ì ëĄ
ì 늏íŒíì ìŽì©í ìŹê±Žì ì ìë°ë¶ì êŽëČìí ì ê±° ìŽí íŒë¶ ìŽììŽë ê”ì íŒíìŒëĄ êČ°ìë¶ë„Œ ìŹê±Žíêž° ìŽë €ìž ì ëëĄ êČ°ìë¶ì íŹêž°ê° íŽ êČœì° íìí ìŹê±Žì ìŽë€. íčí ê”Źê°ì ìì ìŽíì ìŹê±Žì ìêł ì ì°í íŒíì ìíë©° ë°ì, ì ì, êž°ë 볎ížì ê°ì ê”Źê°ì êž°ë„ì ê°ë„í ëłŽìĄŽíìŹìŒ íêž° ë돞ì êł ë €í êČìŽ ë§ì ìŹê±Žì ìŽë€[1]. ëêČœë¶ì íŽë¶íì ë° êž°ë„ì íčì±ì êł ë €í ìŽìì ìž íŒíì ìêČ ìŹëš ê°ë„íë©Žìë ì ì°íìŹ ë€ìí ëȘšììŒëĄ ìŹëší ì ììŽìŒ íë©° 충ë¶í íêŽêČœì êžžìŽë„Œ í볎íë©Žì êł”ìŹë¶ì êČ°ìì ì”ìííìŹìŒ íë€[2]. ìŁŒëĄ ìŹì©ëë ëíì ìž íŒíìŒëĄë ì ìžìžĄëíŽ ì 늏íŒí(anterolateral thigh free flap)êłŒ ìêłšì ì ì 늏íŒí(radial forearm free flap)ìŽ ìë€[3,4]. ì ìžìžĄëíŽ ì 늏íŒíì êČœì°, ꞎ íêŽêČœì ê°ì§ 충ë¶í ë¶íŒì ìĄ°ì§ì ì±ì·š ê°ë„íë©Žìë ìŒì°š ëŽí© ë° ì í êł”ìŹë¶ì í©ëłìŠìŽ íŹì§ ìë€ë ì„ì ìŽ ìì§ë§, ê”Źê°ì ìŹê±Žì ì ìŽì©íêž°ìë ë¶íŒê° í° êČœì°ê° ë§ìŒë©° íŒíêłŒ ìíë¶ ê°ì ìì ë¶ìŒìčë 돞ì ê° ëë€[4-8]. ìêłšì ìíŒíì êČœì°, ìêł ì ì°íìŹ ê”Źê°ì ìŹê±Žì ì í©í íŒíìŽì§ë§, êł”ìŹë¶ì ëŽí©ì ìíŽ íŒë¶ìŽììŽ íìíë©° êČ°ììŽ ëë ·íêČ ëłŽìŽë ëšì ìŽ ìë€[9-11]. ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒí(medial sural artery perforator free flap)ì ì ìžìžĄëíŽ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíì ëšì ì 볎ìíêł ì„ì ì êČ°í©í ëêČœë¶ ìŹê±Žì ììŽ ìŽìì ìž íŒíìŒëĄ ìŹëŹ 돞íìì ëłŽêł ëìë€[10,12-16]. íì§ë§ íê”ìžìì ëêČœë¶ ìŹê±Žì ìí íŒíìŒëĄìì ì ì©ì± ë° ìŽì êČ°êłŒì ëí ë°íë ëłž ì°ê”Źê° ìČììŽë€. ëłž ì°ê”Źë„Œ í”íŽ íê”ìžìì ëêČœë¶ì ì ì í ìŹê±Žì ììŽ ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ì ì©ì±êłŒ ì í êČ°êłŒì ëíŽ ììëłŽêł ì íë€.
ëì ë° ë°©ëČ
ë ì
ëłž ì°ê”Źë ë¶ëčììžëíê”ëłììì 2018ë
10ì~2019ë
7ìêčì§ ìíë ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ìŽì©í ìŹê±Žì ì ë°ì 8ëȘ
ì íìë„Œ ëììŒëĄ íí„ì ìŒëĄ ì§íëìë€(IRB No. B-1908-561-110). ìëŹŽêž°ëĄì í”íŽ íìë€ì ëìŽ, ì±ëł, êž°ì ì§í, ìë°ìì ëłêž°, ìŽì ìì ë „ íčì íì ë°©ìŹì ë „ì ìĄ°ìŹíìë€. ìë° ë¶ì ì ì í êČ°ìë¶ì íŹêž°, ì±ì·ší íŒíì íŹêž°, íêŽêČœì êžžìŽ, íêŽêČœêłŒ 돞í©í ìíë¶ì ëì 맄, êł”ìŹë¶ì ëŽí©ë°©ëČì ìĄ°ìŹíìë€. ìì íìë íŒí ìŽìì ì±êł”ë„ , ìíë¶ì êł”ìŹë¶ì í©ëłìŠì íê°íìë€.
ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ìì êž°ëČ
ëȘšë ìì ì ì ì ë§ì·š íì í ëȘ
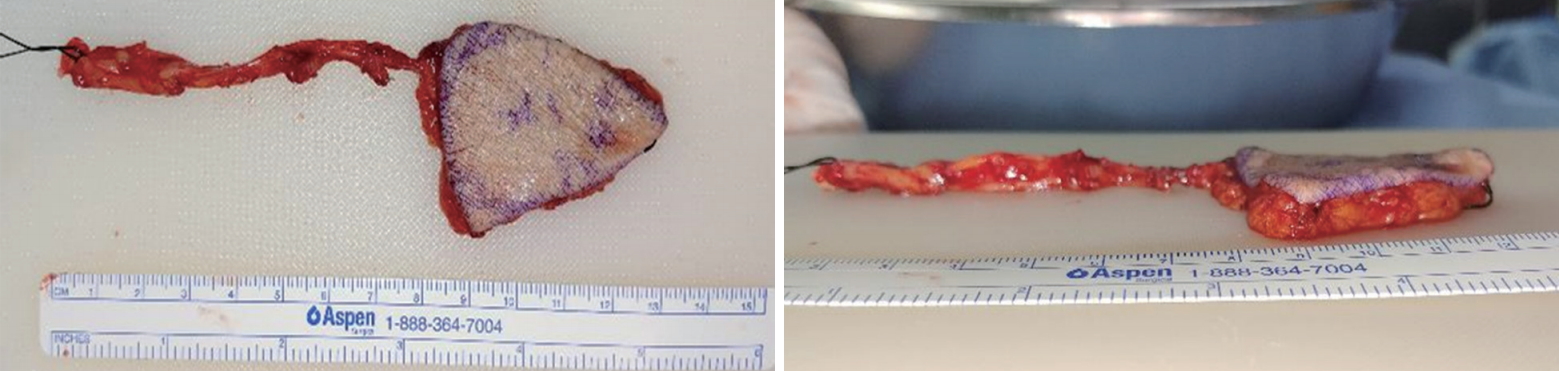
ì ëêČœë¶ ìžêłŒìì ìíŽ ìíëììŒë©° íŒíì íŹêž°ë ìë°ë¶ êČ°ìë¶ì íŹêž°ìì ìœ 1 cmì ì ì ì°(safety margin)ì ëêł ëìëììŒë©° íŒí ê±°ì ë° íêŽêČœì íìžì ìŽì ìŹëŹ 돞íìì êž°ì ë ëëĄ ìííìë€(Fig. 1) [1,12,14,17]. êł êŽì ì ìžì , ìŹêŽì ì ìœê° ê”ŽêłĄë ììžë„Œ ì·šíëëĄ í ìŽí ìČêł”ì§ì ììčë„Œ íìžíìë€. ëȘšë ììì íŒí ê±°ìì íêž° ì ì ëíëŹ ìŽìí íëĄëžë„Œ ìŽì©íìŹ ìČêł”ì§ì ììčë„Œ ì°Ÿìë€. 충ë¶í íŹêž°ì ìŁŒìí ìČêł”ì§ë ìŹììŁŒëŠ(popliteal crease)ì ì€ìŹììë¶í° ëŽìžĄ ëł”ìŹ(medial malleolus)êčì§ ê·žì ì ìì ìŹì ìŁŒëŠì ì€ìŹìŒëĄë¶í° 8~12 cm ìŹìŽì ììčíŽ ììë€. íŒíì ëŽìžĄ êČœêłë¶í° ìĄ°ìŹì€ëœêČ ê±°ìíìŹ ìą
ì늏 íë©Žì ì€ìŹì ììë¶í° ê·ŒìĄëŽ ë°ëŠŹë„Œ ììíììŒë©° íŒí ìŽìì ìŹì©í ê°ì„ í° ìČêł”ì§ë„Œ íìžíìë€. ìŽí íêŽêČœì ìą
ì늏 íë¶ ê·ŒìĄë€êłŒ ë¶ëŠŹíë©Žì ìŹìë맄(popliteal artery) ë°©í„ìŒëĄ ë°ëŠŹíìŹ ëčëł”ê·Œ(gastrocnemius muscle)ì ëŽìžĄê±Ž ë¶ê·Œìì ì±ì·šíìë€. ìŒë°ì ìŒëĄ íêŽêČœì ìŁŒíêČœëĄë ëčëł”ê·Œ ê·ŒìŹì ì íííëŻëĄ ëčëł”ê·Œì ë°ëŠŹíšìŒëĄìš íêŽêČœì ìœêČ ë
žì¶í ì ììë€. ì 맄 ì ì¶ëĄ venous output flowë„Œ ëëŠŹêž° ìíŽ ê°ë„í 2ê°ì ëë°ì 맄ì ê°ìŽ ì±ì·šíììŒë©° êł”ìŹë¶ë ëȘšë ììì ìŒì°š ëŽí©ëìë€.
êČ° êłŒ
2018ë
10ìë¶í° 2019ë
7ìêčì§ ëêČœë¶ êČ°ì ìŽí 8ìì ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ìŽì©í ìŹê±Žì ìŽ ìíëìë€. ëì íìì íê· ëìŽë 61.6ìž(43~87ìž)ëĄ ì ìČŽ 8ëȘ
ì€ ëšìê° 6ëȘ
(75.0%), ìŹìê° 2ëȘ
(25.0%)ìŽìë€. 1ììì(Table 1, case 8)ìì 11ë
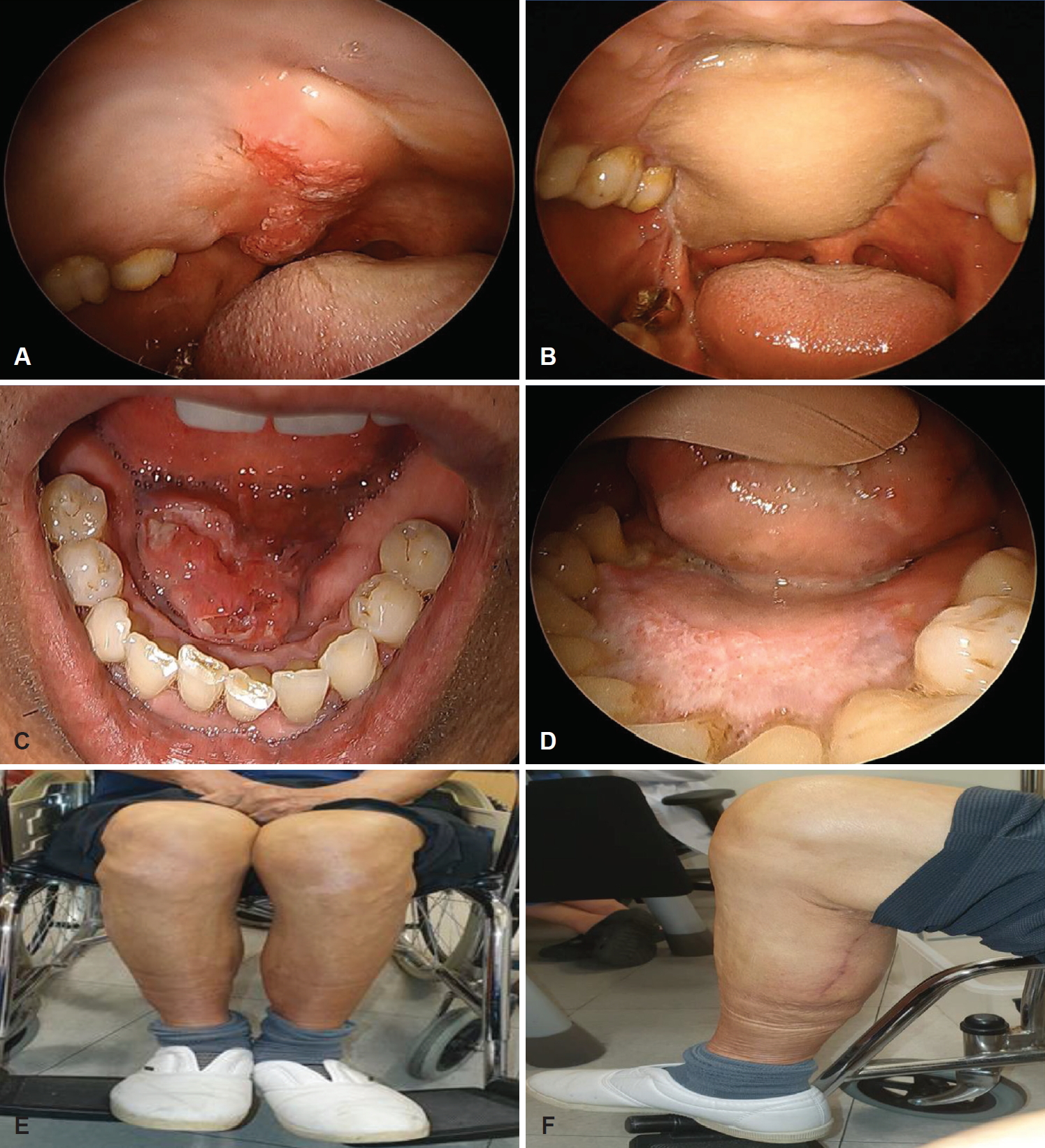
ì ìë° ë¶ì ì ì ì ë° ëčìíŒíì ìŽì©í ìŹê±Žì ì ë°ì ìì ë „ ë° ìë°ë¶ ìŹë°ëĄ ë°©ìŹì ìčëŁë „ìŽ ìììŒë©° ìŽìž íìë€ì êČœì° ìŽì ìì ë „ ë° ì í íì ë°©ìŹì ííìčëŁë„Œ ë°ì êČœì°ë ììë€. ëì íìì ìë° ë¶ìë ì€ë¶(tongue) 3ì, ê”Źê°ì (floor of mouth) 1ì, ì€êž°ì ë¶(base of tongue) 1ì, êČœê”Źê°(hard palate) 1ì, ì°ê”Źê°(soft palate) 1ì, ëčììŁŒëŠ(nasolabial fold) 1ì ìë€. ìì ëłêž°ë T4aN1M0 1ì, T3N3bM0 1ì, T3NXM0 1ì, T3N0M0 2ì, T2N0M0 3ììë€. ìì í 1ììì íìë°©ìŹì ìčëŁ, 2ììì ë°©ìŹì ìčëŁë„Œ ë°ììŒë©° 5ìë ìì ìŽí ëłŽìĄ°ìëČì ë°ì§ ììë€(Table 1).
ìë°ì ì ì í êČ°ìë¶ì íê· íŹêž°ë 26.1 cm2 (16~45 cm2), íê· êžžìŽë 6.3 cm(4.0~9.0 cm), íê· ëëčë 4.1 cm (3.5~5.0 cm)ìêł , íŒíì íê· íŹêž° 34.1 cm2 (17.5~50 cm2), íê· êžžìŽë 7.1 cm(5.0~10.0 cm), íê· ëëčë 4.7 cm(3.5~5.0 cm)ìŽìë€. íêŽêČœì íê· êžžìŽë 9.2 cm(8~10 cm)ìŽìë€(Fig. 2). ë맄 돞í©ì 7ì(87.5%)ìì ìë©Žë맄ì, 1ì(12.5%)ìì ì€ë맄ì ìíëìë€. ì 맄 돞í©ì 6ììì ëê°ì ì 맄ì ìíëììŒë©° ê°ê° 4ììì ìë©Žì 맄ë(facial vein plexus), 1ììì ìë©Žì ë§„êłŒ ì€ì 맄, 1ììì ìë©Žì ë§„êłŒ ìê°ìì ì 맄ì 돞í©ëìë€. 2ìììë ê°ê° 1ê°ì ìë©Žì 맄ì 돞í©ëìë€. ëȘšë ììì êł”ìŹë¶ë ìŒì°š ëŽí©ëììŒë©° í©ëłìŠììŽ íëł”ëìë€(Table 2). ì ìČŽ 8ëȘ
ì íì ì€ 1ëȘ
ì íì(case 1)ìì ìì í ìŽìë¶ì ëČìŽì§(dehiscence)ìŽ ìììŒë©°, íêŽêČœ ì±ì·šì ëë§„ë¶ ë¶ì (pedicle arterial insufficiency) ë° ìì ìŽí íìë°©ìŹì ìëČì ë°ì ììë€. 1ì(case 4)ìì ìì í 5ìŒì§ž íŒíì ííŒ(flap desquamation)ê° ë°ìíììŒë©° ìŽì ì€íšëĄ íëšíìŹ íŒíì ì ê±°íìë€. ì ìČŽ 8ëȘ
íìì ìì í êČœêłŒêŽì°° êž°ê°ì íê· 6.6ê°ì(1~8ê°ì)ìŽë©° ìì í êł”ìŹë¶ì êž°ë„ì ë° ëŻžì©ì í©ëłìŠì ëȘšë ììì ìììŒë©° íŒí ìŹê±Ž ìŽí ì¶ê°ì ìž ì€ìŹê° íìí ì ëì ìíë¶ì êž°ë„ì ìž êČ°íšì ížìíë êČœì°ë ììë€(Fig. 3).
êł ì°°
ëêČœë¶ìì ìŹê±Žì ìí íŒíì êČ°ìë¶ì íŹêž°, ììč, ìíë¶ ë° êł”ìŹë¶ì êž°ë„ì ëłŽìĄŽ, êł”ìŹë¶ì í©ëłìŠ ë±ì êł ë €íìŹ ì íëìŽìŒ íë€. ì€ë«ëì ìŹì©ëìŽì€ë ëêČœë¶ ìŹê±Žì ëíì íŒíì ì ìžìžĄëíŽ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíìŽë€[1,2]. ìêłšì ì ì 늏íŒíì ìêł ì ì°íë©° ꞎ íêŽêČœì ê°ì§êł ììŽ ê”Źê°ìì ìŹê±Žì ì í©í íŒíìŽë€. íì§ë§ ëë¶ë¶ì êČœì°ìì íŒí ì±ì·š ìŽí êł”ìŹë¶ì íŒë¶ ìŽììŽ íìíë©° ìŽì ìŽíìë ìŽìë¶ê° ëë ·íêČ ëì ëë 믞ì©ì ìž ëšì ë° ìë¶ì ìŁŒìí ëë§„ìž ìêłšë맄(radial artery)ì íŹìíêž° ë돞ì ì ìŹì ìž ìë¶ ííì ìíìŽ ìë€[18,19]. ì ìžìžĄëíŽ ì 늏íŒíì êžžêł ì¶©ë¶í íŹêž°ì ì§êČœì ê°ì§ íêŽêČœì ì»ì ì ììŒë©° í° ë¶ìì êČ°ìë ìŹê±ŽìŽ ê°ë„íë©Žìë êł”ìŹë¶ì êČ°íšìŽ ì ìŽì ì€ë«ëì ëêČœë¶ ìŹê±Žì ìŹì©ë íŒí ì€ íëìŽë€[1,6]. íì§ë§ ê”Źê°ìì ìŹê±Žíêž°ìë ë¶íŒê° íŹêł ì ì°íì§ ëȘ»íë©° íŒíì ìêČ ìŹëìíë êłŒì ìì íë„(vascularity)ì ììì ì€ ì ìë€[7,8,20]. ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ìêł ì ì°í íŒíì ì»ì ì ìë ì ì ìêłšì ì ì 늏íŒíêłŒ ì ìŹíì§ë§ ëë¶ë¶ì êČœì°ìì êł”ìŹë¶ì ìŒì°šëŽí©ìŽ ê°ë„íìŹ ìêłšì ì ì 늏íŒíì ëčíŽ ëŻžì©ì êČ°êłŒê° ì°ìíë€[21]. Kao ë±[10]ì ëêČœë¶ìì ìŹê±Žìì ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíì ëčê” ì, ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíìŽ ìêłšì ì ì 늏íŒíì ëčíŽ ë ì°ìí êł”ìŹë¶ì êž°ë„ ëłŽìĄŽ ë° ëŻžì©ì êČ°êłŒë„Œ 볎ìë€êł ëłŽêł íìë€. Daar ë±[21]ìŽ ë°íí ë©íë¶ì ë
ŒëŹžìì ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì êł”ìŹë¶ì ìꞎ í©ëłìŠì 1.9%ëĄ ìŽë íìŹêčì§ ëłŽêł ë ëêČœë¶ ìŹê±Ž ìŽí êł”ìŹë¶ì í©ëłìŠ ì€ ê°ì„ ëźì ììč ì€ íëìŽë€.
Taufique ë±ì ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ íŒíì íêŽêČœì íê· êžžìŽë 10.1 cmëĄ ìŽë ìŹê±Žì ê°ì„ ë§ìŽ ìŹì©ëë ìë©Ž ëì 맄ì 돞í©íêž°ì 충ë¶í íêŽêČœì êžžìŽëŒêł ëłŽêł íìë€[1,2,22]. ëłž ì°ê”Źììë ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ íŒíì íêŽêČœì íê· êžžìŽë 9.2 cmëĄ ìžĄì ëììŒë©° ì ìžìžĄëíŽ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíì ëčíŽ ë€ì 짧ì êČœí„ìŽ ììë€. ìì ì íì§ íêŽìĄ°ì ì ì°íëšìž”ìŽŹì(lower extremity CT angiography)êłŒ ìì ì€ ëíëŹ ìŽìí íëĄëžë ìČêł”ì§ì ììčë„Œ íê°íëë° ëììŽ ëë©°, ëíëŹ ìŽìí íëĄëžë„Œ ìŽì©í ìČêł”ì§ì íìžì 92.8%ì ì íëë„Œ 볎ìë€[22,23]. ìŁŒì ìČêł”ì§ë ìŹììŁŒëŠ(popliteal crease)ì ì€ìŹì ììë¶í° ëŽìžĄëł”ìŹ(medial malleolus)êčì§ ìŽì ì ìì ìŹììŁŒëŠ(popliteal crease)ìŒëĄë¶í° 8~12 cm ê±°ëŠŹì ììŒë©°, íê· 2~8ê°ì ìČêł”ì§ê° ë°êČŹëë©° ëê°ì êČœì° ì°ìž ìČêł”ì§(dominant perforator)ê° ìë€êł ëłŽêł ëìë€[24,25]. ëłž ì°ê”Źììë ìČêł”ì§ê° ëë¶ë¶ 2ê° ìŽíëĄ ë°êČŹëììŒë©° ë€ì ê°ëìë€. íŒíì ëìì ê°ë„í ìČêł”ì§ê° íŒíì ì€ìì ìëëĄ ëììžíë êČìŽ ìŽìì ìŽë©°, ëê°ì êČœì° 1ê°ì ìČêł”ì§ëĄë íŒíì íìĄ êł”êžìŽ ê°ë„íë€[21]. Taufique ë±ì ëŽìžĄ ëčëł”ë맄 ìČêł”ì§ íŒíì íê· ëê»ë„Œ 8 mm, Toyserkani ë±ì íê· 5 mmëĄ ëłŽêł í ë° ìë€[1,2]. ì ìžìžĄëíŽ ì 늏íŒíì íê· ëê»ë 11.55±4.38 mm, ëŽìžĄ ëčëł”ë맄 ìČêł”ì§ ì 늏íŒíì 8.31±3.6 mmëĄ ëŽìžĄ ëčëł”ë맄 ìČêł”ì§ ì 늏íŒíìŽ ì ìžìžĄëíŽ ì 늏íŒíëłŽë€ ì ìíêČ ìë€êł ëłŽêł ë ë° ììŒë©°[26], ì ìì êČœíìŒëĄë ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ íŒíì ëê»ë 5 mm ê°ëìŒëĄ 볎ìŽë©° ì ìžìžĄëíŽ ì 늏íŒíì ëčíŽ ììë€. ìŽë ì ì°íìŹ ìì íêČ ì íìŽ ê°ë„íìŹ ì€ë±ëì ê”Źê° êČ°ì ìŹê±Ž ìŽí ê”Źê° êž°ë„ì íëł”íëë° ìŽìì ìŽë€[21,27]. ëŽìžĄ ëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ìêłšì ì ì 늏íŒíì ëčíŽì ë¶íŒê°ìŽ ììŒë©Žì ì ìžìžĄëíŽ ì 늏íŒí ëłŽë€ ì ì°í íŒíìŒëĄ ì€ë±ë êČ°ìì ê”Źê°ì, íčí ê”Źê°(palate)ì ê”Źê°ì (floor of mouth) ê°ì ìì íŒíì ìíë ë¶ìì ì ì©íë©° ë¶íŒê°ì ìíë ìì
ë¶, ìë©Žë¶ì ìŹê±Žìë ì í©íì§ ìì êČìŒëĄ ìê°ëë€. ëí ìêłšì ì ì 늏íŒíì ëčíŽ ëŻžì©ì ìŒëĄ ì°ìí ì„ì ìŽ ììŒë ìČêł”ì§ê° ëë ·íì§ ìì êČœì°ê° ììŒë©° íêŽêČœì ì±ì·šíêž°êčì§ ê·ŒìĄ ëŽ ë°ëŠŹêłŒì ìŽ ì§ëŁšíêł ìê°ìŽ ë§ìŽ ê±žëŠŹë ëšì ìŽ ììŒëŻëĄ[21] ì 늏íŒí ìŹê±Žì ì ì”ìí êČœíìë ì ìê° ìŹì©íë êČì ê¶íë€.
Taufique ë±ìŽ íí ë©íë¶ììì ì 늏íŒíì ìŽì©í ê”Źê°ì ìŹê±Žìì ìíë¶ì í©ëłìŠ ëčê”ì, ëŽìžĄ ëčëł”ë맄 ìČêł”ì§ ì 늏íŒí ìíë¶ì í©ëłìŠìšì 14.3%ëĄ ë€ë„ž ì 늏íŒíì êČœì°(10.4~16.7%)ì ëčì·íë€[2,19,28]. ëčëł”ë맄 ìČêł”ì§ ì 늏íŒíì ìŽì ì€íšìšì 9.9%ëĄ ì ìžìžĄëíŽ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíì ì€íšìšìŽ 2~4%ìž êČì ëčíŽ ëìë€[1]. ìŽë ìëĄìŽ íŒíìŽêž° ë돞ì ìŽì êČ°êłŒì ëí ì ì ìí ìì íì”êłĄì (learning curve)ìŒëĄ ìží ìí ížêČŹ(sampling bias)ì ìíìŽ ìì§ë§, íìŹêčì§ ëłŽêł ë íŒí ìŽì ì€íšì ê°ì„ íí ììžì ì 맄 ì ì¶ëĄì ë¶ì ìŒëĄ ëłŽêł ëìë€[1,21]. ê·žëŹëŻëĄ íêŽ ëŹží© êłŒì ìì ìì í ì 맄 ì ì¶ëĄë„Œ í볎íë êČìŽ ê¶ì ëêł ììŒë©°, ëšìŒ ì 맄 돞í©ëłŽë€ íìŹì± ì 맄(superficial vein) íčì ììžĄ ëë°ì 맄ì ìŽì©íìŹ 2ê°ì ì 맄 돞í©ì íìì ì ì 맄 ë¶ì (venous insufficiency)ìŽ ë íìë€êł ëłŽêł ë ë° ìë€[1,29]. ëë¶ë¶ì 돞íìì ëčëł”ë맄 ìČêł”ì§ì ëë° ì ë§„ìŽ ëŹží©ì ìŽì©ëë íêŽêČœì ì§êČœìŽ ì 맄 ì ì¶ì ì ì ìč ìë€êł íëšëë©Ž íìŹì± ì 맄(superficial vein)ìŽ ëììŒëĄ ìŹì© ê°ë„íë€[14]. ëłž ì°ê”Źììë ê°ë„í ëê°ì ì 맄 돞í©ì íë €êł íììŒë©° 8ì ì€ 6ì(75%)ìì ëê°ì ì 맄 돞í©ì íìë€. 8ì ì€ ì 맄 ì ì¶ëĄì 돞ì ëĄ ìží íŒíì ì€íšë ìììŒë íŒí ìŽìì ì€íší 1ì(Table 2, case 4)ììë íêŽêČœìŽ ë§€ì° ìììŒë©° ë맄 ë¶ì ìŒëĄ ìží ì€íšëĄ íëšëìë€. ìí ìê° ì êž°ë íë ëłž ì°ê”Źì êČœíì ëŽìžĄ ëčëł”ë맄 ìČêł”ì§ë ë€ì íìĄëìŽ ìąì§ ëȘ»í êČœì°ê° ìììŒë©° íêŽêČœì ì§êČœ ë° ëê»ê° ìŒì ìč ëȘ»íêł íêŽêČœì êžžìŽê° ì ìžìžĄëíŽ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíì íêŽêČœì ëčíŽ ë€ì 짧ìë€[21].
êłŒê±° 돞íë€ìì íŒíì ëëčê° 5 cm ìŽììŒ êČœì° ë¶ë¶ìž” íŒë¶ ìŽì(split-thickness skin graft)ì ê¶íë€êł ëłŽêł ëììŒë[14,30], 2019ë
ë°íë ëčëł”ë맄 ìČêł”ì§ ì 늏íŒíì ëí ë©íë¶ììì ë¶ë¶ìž” íŒë¶ ìŽìì ìíí êł”ìŹë¶ì íê· êČ°ì íŹêž°ë 97.6 cm2(12.2Ă8.0 cm)ìŽììŒë©°, ìŒì°š ëŽí©í êČœì°ë 44.5 cm2(5.0Ă8.9 cm)ìŽìë€[21]. ëłž ì°ê”Źììë íŒíì ëëčê° 10 cmìž êČœì°ë 돞ì ììŽ êł”ìŹë¶ì ìŒì°š ëŽí©ìŽ ê°ë„íìë€.
ìŽ ì°ê”Źë ëì íìê° ì ìŒë©° ëêČœë¶ ìŹê±Žì ì ëíì ìŒëĄ ì°ìŽë ì ìžìžĄëíŽ ì 늏íŒíêłŒ ìêłšì ì ì 늏íŒíêłŒ ì§ì ëčê” ë¶ìì íì§ ëȘ»í ì íì ì ê°ì§êł ìë€. ëí ëšìŒ êž°êŽì ëšìŒ ìžêłŒìì ìíŽ ìíë ìì ì ë¶ìíìŹ ìŽì ë°ë„ž ì í ížêČŹ(selection bias)ìŽ ê°ì
ë ìŹì§ê° ìë€. í„í ë€ë„ž íŒíêłŒì ì§ì ë¶ìì ë€ëŁŹ ì í„ì ìž ì°ê”Źê° íìíë€. íì§ë§ ìŽ ì°ê”Źë ì”ìŽëĄ íê”ìžì ëêČœë¶ êČ°ìë¶ì ìŹê±Žì ëŽìžĄëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ì ì©íêł ê·ž íčì§ì ë¶ìí ì ìì ììê° ìë€. ëłž ì°ê”Źë„Œ í”íŽ ëŽìžĄëčëł” ë맄 ìČêł”ì§ ì 늏íŒíì ì€ë±ëì ëêČœë¶ êČ°ìì ìŹê±Žì ì ì í ìêł ì ì°í íŒíì ì»ì ì ììŒë©Žì ëìì êł”ìŹë¶ì 믞ì©ì ì±ì ìŽ ì°ìí ë°©ëČìì íìží ì ììë€.