Introduction
Tonsillar hypertrophy is a common clinical finding in the otolaryngology outpatient clinic, but hypertrophy due to distant metastatic cancer is known to be very rare, and according to the literature, the proportion of metastatic tumors among malignant tonsillar tumors is low at less than 1%. Among these, metastatic tonsillar cancer originating from lung cancer has been reported to be extremely rare [1]. Most tumors metastasizing to the tonsil originate from renal cell carcinoma and small cell lung cancer, and tonsillar metastasis of non-small cell lung carcinoma (NSCLC) is very rare [1,2]. In most cases, tonsillar metastasis of NSCLC is confirmed during treatment after a diagnosis of lung cancer when tonsillar hypertrophy develops [3], and as in this case, there have been almost no reports in which lung cancer was discovered during evaluation of the primary site after a patient presented with tonsillar hypertrophy as the initial symptom [4].
In this case, we report a very rare case in which NSCLC was ultimately diagnosed in a patient who presented with a tonsillar mass, together with a review of the relevant literature.
Case
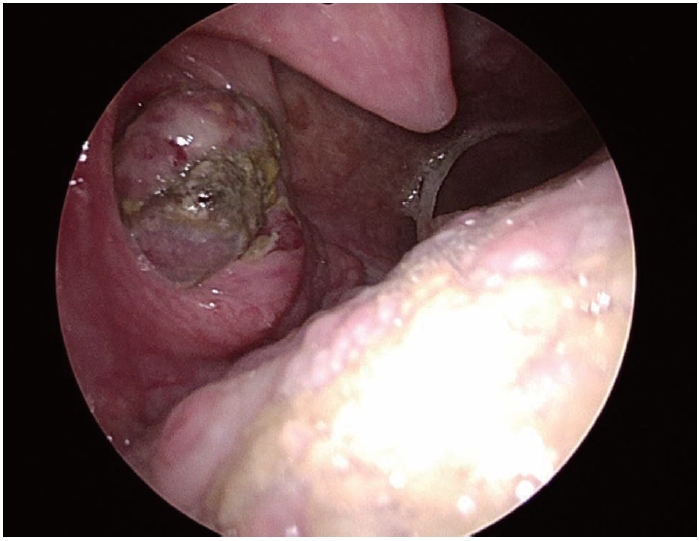
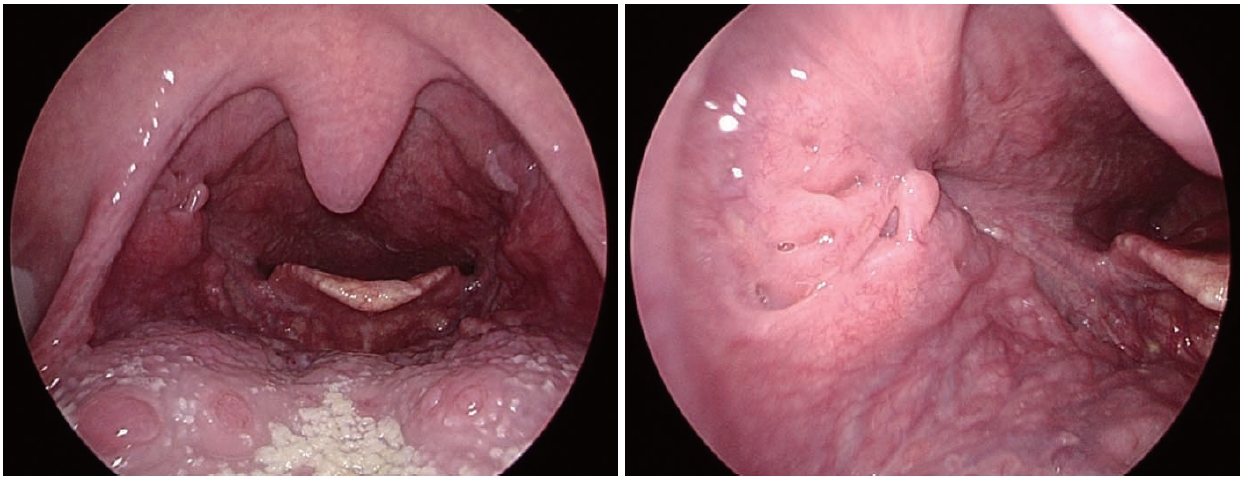
A 54-year-old man presented to a local clinic with a 2-week history of throat foreign-body sensation and blood-tinged saliva. On physical examination, an oval ulcerative lesion was observed on the right tonsil, and biopsy suggested pleomorphic sarcoma or a poorly differentiated malignant tumor, and he was referred to the otolaryngology department of our hospital (Fig. 1). There was no history of alcohol use, and he had a smoking history of half a pack per day for more than 30 years. He had no notable medical history other than hyperlipidemia.
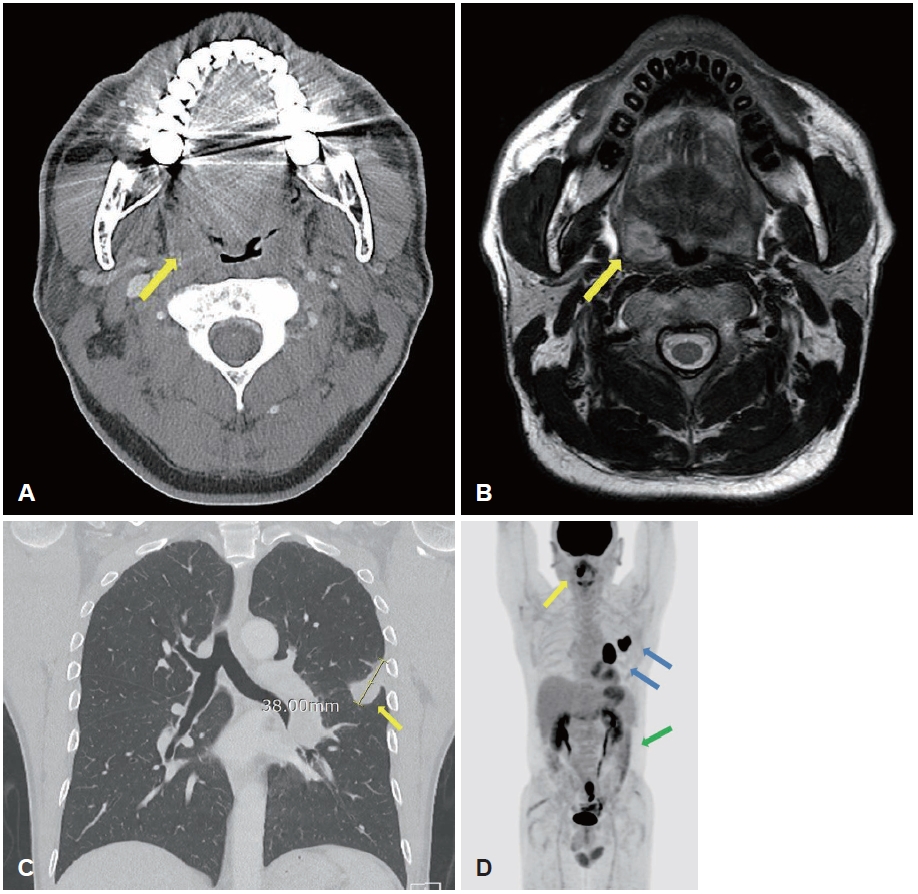
Contrast-enhanced neck CT showed a peripherally enhancing lesion with central low attenuation (1.8 cm) in the right palatine tonsil (Fig. 2A), and neck MRI showed a lobulated mass (2.3 cm) at the same site with low T1 signal intensity and intermediate T2 signal intensity (Fig. 2B). There was no local invasion and there were no notable findings in the cervical lymph nodes.
For staging and treatment planning under suspicion of a primary tonsillar malignancy, chest CT revealed a 3.8 cm lobulated mass extending across the left major fissure and pleura (Fig. 2C) and a 4.3 cm enlarged lymph node in the left hilum. PET-CT demonstrated fluorodeoxyglucose-avid lesions in the right tonsil (SUVmax 21.64), left lower lobe lung (SUVmax 26.41), left hilum (SUVmax 29.64), and small intestine (SUVmax 16.55) (Fig. 2D).
Endobronchial ultrasound-guided transbronchial needle aspiration of the pulmonary lesion was performed, confirming NSCLC. Molecular testing showed no EGFR or ALK alterations, PD-L1 (SP263) expression was 60%, and KRAS mutation and ROS-1 rearrangement were negative. Next-generation sequencing did not identify any clinically significant (Tier I) alterations.
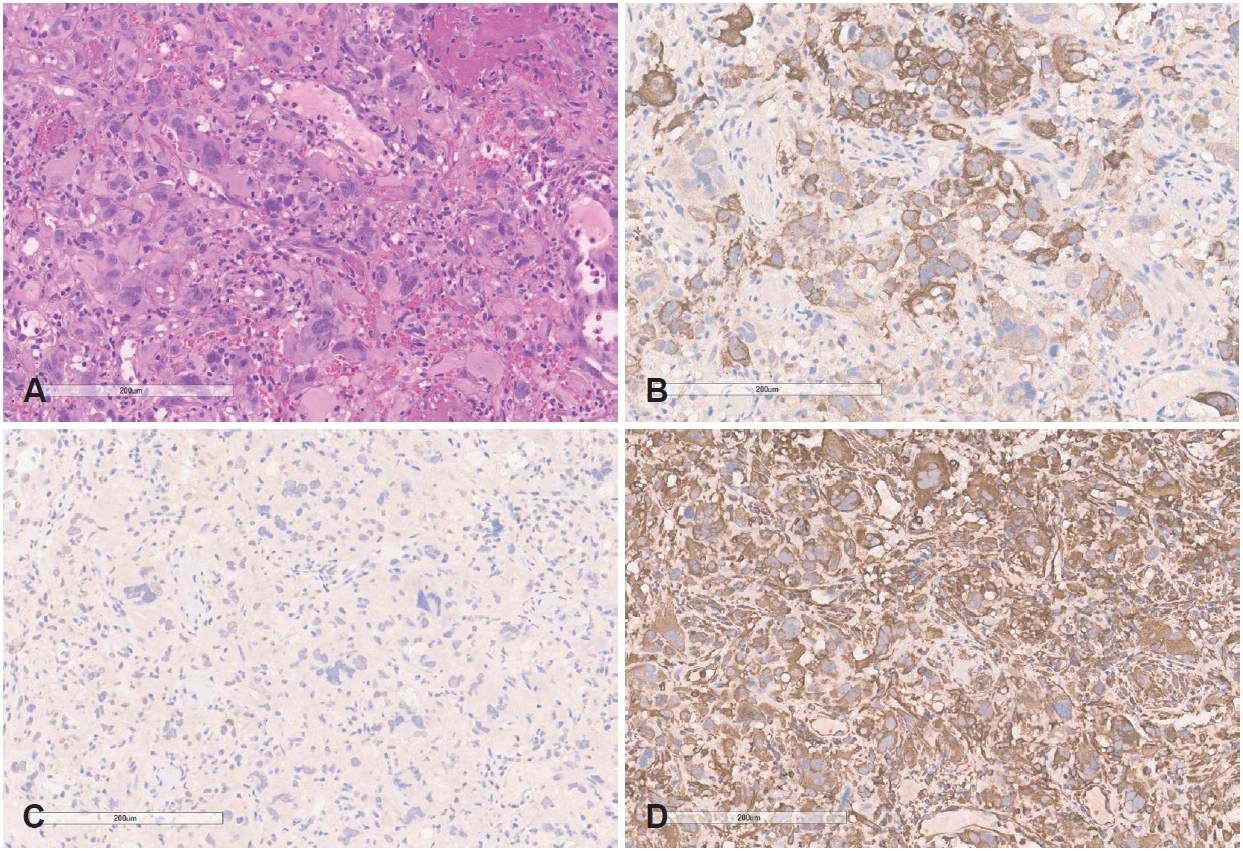
Because a separate primary malignancy of the tonsil was considered, tonsillar biopsy was repeated at our hospital, and poorly differentiated carcinoma consistent with metastatic NSCLC with morphology identical to the lung and mediastinal lymph node lesions was observed. On immunohistochemistry, pancytokeratin was positive and P40 was negative, making primary squamous cell carcinoma of the tonsil unlikely. Vimentin showed focal expression, but according to the pathology interpretation, this did not indicate sarcoma and was interpreted as being related to sarcomatoid features that can be seen in poorly differentiated carcinoma. Based on this immunophenotype and the morphologic similarity to the lung lesion, the lesion was ultimately reported as metastatic disease originating from the lung (Fig. 3). Accordingly, after integrating radiologic and histologic findings, the final diagnosis was tonsillar metastasis originating from the lung.
During staging evaluation, the patient developed small bowel intussusception and underwent small bowel resection. Pathology showed poorly differentiated carcinoma consistent with metastatic NSCLC, identical to the tonsillar biopsy, and this was also determined to be distant metastasis. Pembrolizumab (Keytruda, 200 mg, intravenous infusion, every 3 weeks) was administered, and to improve dysphagia and dyspnea due to the tonsillar tumor, radiotherapy to the tonsillar tumor was performed (quad shot, 3.7 Gy×4 delivered twice daily over 2 days, repeated at 4-week intervals).
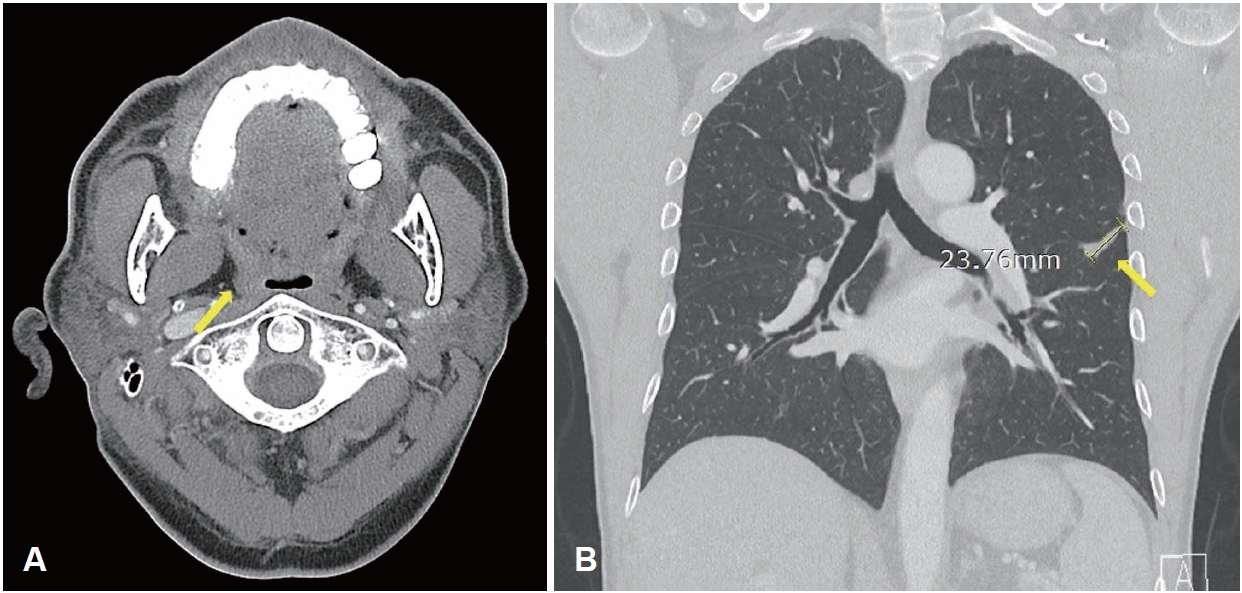
After the second course of radiotherapy during treatment, neck CT showed disappearance of the right tonsillar lesion, and radiotherapy was concluded while immunotherapy was continued. After three cycles of immunotherapy, neck CT showed no residual lesion in the right tonsil (Fig. 4A), and chest CT showed marked reduction in the size of the left primary lung cancer and the metastatic hilar lymph node (Fig. 4B). Abdominal CT also showed resolution of the small bowel lesion previously identified. On outpatient endoscopic re-evaluation, the ulcerative mass previously observed in the right tonsil had resolved and no active mass was identified (Fig. 5). The patient is currently being followed while maintaining immunotherapy.
Discussion
Although the tonsil is a structure with abundant blood supply, metastasis from distant organs is known to be very rare, and major primary sites include cutaneous melanoma, kidney, lung, gastrointestinal tract, and breast [1,5].
The metastatic route to the tonsil has not yet been clearly elucidated, but because the tonsil lacks afferent lymphatics, hematogenous metastasis is considered the main mechanism rather than the typical lymphatic pathway [1,4,6]. This case also showed multiple metastases to the tonsil and small intestine along with radiologic and pathologic characteristics of the primary lung lesion, suggesting the possibility of hematogenous metastasis.
In distant metastasis, NSCLC commonly metastasizes to the brain, liver, adrenal glands, and skeletal system [7], and head and neck and gastrointestinal metastases are relatively rare. In this case, the tonsillar lesion was observed first, and subsequently, symptoms of intussusception and obstruction due to small bowel metastasis developed.
When a tonsillar mass is identified, tonsillar cancer, lymphoma, and chronic inflammation are generally considered first [8], and the possibility of distant metastasis is often assessed as low. However, as in this case, when the initial biopsy result is nonspecific or the diagnosis is not clear, re-evaluation of the lesion is necessary along with systemic staging evaluation.
From a treatment perspective, tonsillar metastasis is already classified as advanced metastatic disease, and systemic chemotherapy rather than local resection is the main treatment [9]. Some studies have reported cases of prolonged survival with targeted therapy in patients with molecular markers such as EGFR mutation or ALK rearrangement [5,10], but in most cases the prognosis is poor. In this case, the patient is receiving immunotherapy, but careful follow-up is required regarding prognosis due to the presence of multiple metastases.
In addition, in this case, palliative radiotherapy using the quad-shot regimen was performed to alleviate dysphagia and foreign-body sensation due to tonsillar metastasis, and it was judged to have contributed to symptom improvement within a short period. While systemic chemotherapy is the cornerstone of treatment for metastatic NSCLC, this short-course hypofractionated radiotherapy may be used as an adjunctive treatment in patients with local symptoms due to tonsillar metastasis [1,11].
This case represents a situation in which nonspecific symptoms beginning with a tonsillar mass were found to be a rare metastasis from a primary lung cancer. The local symptoms caused by the tonsillar mass appeared as the initial clinical manifestation, and primary lung cancer was diagnosed through systemic evaluation based on this clue, which gives this case clinical significance distinct from prior reports, and suggests that clinicians should consider the possibility of distant metastasis in the differential diagnosis process for tonsillar masses.
In addition, a conclusion of metastatic disease of lung origin was reached by integrating detailed pathologic analysis including immunohistochemistry performed at our hospital, biopsy of the pulmonary lesion by pulmonology, and repeated tonsillar biopsy by otolaryngology. This diagnostic process is an important example demonstrating that in atypical cases that are difficult to interpret based on a single pathologic finding, accurate diagnosis and appropriate treatment planning require close multidisciplinary collaboration along with radiologic and pathologic evaluation.