데, 장액점액선의 분비관이 폐쇄되고 팽창되어 발생한다[ 1]. 급성 및 만성 부비동염의 병적 상태에서는 점막 염증이 분비관의 폐쇄를 유발할 수 있기 때문에 저류낭종이 더욱 쉽게 발생한다[ 2]. 저류낭종은 대개 무증상이기 때문에 부비동 단순 방사선 검사나 전산화단층촬영, 치과 영역의 파노라마 촬영 등에서 우연히 발견되는 경우가 많고, 진단은 주로 임상증상 및 영상학적 검사를 통해 이루어진다. 유병률은 다양하고, 주로 상악동에 많이 발생하며 나머지 부비동에는 드물다[ 3]. 시간이 경과하면 퇴화하는 저류낭종의 특성을 고려할 때, 대부분의 경우 경과 관찰만으로 충분하지만, 실제 임상에서는 뚜렷한 객관적인 적응증 없이 수술적 치료가 시행되는 것을 종종 볼 수 있다. 따라서 본 종설에서는 상악동 저류낭종의 임상적 특성 및 치료 전략에 대해 고찰해 보고자 한다.
본 론
정 의
저류낭종은 부비동 점막의 분비선에서 기원하여 연부 종괴 형태를 보이는 원형 또는 원개형(dome-shape)의 병변이다( Fig. 1). 부비동 점막에 발생하는 낭종은 보통 비분비성과 분비성으로 분류한다. 비분비성 낭종은 상피 내벽이 없고 염증 세포들이 침윤된 부종성의 결체 조직층으로 이루어지며, 분비성 낭종은 입방형의 섬모원주상피로 둘러싸인 점액 축적물로 이루어지며 저류낭종과 점액종이 해당된다[ 4]. Kim 등[ 5]은 상악동 저류낭종을 병리학적으로 유출형(extravasation type), 내강형(luminal type)과 혼합형(mixed type)의 세 가지로 분류하였고, 내강형이 가장 흔하게 발생한다. 유출형은 세포질에 호산구성 물질이 포함된 대식세포가 얇은 섬유 결체 조직 벽에 침착되고, 내강형은 점액성 물질로 내강이 가득 차 팽창된 것이 특징이다[ 5]. 부비동 점막 낭종은 이외에도 병인 기전에 따라 비부비동의 만성 염증상태에서 발생한 일차성과 외상 또는 의인성으로 발생한 이차성으로도 분류한다[ 6].
역 학
저류낭종의 유병률은 1.4%-35.6%로 다양하고 부비동 중 상악동에 가장 많이 발생하지만 이유는 밝혀져 있지 않다[ 1, 7]. 상악동 내벽 중에서도 하벽에 가장 흔하지만 외벽, 전벽, 상벽 등 어느 부위에서나 발생 가능하고 대개 일측성이며, 양측성은 16.6%에서 발생한다[ 1, 3, 7, 8]. 저류낭종은 20대와 남성에서 유병률이 높은 경향성은 있지만, 성별이나 연령과 유병률 간에 유의한 관련성은 없다[ 4].
병태생리
저류낭종은 급성 또는 만성 비부비동염, 알레르기비염, 비부비동 또는 상악-안면 부의 외과적 처치, 안면 외상 및 비부비동 종양 등에서 발생하며, 부비동 점막에 존재하는 장액점 액선의 분비관이 폐쇄되면 분비관이 팽창되면서 저류낭종이 발생한다[ 1]. 저류낭종의 함유물에는 높은 수치의 면역글로불린 및 보체, 항단백효소가 존재하여 염증성 병인을 반영한다[ 9]. 하지만 상악동염과 상악동 저류낭종의 분비물을 비교해 보면 상악동염에서는 염증성 사이토카인과 항균 단백질이, 그리고 상악동 저류낭종에서는 점막 보호 단백질이 상대적으로 높게 검출되어 상악동염과 상악동 저류낭종은 다른 병인 기전으로 발생한다[ 10]. 비흡연자에 비해 흡연자에서 유의하게 유병률이 높은 것도 흡연으로 인한 전염증 상태와 연관이 있지만, 치원성 감염과 치성 낭종은 상악동 저류낭종과는 유의한 관련성이 없다[ 11, 12].
임상 양상 및 경과
저류낭종은 대개 무증상이지만 부비동 내의 위치, 크기, 부비동 입구의 폐색 여부, 신경 구조물의 침범 여부에 따라 감각이상, 어지러움, 안면부 통증이나 압박감, 농성 콧물, 코막힘, 후비루 등의 증상이 나타난다. Choi 등[ 13]이 상악동 저류낭종을 3년 이상 장기 추적 관찰한 10예 중 10%는 특이 증상 없이 크기가 2배 이상 증가하였지만, 90%는 자연 소실되거나 유의한 크기 변화가 없었고 Casamassimo와 Lilly [ 14]가 34예의 저류낭종에 대해 평균 10개월간 추적 관찰한 결과에서도 15%에서만 크기가 증가하고, 24%에서는 크기가 감소 또는 소멸하고, 나머지 61%에서는 크기 변화가 없었다. 따라서 환자가 특이 증상 없이 우연히 저류낭종으로 진단되면 저류낭종의 양성 경과에 대한 적절한 교육을 통해 환자의 불안을 완화하고 안심시켜주는 것이 중요하다.
영상 진단
부비동 전산화단층촬영(CT)은 저류낭종을 진단하기 위한 가장 정확한 검사로, 상악동 전체를 차지할 만큼 크기가 큰 낭종을 단순 방사선검사에서 부비동염이나 상악동 종양과 구별하기 어려울 때에 유용하다. 자기공명영상검사(MRI)는 부비동의 염증성 병변에 대해 일차적으로 사용되는 검사는 아니지만, 비부비동 외의 질환을 평가하기 위해 촬영한 자기공명영상검사에서 우연히 저류낭종이 발견될 수 있다. 저류낭종은 영상 의학적 검사에서 균일한 원개형의 낭성 종괴, 바깥쪽 경계는 뚜렷하고 자유 연은 부드러운 구형, 골 파괴의 부재, 치근부와 연결점이 없는 특징을 보인다[ 8]. 또한 저류낭종은 부비동 전산화단층촬영과 자기공명영상검사에서 조영 증강이 되지 않고, 전산화단층촬영에서는 저음영을 보이고, 자기공명 영상검사에서는 T1-강조영상에서 다양한 신호 강도와 T2-강조영상에서 고신호강도를 보인다( Figs. 2 and 3).
감별 진단
부비동의 저류낭종과 감별해야 할 질환에는 치성 낭종, 악성 종양과 점액종 등이 있다[ 15]. 치성 낭종의 경우 영상 의학적 검사에서 치근부와의 연결부를 확인하여 감별할 수 있으며, 악성 종양은 골 파괴를 동반하는 것이 일반적이다. 저류낭종의 가장 중요한 감별진단인 점액종은 장액점액선의 분비관이 막혀 발생하는 저류낭종과 달리 부비동의 자연공이 폐쇄되어 발생하며 일반적으로 외과적 처치가 필요하다. 점액종은 대부분 전두동이나 사골동에서 발생하고 주로 안구 증상을 호소하는데, 영상 의학적 검사에서 골 파괴는 드물지만 골 팽창 및 재형성 소견이 흔히 관찰된다( Table 1) [ 16]. 상악동 저류낭종은 드물게는 부자연공을 통해서 후비공으로 돌출하기도 한다[ 17, 18].
치 료
대부분의 저류낭종은 자연히 퇴화하기 때문에 증상이 없는 환자는 정기적인 경과 관찰과 보존적 치료만으로도 충분하다. 저류낭종이 상악동 자연공을 막을 때, 낭종이 상악동 밖으로 나와 부비동 개구복합체(ostiomeatal complex)를 막을 때, 낭종이 상악동의 50% 이상을 차지하면서 연관된 증상이 있을 때, 그리고 하안와신경 주변의 낭종이 감각이상 또는 통증을 유발할 때에는 수술의 적응증이 된다[ 1]. 그 외에도 진단 당시 크기가 2 cm 이상이거나 양측성인 저류낭종은 크기가 커질 수 있는 확률이 높아 정기적인 추적 관찰을 통해 수술적 치료 여부를 결정한다[ 3]. 저류낭종은 과거에는 하비도 또는 자연공을 통해 천자 및 흡입을 하거나 Caldwell-Luc씨 접근술을 통해 낭종을 제거하였지만 최근에는 내시경을 이용한 낭종 적출 또는 부비동 내시경 수술을 통한 낭종조대술이 주된 치료 술식이며, 다양한 각도의 내시경을 적절히 사용하면 상악동 내 관찰 시야를 넓혀 재발을 줄일 수 있다.
상악동 개방술의 범위는 낭종 원발부의 크기 및 위치에 따라 달라지는데, 중비도 개창술(middle meatal antrostomy)을 통한 제거는 잔여 병소를 남길 가능성이 높지만, 하비도 개창술(inferior meatal antrostomy)로 접근 시 중비도 개창술로 확인할 수 없는 부위까지 저류낭종의 제거가 가능하다. Lou [ 19]는 하비도 개창술과 기저 점막 소작술을 함께 시행하면 중비도 개창술만으로 수술하는 것보다 수술 시간이 짧고, 재발이 적다고 하였다. 다양한 수술을 통해 저류낭종 내 압력이 감소하면 임상 증상이 호전되지만, 수술 방법에 따른 증상 호전 정도는 유의한 차이가 없다[ 19]. 부비동 내시경수술 후 재발률은 약 3% 정도이며, 과거 Caldwell-Luc씨 접근술을 통한 수술 후에는 술후 안면부종, 협부 불편감, 안면 및 치아 감각이상, 술후성 협부낭종 등의 합병증이 발생했지만 부비동 내시경 수술은 이러한 합병증의 발생이 적다[ 20]. 이 외에도 상악동 풍선확장술이나 연성내시경을 이용한 접근법이 보고되어 있지만 부비동 내시경 수술(경성)에 비한 이점에 대해서는 추가적인 비교 연구가 필요하다.
결 론
상악동 저류낭종은 임상적으로 흔하게 발견되지만 대부분 무증상인 질환으로, 다양한 영상 의학적 검사를 통해 우연히 진단된다. 저류낭종은 시간이 경과하면 퇴화하는 경우가 많기 때문에 보존적 치료가 원칙이며, 임상 증상이 있는 경우, 부비동 자연공을 막거나 부비동 개구복합체의 병변인 경우, 또는 임상 증상이 동반된 하안와신경의 병변인 경우에는 수술적 치료의 적응증이 된다( Fig. 4). 수술적 치료 원칙은 부비동 내시경 수술을 통한 제거 또는 조대술이며, 임상의는 저류낭종의 임상경과와 특성을 정확히 이해하여 환자에게 저류낭종의 양성적인 임상 경과에 대한 충분한 설명을 통해 환자를 교육하는 것이 중요하며, 불필요한 수술을 피하는 것이 필요하다.
Fig. 1.
Nasal endoscopic finding of retention cysts. A: Large retention cyst protruding from the left maxillary sinus ostium. B: Retention cyst originating from the lateral wall of left maxillary sinus. C: Retention cyst protruding from the right middle meatal antrostomy. Yellow asterisk: retention cyst. 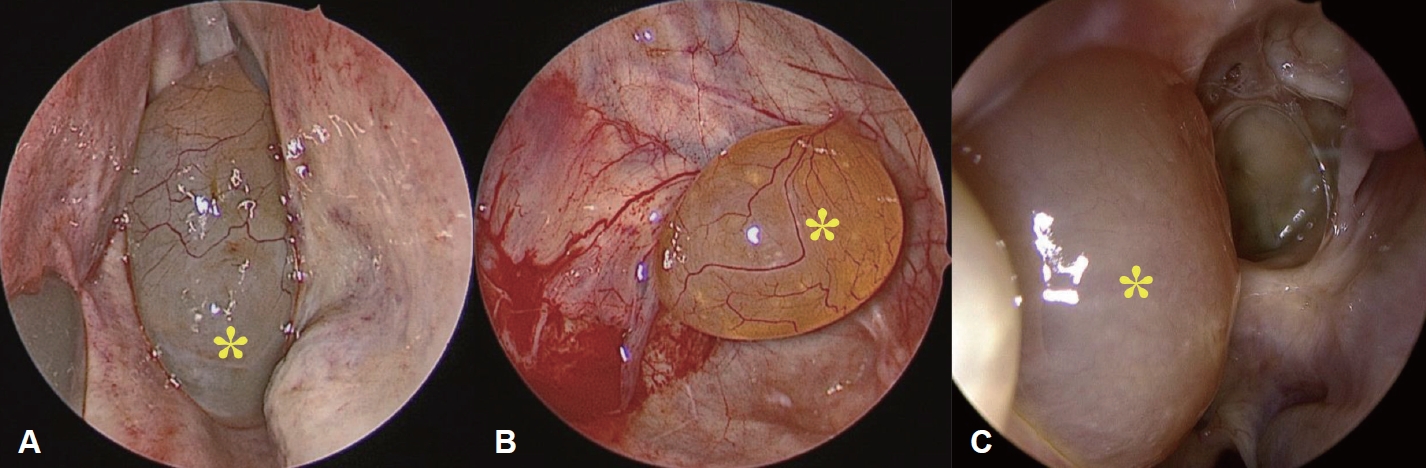
Fig. 2.
Various locations of maxillary retention cyst on paranasal sinus CT. A-C: Coronal view. D-F: Axial view. 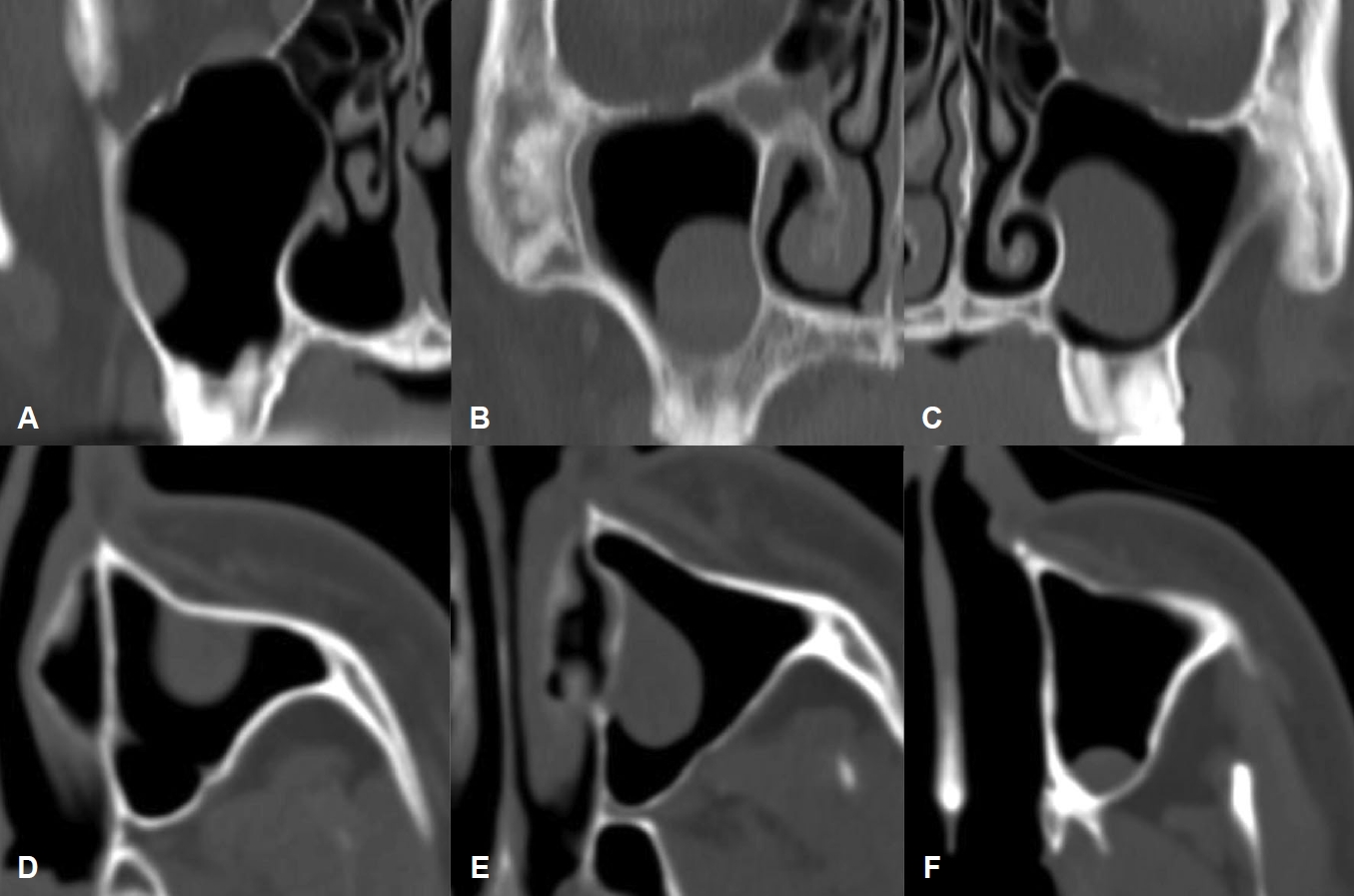
Fig. 3.
Paranasal sinus MRI of retention cyst fully occupying maxillary sinus. High signal on T1 (A: coronal view), T2 (B: coronal view, C: axial view). 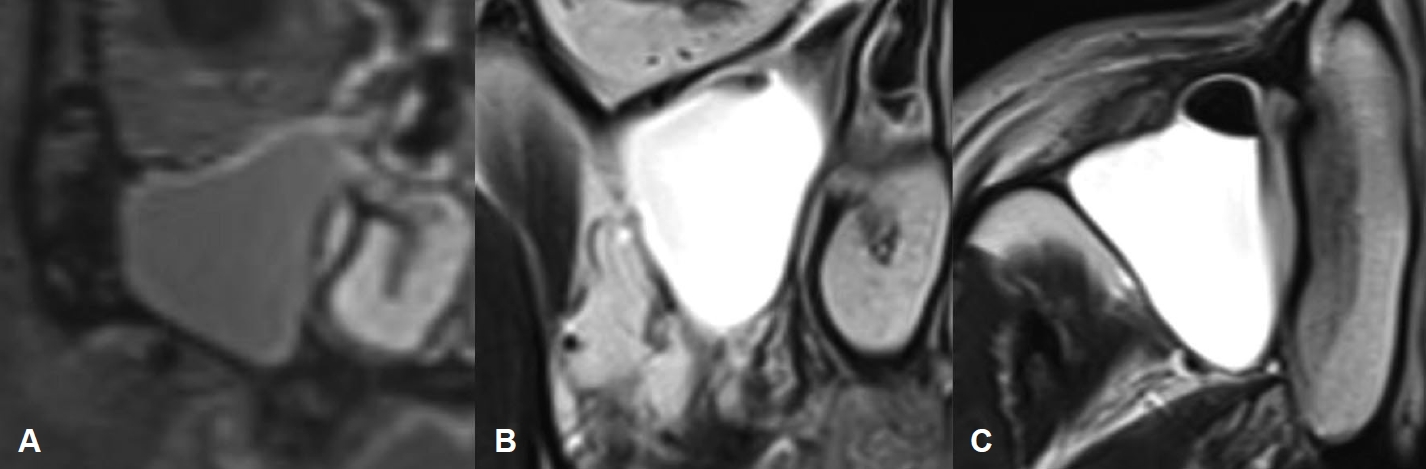
Fig. 4.
Clinical algorithm for retention cyst of paranasal sinus. 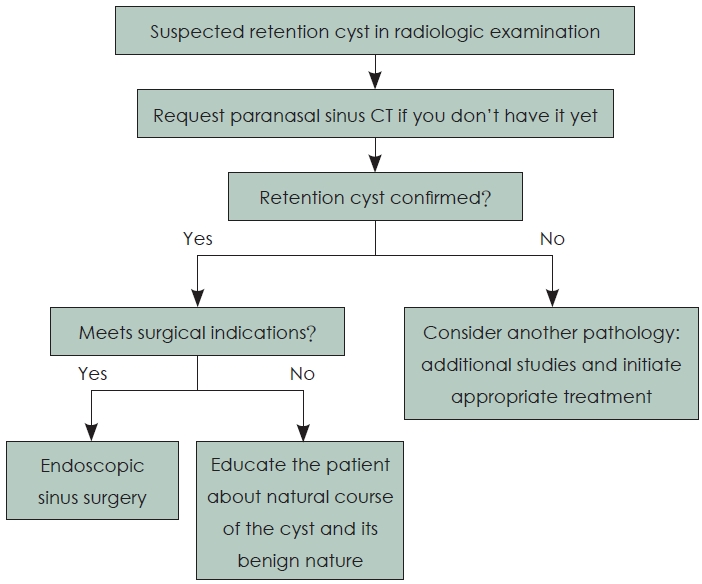
Table 1.
Comparison between retention cyst and mucocele of maxillary sinus
|
Retention cyst |
Mucocele |
|
Clinical features |
Mostly, incidental radiographic finding |
Osteomeatal complex obstruction: chronic rhinosinusitis |
|
Generally asymptomatic (except in case of big size) |
Signs and symptoms: pain, swelling, nasal obstruction, nasal discharge |
|
Variable size, can be bilateral |
Occasionally infection (mucopyocele) |
|
Normally, no treatment required |
Surgical treatment required |
|
Radiologic characteristics |
Rounded, cupuliform or “rising sun” shape |
Radiodense, uniform density, expansive growth |
|
Initial stage, mucosal thickening shape |
Aggressive lesion appearance |
|
Uniform radiodensity with clear limits |
Significant bone resorption |
|
Underlying bone structure preserved |
Can spread to adjacent structures |
|
No bone resorption or expansion |
|
|
Pathologic findings |
Epithelium-lined, cystic structure |
Cyst lining of respiratory epithelium |
|
Accumulation of inflammatory fluid accumulation |
Mucous content |
REFERENCES
1. Albu S. Symptomatic maxillary sinus retention cysts: should they be removed? Laryngoscope 2010;120(9):1904-9.   2. Verdugo VI. [Presence of mucous retention cysts in the maxillary sinus, CUENCA - ECUADOR, 2016-2017]. Odontología Activa Revista Científica 2019;4(3):9-14, Spanish.
3. Jaramillo-Moncayo C, Herrera JL, Ospina J. [When should retention cysts in paranasal sinuses be operated? Literature review]. Acta de Otorrinolaringología & Cirugía de Cabeza y Cuello 2021;50(1):78-84, Spanish.
4. Schuknecht HF, Lindsay JR. Benign cysts of the paranasal sinuses. Arch Otolaryngol (1925) 1949;49(6):609-30. 5. Kim YS, An KY, Lee SK. Pathological findings for mucous retention cyst in maxillary sinus. Korean J Oral Maxillofac Pathol 2010;34(1):9-18.
6. Morikawa-Saito M, Kuyama K. A histopathological study of mucous cyst of the maxillary sinus. Int J Oral Med Sci 2013;11(3):163-71. 7. Bósio Bósio, Tanaka O, Rovigatti E, de Gruner SK. The incidence of maxillary sinus retention cysts in orthodontic patients. World J Orthod 2009;10(2):e7-8. 8. Bhattacharyya N. Do maxillary sinus retention cysts ref lect obstructive sinus phenomena? Arch Otolaryngol Head Neck Surg 2000;126(11):1369-71. 11. Rodrigues CD, Freire GF, Silva LB, Fonseca da Silveira MM, Estrela C. Prevalence and risk factors of mucous retention cysts in a Brazilian population. Dentomaxillofac Radiol 2009;38(7):480-3. 12. Niknami M, Mirmohammadi M, Pezeshki A. Evaluation of the prevalence of mucous retention pseudocyst and its correlation with the associated risk factors using panoramic radiography and conebeam computed tomography. J Dent (Tehran) 2018;15(2):123-9.  13. Choi SM, Wang JH, Chung YS, Jang YJ, Lee BJ. The long term fol low-up of ma x il la r y si nu s ret ent ion cyst. Korea n J Otorhinolaryngol-Head Neck Surg 2003;46(7):572-4.
14. Casamassimo PS, Lilly GE. Mucosal cysts of the maxillary sinus: a clinical and radiographic study. Oral Surg Oral Med Oral Pathol 1980;50(3):282-6. 15. Demicheri G, Kornecki F, Bengoa J, Abalde H, Massironi C, Mangarelli Garcia C, et al. Maxillary sinus mucocele: review of case report. Odontoestomatología 2016;18(27):55-63.
17. Berg O, Carenfelt C, Sobin A. On the diagnosis and pathogenesis of intramural maxillary cysts. Acta Otolaryngol 1989;108(5-6):464-8. 18. Frosini P, Picarella G, De Campora E. Antrochoanal polyp: analysis of 200 cases. Acta Otorhinolaryngol Ital 2009;29(1):21-6. 20. Hadar T, Shvero J, Nageris BI, Yaniv E. Mucus retention cyst of the maxillary sinus: the endoscopic approach. Br J Oral Maxillofac Surg 2000;38(3):227-9.
|
|














