ņä£ļĪĀ
ļé£ņ▓ŁņØĆ Ļ░Ćņן ĒØöĒĢ£ ņØĖĻ░äņØś Ļ░ÉĻ░üņןņĢĀ ņżæ ĒĢśļéśņØ┤ļ®░, ļģĖņØĖņŚÉĻ▓ī 3ļ▓łņ¦ĖļĪ£ ĒØöĒĢ£ ļ¦īņä▒ņ¦łĒÖśņØ┤ļŗż[1]. ļģĖĒÖöņŚÉ ņØśĒĢ£ Ēć┤Ē¢ēņä▒ ļ│ĆĒÖöļĪ£, 65ņäĖ ņØ┤ņāüņØś Ļ│ĀļĀ╣ņØś ĒÖśņ×ÉļōżņØĆ ļé£ņ▓Ł ļ░£ņāØņØ┤ ĻĖēĻ▓®Ē׳ ņ”ØĻ░ĆĒĢ£ļŗż. ņĀ£8ĻĖ░ ĻĄŁļ»╝Ļ▒┤Ļ░Ģņśüņ¢æņĪ░ņé¼ Ļ▓░Ļ│╝ņŚÉ ļö░ļź┤ļ®┤, 65ņäĖ ņØ┤ņāüņØś ņä▒ņØĖņŚÉņä£ ņżæņ”ØļÅä ņØ┤ņāü ļé£ņ▓Ł ņ£Āļ│æļźĀņØĆ ļé©ņä▒ 44.7%, ņŚ¼ņä▒ 36.2%ņØ┤ļ®░, 70ņäĖ ņØ┤ņāüņŚÉņä£ļŖö ļé©ņä▒ 54.0%, ņŚ¼ņä▒ 44.5%ņŚÉ ļŗ¼ĒĢ£ļŗż[2].
ļģĖņØĖņŚÉņä£ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņÖĆņØś ņŚ░Ļ┤Ćņä▒ņØĆ, ņ▓ŁĻ░üņןņĢĀļź╝ Ļ░Ćņ¦ä ļģĖņØĖņØ┤ ņĀĢņāü ņ▓ŁļĀźņØä Ļ░Ćņ¦ä ļģĖņØĖļ│┤ļŗż ļ╣ĀļźĖ ņØĖņ¦ĆļĀź ņĀĆĒĢśļź╝ ļ│┤ņØĖļŗżļŖö Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ļŖö ņĀäĒ¢źņĀüņØ┤Ļ│Ā ņóģņĀüņØĖ(prospective, longitudinal) ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØä ĒåĄĒĢ┤ ĒÖĢļ”ĮļÉśņŚłļŗż[3-8]. ņØ┤ļĀćĻ▓ī ņ▓ŁĻ░üņןņĢĀņÖĆ ņØĖņ¦ĆļĀź ņĀĆĒĢśņØś ņŚ░Ļ┤Ćņä▒ņØä ļ│┤ņŚ¼ņŻ╝ļŖö ļŗżļģäĻ░äņØś ņŚ░ĻĄ¼ļōżņØä ņŚ░ĻĄ¼ ĻĖ░Ļ░ä, ļīĆņāü ĒÖśņ×É ņłś, ņ▓ŁĻ░üņןņĢĀ ĒÅēĻ░Ćņ¦ĆĒæ£, ņØĖņ¦ĆĻĖ░ļŖź ĒÅēĻ░Ć ņ¦ĆĒæ£ ļ░Å ņŚ░ĻĄ¼Ļ▓░Ļ│╝ņŚÉ ļīĆĒĢ┤ ņĀĢļ”¼ĒĢ┤ņä£ Table 1ņŚÉņä£ ļ│┤ņŚ¼ņŻ╝ņŚłļŗż. ĻĘĖļ¤¼ļéś ņĢäņ¦ü ļģĖĒÖöņä▒ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņØś Ļ┤ĆļĀ©ņä▒ņŚÉ ļīĆĒĢ£ ņøÉņØĖ ĻĖ░ņĀäņØĆ ļ¬ģĒÖĢĒ׳ ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśĻ│Ā, ļ│ĄĒĢ®ņĀüņØĖ ņÜöņØĖļōżņØ┤ Ļ┤ĆņŚ¼ĒĢśļŖö Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż[9]. ļśÉĒĢ£, ļé£ņ▓ŁņØĆ ņ╣śļ¦żņŚÉ ļīĆĒĢ£ 12Ļ░Ćņ¦Ć ņ£äĒŚśņÜöņØĖ ņżæ, Ļ░Ćņן Ēü░ ņ×Āņ×¼ļĀźņØä ņ¦Ćļŗī ņłśņĀĢ Ļ░ĆļŖźĒĢ£ ņ£äĒŚś ņÜöņåīņØ┤ļ®░[10,11], ļé£ņ▓ŁņŚÉ ļīĆĒĢ£ ņ▓ŁĻ░üņĀü ņżæņ×¼ļź╝ ĒåĄĒĢ┤ ņ╣śļ¦żĻ░Ć ņśłļ░®ļÉĀ ņłś ņ׳ļŗżļŖö Ļ▓āņØä ņĀ£ņĢłĒĢ£ļŗż. ĻĘĖļ¤¼ļéś, ņØĖņ¦ĆĻĖ░ļŖźņŚÉ ļīĆĒĢ£ ļ│┤ņ▓ŁĻĖ░ņØś ĒÜ©Ļ│╝ļŖö ņĢäņ¦ü ļ¬ģĒÖĢĒĢśņ¦Ć ņĢŖņØĆļŹ░[12,13], ņØ┤ļŖö ļ│┤ņ▓ŁĻĖ░ļĪ£ ņØĖĒĢ£ ņ▓ŁļĀźņØś Ē¢źņāüņØ┤ ļģĖņØĖ ĒÖśņ×ÉņŚÉĻ▓ī ņĀ£ĒĢ£ņĀüņØ┤ĻĖ░ ļĢīļ¼ĖņØ┤ļŗż. Ļ│Āņŗ¼ļÅä Ļ░ÉĻ░üņŗĀĻ▓Įņä▒ ļé£ņ▓Ł(profound sensorineural hearing loss) ĒÖśņ×ÉļōżņŚÉĻ▓ī ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ(cochlear implantation)ņØĆ ņ£ĀņØ╝ĒĢśĻ▓ī Ļ░ĆļŖźĒĢ£ ņ╣śļŻīļ▓ĢņØ┤ļ®░, ņłśņłĀ ņØ┤Ēøä ņ▓ŁļĀź ņłśņżĆņØĆ Ēü¼Ļ▓ī Ē¢źņāüļÉ£ļŗż. ņØ┤ļŖö ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä, ļģĖņØĖņØś ņ▓ŁĻ░ü ņłśņżĆņØ┤ ņØĖņ¦ĆļŖźļĀźņŚÉ ĻĖŹņĀĢņĀüņØĖ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ņØīņØä ņŗ£ņé¼ĒĢĀ ņłś ņ׳ļŗż. ļ│Ė ņŚ░ĻĄ¼ņŚÉņä£ļŖö ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņ▓ŁĻ░üņןņĢĀņÖĆ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņØś ņŚ░Ļ┤Ćņä▒ ļ░Å ņØĖĻ│Ą ņÖĆņÜ░ ņłśņłĀ Ēøä ņØĖņ¦ĆĻĖ░ļŖź Ē¢źņāüņŚÉ ļīĆĒĢ£ Ļ▓░Ļ│╝ļź╝ ņĄ£ĻĘ╝ ļģ╝ļ¼Ė ļ”¼ļĘ░ļź╝ ĒåĄĒĢ┤ ņĀĢļ”¼ĒĢśĻ│Ā, ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀĻ│╝ Ļ░ÖņØĆ ņ▓ŁĻ░üņĀü ņżæņ×¼Ļ░Ć ņØĖņ¦Ć ĻĖ░ļŖźņŚÉ ņ׳ņ¢┤ ņ¢┤ļ¢ż ņśüĒ¢źņØä ļ»Ėņ╣Āņ¦ĆņŚÉ ļīĆĒĢ┤ ņĢīņĢäļ│┤Ļ│Āņ×É ĒĢ£ļŗż.
ļ│ĖļĪĀ
ļģĖņØĖņŚÉĻ▓ī ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņØś ņŚ░Ļ┤Ćņä▒
ņĄ£ĻĘ╝ņŚÉ ņ▓┤Ļ│äņĀü ļ”¼ļĘ░ ļ░Å ļ®öĒāĆ ļČäņäØņŚÉ ļīĆĒĢ£ ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØĆ ļģĖņØĖņŚÉņä£ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś ļ░Å ņ╣śļ¦ż ņ£äĒŚśņØś ņ”ØĻ░Ć ļō▒ņŚÉ Ļ┤ĆĒĢ£ ņŚ░Ļ┤Ćņä▒ņØä ļ│┤ņŚ¼ņŻ╝Ļ│Ā ņ׳ļŗż[14-16]. 20264ļ¬ģņØä ļīĆņāüņ£╝ļĪ£ ĒĢ£ 36Ļ░£ņØś ņŚ░ĻĄ¼ļōżņØä ļ®öĒāĆ ļČäņäØĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£, ļģĖĒÖöņä▒ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś(odds ratio [OR], 1.22; 95% confidence interval [CI], 1.09-1.36)ņÖĆ ņ╣śļ¦ż(OR, 1.28; 95% CI, 1.02-1.59)ņÖĆņØś ņ£ĀĒÜ©ĒĢ£ ņŚ░Ļ┤Ćņä▒ņØä ĒÖĢņØĖĒĢśņśĆļŗż[14].
Lin ļō▒[3,4]ņØĆ ļģĖņØĖņŚÉņä£ ļé£ņ▓ŁņØś ņŗ¼Ļ░üļÅäĻ░Ć Ļ░ĆņåŹĒÖöļÉ£ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņÖĆ ļÅģļ”ĮņĀüņ£╝ļĪ£ ņŚ░Ļ┤ĆļÉ©ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż. Ļ▓░Ļ│╝ņĀüņ£╝ļĪ£, ņØĖņ¦ĆĻĖ░ļŖź ĒÅēĻ░ĆņŚÉņä£ ļé£ņ▓ŁņØś ņĀĢļÅäĻ░Ć ņŗ¼ĒĢĀņłśļĪØ ļŹö ļéśņü£ ņØĖņ¦ĆĻĖ░ļŖźĻ│╝ ņ£ĀņØśļ»ĖĒĢ£ ņāüĻ┤ĆĻ┤ĆĻ│äļź╝ Ļ░Ćņ¦ÉņØä ĒÖĢņØĖĒĢĀ ņłś ņ׳ņŚłļŗż. ļśÉĒĢ£, 25 dB HL ņØ┤ņāüņØś ļé£ņ▓ŁņØ┤ ņ׳ļŖö Ļ▓ĮņÜ░ ņ▓ŁļĀźņŚŁņ╣śĻ░Ć 10 dBņö® ņ”ØĻ░ĆĒĢ©ņŚÉ ļö░ļØ╝ ņ╣śļ¦ż ļ░£ņāØ ņ£äĒŚśņØ┤ 20% ņ”ØĻ░ĆĒĢ£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[3]. 6ļģäĻ░äņØś ņČöņĀü Ļ┤Ćņ░░ ļÅÖņĢł, ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖņØĆ ņĀĢņāü ņ▓ŁļĀźņØä Ļ░Ćņ¦ä ļģĖņØĖņŚÉ ļ╣äĒĢ┤, 30%-40%ņØś ļé«ņØĆ ņØĖņ¦ĆĻĖ░ļŖźņØä ļ│┤ņśĆĻ│Ā, ņØĖņ¦ĆņןņĢĀ ņ£äĒŚśņØ┤ 24% ņ”ØĻ░ĆĒ¢łļŗż[4].
ļö░ļØ╝ņä£, ļé£ņ▓ŁņØĆ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś ļ░Å ņ╣śļ¦ż ļ░£ņāØĻ│╝ ļÅģļ”ĮņĀüņØĖ ņŚ░Ļ┤Ćņä▒ņØä Ļ░¢ļŖöļŗżĻ│Ā ĒĢĀ ņłś ņ׳ļŗż. ņĄ£ĻĘ╝ņØś ņŚ░ĻĄ¼ļōżņŚÉņä£ ņ▓ŁļĀźņØ┤ ņĀĢņāüņØĖ ņä▒ņØĖņŚÉ ļ╣äĒĢ┤, Ļ▓ĮļÅä, ņżæļō▒ļÅä, ņŗ¼ļÅä ļé£ņ▓ŁņØ┤ ņ׳ļŖö ņä▒ņØĖņŚÉņä£ ņ╣śļ¦ż ļ░£ņāØ ņ£äĒŚśņØ┤ Ļ░üĻ░ü 2ļ░░, 3ļ░░, 5ļ░░ ņØ┤ņāü ņ”ØĻ░ĆĒĢ©ņØä ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ļŗż[4,17]. ļśÉĒĢ£, ņĄ£ĻĘ╝ņØś ņĀäĒ¢źņĀü ņĮöĒśĖĒŖĖ ņŚ░ĻĄ¼ļōżņŚÉņä£ļŖö ļé£ņ▓ŁņØ┤ ņ╣śļ¦ż ļ░£ņāØņŚÉ ņ׳ņ¢┤ ļÅģļ”ĮņĀüņØĖ ņ£äĒŚśņÜöņØĖņ×äņØä ļ│┤ņŚ¼ņŻ╝Ļ│Ā ņ׳ļŗż[3,18-20]. ļé£ņ▓ŁņØ┤ ņ╣śļ¦ż ļ░£ņāØņØś ņ£äĒŚśņÜöņØĖņ×äņØä ņäżļ¬ģĒĢśĻĖ░ ņ£äĒĢ┤, Ļ░£ņ▓┤ĻĄ░ ĻĘĆņåīļČäĒÜŹ(population attributable fraction)ņØ┤ļØ╝ļŖö Ļ░£ļģÉņØä ņé¼ņÜ®ĒĢĀ ņłś ņ׳ļŖöļŹ░, ņØ┤ļŖö ņŻ╝ņ¢┤ņ¦ä ĻĖ░Ļ░ä ļÅÖņĢł ļé£ņ▓ŁĻ│╝ Ļ░ÖņØĆ ņ£äĒŚśņÜöņØĖņØ┤ ņĀ£Ļ▒░ļÉśņŚłņØä ļĢī, ņ╣śļ¦ż ļ░£ņāØņØ┤ Ļ░ÉņåīĒĢśļŖö ļ╣äņ£©ņØä ļéśĒāĆļéĖļŗż[11]. ņ╣śļ¦ż ļ░£ņāØņŚÉņä£ ļé£ņ▓ŁņØś ĻĘĆņåīļČäĒÜŹņØĆ 23.0%ļĪ£, ņØ┤ļŖö ņÜ░ņÜĖ (10.1%), ņé¼ĒÜīņĀü Ļ│Āļ”Į(5.9%), ĒØĪņŚ░(13.9%), Ļ│ĀĒśłņĢĢ(5.1%), ļŗ╣ļć© (3.2%) ļō▒ņØś ļŗżļźĖ ņ£äĒŚśņÜöņØĖļōżļ│┤ļŗż Ļ░Ćņן ļåÆņØĆ ņłśņ╣śņØ┤ļŗż[11]. ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś ļ░Å ņ╣śļ¦ż ļ░£ņāØ ņé¼ņØ┤ņŚÉ ņØĖĻ│╝Ļ┤ĆĻ│äĻ░Ć ņĀĢļ”ĮļÉ£ļŗżļ®┤, ļ│┤ņ▓ŁĻĖ░ļéś ņØĖĻ│ĄņÖĆņÜ░ņÖĆ Ļ░ÖņØĆ ņ▓ŁĻ░üņ×¼ĒÖ£ņØä ĒåĄĒĢ£ ņ▓ŁļĀźņØś Ē¢źņāüņØ┤ Ļ░ÉĻ░üņĀĆĒĢśņÖĆ ļģĖĒÖöņÖĆ Ļ┤ĆļĀ©ļÉ£ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśļź╝ ņÖäĒÖöņŗ£Ēé¼ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż[21].
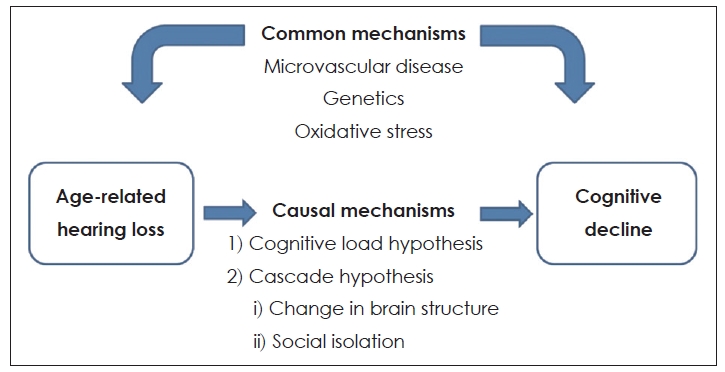
ļģĖĒÖöņä▒ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņØś Ļ┤ĆļĀ©ņä▒ņØä ņäżļ¬ģ Ļ░ĆļŖźĒĢ£ ĻĖ░ņĀäņØ┤ ņĢäņ¦ü ļ¬ģĒÖĢĒĢśĻ▓ī ļ░ØĒśĆņ¦Ćņ¦Ć ņĢŖņĢśņ¦Ćļ¦ī, ļģĖĒÖöņä▒ ļé£ņ▓ŁņØ┤ ņ╣śļ¦żņŚÉ ĻĖ░ņŚ¼ĒĢĀ ņłś ņ׳ņØīņØä ņäżļ¬ģĒĢśļŖö ņ×Āņ×¼ņĀüņØĖ ņøÉņØĖ Ļ░ĆņäżļōżņØ┤ ņ׳ļŗż (Fig. 1). Ēü¼Ļ▓ī 2Ļ░Ćņ¦Ć Ļ░ĆņäżņØ┤ ņ׳ļŖöļŹ░, causal mechanismĻ│╝ common mechanismņØ┤ļŗż. ĻĘĖ ņżæ causal mechanismņØä ņäżļ¬ģĒĢśļŖö 2Ļ░Ćņ¦Ć Ļ░ĆņäżņØ┤ ņ׳ļŗż.
ņ▓½ņ¦Ė, ņØ┤ ļæśņØś Ļ┤ĆĻ│äĻ░Ć ņØĖĻ│╝Ļ┤ĆĻ│ä(causal mechanism)ļØ╝ļŖö Ļ░ĆņäżļĪ£, cognitive load hypothesisņÖĆ cascade hypothesis ļō▒ņØ┤ ņ׳ļŗż. Cognitive load hypothesisļ×Ć, ļé£ņ▓Łņ£╝ļĪ£ ņØĖĒĢśņŚ¼ ņ▓ŁĻ░ü ņØĖņ¦Ć Ļ│╝ņĀĢņØä ņ£äĒĢ┤ ļŹö ļ¦ÄņØĆ ņØĖņ¦Ć ņ×ÉņøÉņØä ĒĢäņÜöļĪ£ ĒĢśĻ│Ā, ļŗżļźĖ ņØĖņ¦Ć Ļ│╝ņĀĢņŚÉ ņé¼ņÜ®ļÉśļŖö ņ×ÉņøÉņØä ņ▓ŁņĘ©ļģĖļĀź ņ¬Įņ£╝ļĪ£ ņĀäĒÖśĒĢśĻ▓ī ļÉśņ¢┤, Ļ▓░ĻĄŁ ņØĖņ¦ĆņĀü ņśłļ╣äņ£©(cognitive reserve) Ļ░Éņåīļź╝ ņ£Āļ░£ĒĢ£ļŗżļŖö Ļ░ĆņäżņØ┤ļŗż[22-25]. ņ”ē, ņ▓ŁĻ░ü ņ¦ĆĻ░ü ņ▓śļ”¼ņŚÉ ņŤļŖö Ļ│╝ļÅäĒĢ£ ņØĖņ¦Ć ļČĆĒĢś(cognitive load)Ļ░Ć ļćīņØś ĻĄ¼ņĪ░ņĀü ļ│ĆĒÖöņÖĆ ļŗżļźĖ ņØĖņ¦Ć Ļ│╝ņĀĢņØś ņåÉņāüĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņŗĀĻ▓ĮņØś Ēć┤Ē¢ēņØä ņ£Āļ░£ĒĢśļ®░, ņØĖņ¦ĆĻĖ░ļŖźņØś ņĀĆĒĢśļź╝ ņØ╝ņ£╝ĒéżĻ▓ī ļÉ£ļŗż[26]. Cascade hypothesisņŚÉņä£ļŖö, ļģĖĒÖöņä▒ ļé£ņ▓ŁņØ┤ ļćī ĻĄ¼ņĪ░ņŚÉ ļ│ĆĒÖöļź╝ ņØ╝ņ£╝ĒéżĻ│Ā ņ╣śļ¦ż ņ£äĒŚśņØä ņ”ØĻ░Ćņŗ£Ēé©ļŗżļŖö Ļ▓āņØ┤ļŗż. ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖļōżņØś MRIņŚÉņä£ ņØ╝ņ░© ņ▓ŁĻ░ü Ēö╝ņ¦łņØś ļČĆĒö╝ Ļ░Éņåīļź╝ ļ│┤ņśĆĻ│Ā[27,28], ņØ┤ļ¤░ ļćīļČĆĒö╝ņØś Ļ░ÉņåīļŖö ņ×Āņ×¼ņĀüņ£╝ļĪ£ ņ╣śļ¦ż ņ£äĒŚś ņ”ØĻ░Ćļź╝ ņ£Āļ░£ĒĢĀ ņłś ņ׳ļŖö ņØĖņ¦Ć Ļ│╝ņĀĢņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłśņ׳ļŗżļŖö Ļ▓āņØ┤ļŗż. Cascade hypothesisļź╝ ņäżļ¬ģĒĢśļŖö ļśÉ ļŗżļźĖ Ļ░ĆņäżņØĆ ņé¼ĒÜīņĀü Ļ│Āļ”ĮņØ┤ļŗż. ļģĖĒÖöņä▒ ļé£ņ▓Ł ĒÖśņ×ÉņŚÉņä£ņØś ņØśņé¼ņåīĒåĄņØś ņŗżĒī©ļŖö ņé¼ĒÜīņĀü ĒåĄĒĢ®ņØä ņŗ¼Ļ░üĒĢśĻ▓ī ņĀ£ĒĢ£ĒĢśļ®░, ņØ┤ļ¤░ ņé¼ĒÜīĒÖöņØś Ļ░ÉņåīļŖö ņé¼ĒÜīņĀü Ļ│Āļ”Į, Ļ│ĀļÅģĻ░ÉĻ│╝ ņÜ░ņÜĖņ”ØņØä ņØ╝ņ£╝ĒéżĻ▓ī ļÉ£ļŗż[29-34]. ņÜ░ņÜĖņ”ØĻ│╝ ņé¼ĒÜīņĀü Ļ│Āļ”ĮņØĆ ņ▓ŁĻ░üņןņĢĀņÖĆ ņØĖņ¦ĆņןņĢĀ ņé¼ņØ┤ļź╝ ļ¦żĻ░£ĒĢśļŖö ņŚŁĒĢĀņØä ĒĢśļ®░ ņ▓ŁĻ░üņןņĢĀņÖĆ Ļ┤ĆļĀ©ļÉ£ ņØ┤ļ¤¼ĒĢ£ ļ¼ĖņĀ£ļŖö ņ¦üĻ░äņĀæņĀüņ£╝ļĪ£ ņØĖņ¦ĆņןņĢĀļź╝ ņ£Āļ░£ĒĢśĻ▓ī ļÉ£ļŗż.
ļæśņ¦Ė, common mechanism Ļ░ĆņäżņØĆ ļģĖĒÖöņä▒ ļé£ņ▓Ł ĻĘĖ ņ×Éņ▓┤Ļ░Ć ņ╣śļ¦żļź╝ ņØ╝ņ£╝ĒéżļŖö Ļ▓āņØ┤ ņĢäļŗłļØ╝, ņ╣śļ¦żņÖĆ ļģĖĒÖöņä▒ ļé£ņ▓ŁņŚÉ ĻĖ░ņŚ¼ĒĢśļŖö Ļ│ĄĒåĄ ĻĖ░ņĀäņØ┤ ņ׳ļŗżļŖö Ļ▓āņØ┤ļŗż. ņ”ē, ļģĖĒÖöņä▒ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ņøÉņØĖ Ļ┤ĆĻ│äĻ░Ć ņĢäļŗłļØ╝ Ļ│ĄĒåĄņØś ņøÉņØĖņŚÉ ņØśĒĢ┤ ļ░£ņāØĒĢśĻ│Ā ņä£ļĪ£ ļÅģļ”ĮņĀüņ£╝ļĪ£ ļ░£ņāØĒĢśļ®░[26], ļćīņØś ļģĖĒÖöĻ│╝ņĀĢņŚÉņä£ Ļ│ĄĒåĄņĀüņØĖ ņŗĀĻ▓Į Ēć┤ĒÖö Ļ│╝ņĀĢņØś Ļ▓░Ļ│╝ļØ╝Ļ│Ā ĒĢĀ ņłś ņ׳ļŗżļŖö Ļ▓āņØ┤ļŗż[22]. ņØ┤ņÖĖņŚÉļÅä ļģĖĒÖöņä▒ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś ņé¼ņØ┤ņØś ņŚ░Ļ┤Ćņä▒ņØä ņäżļ¬ģĒĢśĻĖ░ ņ£äĒĢ┤ ņĄ£ĻĘ╝ ļģĖņćĀ(frailty)ņÖĆ Ļ┤ĆļĀ©ļÉ£ Ļ░ĆņäżļÅä ņĀ£ĻĖ░ļÉśĻ│Ā ņ׳ņ¦Ćļ¦ī[35,36], ņØ┤ ļæś Ļ░äņØś ņĀĢĒÖĢĒĢ£ ņØĖĻ│╝Ļ┤ĆĻ│äņØś ĒÖĢļ”ĮņØä ņ£äĒĢ┤ ļ¦ÄņØĆ ĒøäņåŹ ņŚ░ĻĄ¼ļōżņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż.
ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ Ēøä Ļ▓░Ļ│╝
ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØ┤ Ļ│Āņŗ¼ļÅä ļé£ņ▓ŁņØś Ēæ£ņżĆņĀüņØĖ ņ╣śļŻīļ▓Ģņ£╝ļĪ£ ņØĖņĀĢļÉśļ®┤ņä£, ņłśņłĀ Ļ▒┤ņłśĻ░Ć ņ”ØĻ░ĆĒĢśĻ│Ā ņłśņłĀ ņĀüņØæņ”ØņØś ļ▓öņ£äļÅä ĒÖĢļīĆļÉśĻ│Ā ņ׳ļŗż[37]. ļśÉĒĢ£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä ĒÜŹĻĖ░ņĀüņ£╝ļĪ£ Ļ░£ņäĀļÉ£ ņ▓ŁļĀźņ×¼ĒÖ£ņØś Ļ▓░Ļ│╝ņŚÉ ļīĆĒĢ£ ļ│┤Ļ│ĀĻ░Ć ļ¦ÄņĢśņ£╝ļéś, ņØ┤ļŖö ņŻ╝ļĪ£ ņåīņĢäļéś ņä▒ņØĖ ĒÖśņ×ÉņŚÉ ĻĄŁĒĢ£ļÉśņŚłļŗż. ĻĘĖļ¤¼ļéś, ņĄ£ĻĘ╝ ļģĖļĀ╣ ņØĖĻĄ¼ņØś ņ”ØĻ░ĆņŚÉ ļö░ļØ╝, ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ņØś ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØ┤ ņ”ØĻ░ĆĒĢ©ņŚÉ ļö░ļØ╝ ņØ┤ņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ Ļ▓░Ļ│╝Ļ░Ć ļ¦ÄņØ┤ ļ│┤Ļ│ĀļÉśĻ│Ā ņ׳ļŗż. ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņŗ£Ē¢ē Ēøä ņĀŖņØĆ ļéśņØ┤ņØś ļīĆņĪ░ĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ņłĀĒøä ņ¢Ėņ¢┤ņłśĒ¢ēļĀźņŚÉ ņ░©ņØ┤Ļ░Ć ņŚåņØīņØ┤ ļ│┤Ļ│ĀļÉśņŚłĻ│Ā[38,39], ņéČņØś ņ¦łņĀüņØĖ ņĖĪļ®┤ņŚÉņä£ļÅä ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņÖĆņÜ░ņØ┤ņŗØņłĀ Ēøä Ē¢źņāüļÉ£ Ļ▓░Ļ│╝Ļ░Ć ļ│┤Ļ│ĀļÉśņŚłļŗż[40]. ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ Ēøä ņ¢Ėņ¢┤ņłśĒ¢ēļĀź Ļ▓░Ļ│╝ļź╝ ļ│┤Ļ│ĀĒĢ£ ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņØ┤ ņ׳ļŗż. Vermeire ļō▒[40]ņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä 2ļģäĻ░ä 89ļ¬ģņØś ņ¢Ėņ¢┤ņŖĄļōØ Ēøä ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ņä▒ņØĖ ĒÖśņ×ÉļōżņØä ļČäņäØĒĢśņśĆĻ│Ā, ņØ┤ņŗØ ņŗ£ņØś ņŚ░ļĀ╣ņØĆ ĒÅēĻĘĀ 58ņäĖ(17-83ņäĖ)ņśĆņ£╝ļ®░, ļé£ņ▓ŁņØś ĻĖ░Ļ░äņØ┤ļéś ļ│┤ņ▓ŁĻĖ░ ņé¼ņÜ® ņ£Āļ¼┤ņŚÉ ļīĆĒĢ£ ņ¢ĖĻĖēņØĆ ņŚåņŚłļŗż. ņØ┤ ņżæ 25ļ¬ģņØĆ 70ņäĖ ņØ┤ņāüņØś ĒÖśņ×ÉļōżņØ┤ņŚłĻ│Ā, 70ņäĖ ņØ┤ĒĢś ĒÖśņ×ÉĻĄ░Ļ│╝ņØś ļ╣äĻĄÉ ņŚÉņä£ ņ¢Ėņ¢┤ņłśĒ¢ēļĀźņŚÉ ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż. Budenz ļō▒[41]ņØĆ ņ¢Ėņ¢┤ņŖĄļōØ Ēøä ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ņä▒ņØĖ ĒÖśņ×ÉļōżņŚÉņä£ 70ņäĖ ņØ┤ņāüņØś ĒÖśņ×É 60ļ¬ģĻ│╝ 18-69ņäĖ ņé¼ņØ┤ņØś ĒÖśņ×É 48ļ¬ģņØś ņ¢Ėņ¢┤ņłśĒ¢ēļĀźņØä 2ļģäĻ░ä Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ ĒĢśņśĆļŗż. ļģĖņØĖ ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņØ┤ņŗØ ņŗ£ ĒÅēĻĘĀņŚ░ļĀ╣ņØĆ 76┬▒4.0ņäĖ(70-86ņäĖ)ņśĆĻ│Ā, ņĀŖņØĆ ĒÖśņ×ÉĻĄ░ņŚÉņä£ ĒÅēĻĘĀņŚ░ļĀ╣ņØĆ 47.9┬▒10.8ņäĖ(22-62ņäĖ)ņśĆņ£╝ļ®░, ļé£ņ▓Ł ĻĖ░Ļ░äņØĆ ĒÅēĻĘĀ 34.0┬▒21.4ļģäĻ│╝ 23.4┬▒17.9ļģäņ£╝ļĪ£ ļæÉ ĻĄ░ Ļ░äņØś ņ£ĀņØśĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņśĆļŗż(p=0.01). ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ Ēøä ņ¢Ėņ¢┤ņłśĒ¢ēļĀźņŚÉņä£ ļģĖņØĖ ĒÖśņ×ÉĻĄ░ņŚÉņä£ ņ£ĀņØśļ»ĖĒĢ£ Ē¢źņāüņØä ļ│┤ņśĆļŗż. ļæÉ ĻĄ░ ļ¬©ļæÉ ņ▓½ 3Ļ░£ņøöņŚÉ ņ¢Ėņ¢┤ļČäļ│äļĀź(speech discrimination)ņØś ļ╣ĀļźĖ Ē¢źņāüņØä ļ│┤ņśĆĻ│Ā, ņ¢Ėņ¢┤ņłśĒ¢ēļĀźņŚÉņä£ļÅä ļ╣äņŖĘĒĢ£ ņä▒ņן ņåŹļÅäļź╝ ļ│┤ņśĆļŗż. ļ╣äļĪØ ļģĖņØĖ ĒÖśņ×ÉĻĄ░ņØś ņ¢Ėņ¢┤ņłśĒ¢ēļĀźņØ┤ ĒÅēĻĘĀņĀüņ£╝ļĪ£ ņĀŖņØĆ ĒÖśņ×ÉĻĄ░ņŚÉ ļ╣äĒĢ┤ ļé«ņĢśņ¦Ćļ¦ī, ņØ┤ļŖö ņŚ░ļĀ╣ņØś ņ░©ņØ┤ņŚÉ ņØśĒĢ£ Ļ▓āņØ┤ ņĢäļŗłļØ╝ ļæÉ ĻĄ░ Ļ░äņØś ļé£ņ▓Ł ĻĖ░Ļ░äņØś ņ░©ņØ┤ņŚÉ ņØśĒĢ£ Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. Lenarz ļō▒[42]ņØĆ 1005ļ¬ģņØś ņ¢Ėņ¢┤ņŖĄļōØĻĖ░ Ēøä ļé£ņ▓Ł ĒÖśņ×É ņżæņŚÉņä£ 70ņäĖ ņØ┤ņāüņØś ĒÖśņ×É 130ļ¬ģ(Group 4)Ļ│╝ 18-69ņäĖņé¼ņØ┤ņØś ĒÖśņ×É 875ļ¬ģņØä 2ļģäĻ░ä ļ╣äĻĄÉ ļČäņäØĒĢśņśĆĻ│Ā, ņĀŖņØĆ ĒÖśņ×ÉļōżņØĆ ļéśņØ┤ņŚÉ ļö░ļØ╝, Group 1 (18-39ņäĖ, n=220), Group 2 (40-59ņäĖ, n=420), Group 3 (60-69ņäĖ, n=235)ļĪ£ ļČäļźśĒĢśņśĆļŗż. ļģĖņØĖ ĒÖśņ×ÉĻĄ░ņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä ņĀŖņØĆ ĒÖśņ×ÉĻĄ░Ļ│╝ ņ£Āņé¼ĒĢ£ ĒĢÖņŖĄĻ│ĪņäĀ (learning curve)ņØä ļ│┤ņśĆĻ│Ā, ņĪ░ņÜ®ĒĢ£ ĒÖśĻ▓ĮņŚÉņä£ ņ¢Ėņ¢┤ ĒÅēĻ░ĆņŚÉņä£ļÅä ņĀŖņØĆ ĒÖśņ×ÉĻĄ░Ļ│╝ ļ╣äņŖĘĒĢ£ ņłśĒ¢ēļĀźņØä ļ│┤ņśĆļŗż. ņ¢Ėņ¢┤ ņłśĒ¢ēļĀźņØĆ 6Ļ░£ņøö ņ¦Ė ņĢłņĀĢņĀüņØĖ ņłśņżĆņŚÉ ļÅäļŗ¼ĒĢśņśĆņ£╝ļ®░, 2ļģäĻ░ä ņłśĒ¢ēļĀźņØś Ļ░ÉņåīļŖö Ļ┤Ćņ░░ļÉśņ¦Ć ņĢŖņĢśļŗż. ĒŖ╣Ē׳ ņØ┤ ņŚ░ĻĄ¼ņŚÉņä£ļŖö ņŚ░ļĀ╣ ņØ┤ņÖĖņŚÉ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ Ļ▓░Ļ│╝ņŚÉ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ļŖö ņ×Āņ×¼ņĀüņØĖ ĻĄÉļ×Ć ņÜöņåīļĪ£ ņāØĻ░üļÉśļŖö ļé£ņ▓Ł ĻĖ░Ļ░ä, ņłśņłĀ ņĀä ņ▓ŁļĀź ņłśņżĆ, ņ×äĒöīļ×ĆĒŖĖ ņŗ£ņŖżĒģ£ņØś ņ£ĀĒśĢ ļō▒ņØä Ļ░ÖņØ┤ ĒÅēĻ░ĆĒĢśņśĆĻ│Ā, ļģĖņØĖ ĒÖśņ×ÉĻĄ░Ļ│╝ ņĀŖņØĆ ĒÖśņ×ÉĻĄ░ ņé¼ņØ┤ņŚÉņØ┤ ņäĖ Ļ░Ćņ¦Ć ņÜöņØĖņŚÉ ļīĆĒĢ┤ ņ£ĀņØśļ»ĖĒĢ£ ņ░©ņØ┤Ļ░Ć ņŚåņŚłļŗż. ņ”ē ņ¢Ėņ¢┤ņŖĄļōØĻĖ░ Ēøä ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä ņØīņä▒ ņØĖņŗØ(speech perception)ņØĆ ĒÖśņ×ÉņØś ņŚ░ļĀ╣Ļ│╝ ņāüĻ┤ĆņŚåņØ┤ Ēü¼Ļ▓ī Ē¢źņāüļÉśņŚłĻ│Ā[43], ņØ┤Ļ▓āņØĆ ņØ┤ņŗØ ņŗ£ ņŚ░ļĀ╣ļ¦īņØä ņłĀĒøä ņ▓ŁļĀź Ļ▓░Ļ│╝ņØś ņśłņĖĪ ņØĖņ×ÉļĪ£ Ļ│ĀļĀżĒĢĀ Ļ▓āņØ┤ ņĢäļŗłļØ╝, ļé£ņ▓Ł ĻĖ░Ļ░äĻ│╝ Ļ░ÖņØĆ ļ│┤ļŗż ļ¬ģĒÖĢĒĢ£ ņśłņĖĪņØĖņ×ÉĻ░Ć Ļ│ĀļĀżļÉśņ¢┤ņĢ╝ ĒĢ©ņØä ņØśļ»ĖĒĢ£ļŗż. ļśÉĒĢ£, ņĄ£ĻĘ╝ņØś ņŚ░ĻĄ¼ļōżņŚÉ ņä£ļÅä ņ¢Ėņ¢┤ņŖĄļōØĻĖ░ Ēøä ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ Ēøä ņ▓ŁĻ░üĒĢÖņĀü Ļ▓░Ļ│╝ļŖö ņØ┤ņŗØ ņŚ░ļĀ╣Ļ│╝ ņ£ĀņØśļ»ĖĒĢ£ ņāüĻ┤ĆĻ┤ĆĻ│äĻ░Ć ņŚåņØīņØä ļ│┤Ļ│ĀĒĢśĻ│Ā ņ׳ļŗż[44-46]. ļö░ļØ╝ņä£, ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØĆ Ļ│Āņŗ¼ļÅäņØś ļé£ņ▓ŁņØä Ļ░Ćņ¦ä Ļ│ĀļĀ╣ņØś ĒÖśņ×ÉņŚÉĻ▓ī ņ▓ŁĻ░üĒĢÖņĀü ņłśĒ¢ēļĀź, Ļ▒┤Ļ░Ģ ņāüĒā£, ņé¼ĒÜīņĀü ņāüĒśĖņ×æņÜ®ņŚÉ ņ׳ņ¢┤ ĒśäņĀĆĒĢ£ Ļ░£ņäĀņØś Ļ▓░Ļ│╝ļź╝ ņżä ņłś ņ׳ļŖö ņĢłņĀäĒĢśĻ│Ā ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻīļ▓Ģņ×äņØä ņŗ£ņé¼ĒĢ£ļŗż[43].
ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØ┤ ņØĖņ¦ĆĻĖ░ļŖźņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢ź
ņ╣śļ¦żļź╝ ņ╣śļŻīĒĢśļŖö ļŹ░ ņ׳ņ¢┤ ĒÜ©Ļ│╝ņĀüņØĖ ņ╣śļŻīĻ░Ć ņĢäņ¦ü ņŚåĻĖ░ ļĢīļ¼ĖņŚÉ, ņØĖņ¦Ć ĻĖ░ļŖź ņĀĆĒĢśņŚÉ ļīĆĒĢ£ ņłśņĀĢ Ļ░ĆļŖźĒĢ£ ņ£äĒŚś ņÜöņåīļź╝ Ļ┤Ćļ”¼ĒĢśļŖö Ļ▓āņØ┤ Ļ░£ņØĖĻ│╝ ņé¼ĒÜīņŚÉ ņ¦ĆļīĆĒĢ£ ņśüĒ¢źņØä ļ»Ėņ╣Ā ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż. ļö░ļØ╝ņä£ ļé£ņ▓ŁņØ┤ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśņØś ņØ╝ņ░©ņĀüņØĖ Ļ░£ņäĀ Ļ░ĆļŖźĒĢ£ ņ£äĒŚś ņÜöņåīĻ░Ć ļÉśĻĖ░ ļĢīļ¼ĖņŚÉ, ļ│┤ņ▓ŁĻĖ░ļéś ņØĖĻ│ĄņÖĆņÜ░ Ļ░ÖņØĆ ņ▓ŁĻ░üņĀü ņżæņ×¼Ļ░Ć ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś ļ░Å ņ╣śļ¦żņÖĆ Ļ┤ĆļĀ©ļÉ£ Ļ▓░Ļ│╝ļź╝ ņāüļŗ╣Ē׳ Ļ░£ņäĀņŗ£Ēé¼ Ļ▓āņØ┤ļØ╝ ņśłņāüļÉ£ļŗż. ņØ┤ļŖö ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØ┤ ņØĖņ¦ĆĻĖ░ļŖź Ē¢źņāüņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņŚÉ ļīĆĒĢ┤ ņé┤ĒÄ┤ļ│Ė ļ¬ćļ¬ć ņŚ░ĻĄ¼ņŚÉņä£ ĒÖĢņØĖĒĢĀ ņłś ņ׳ļŗż.
Ēöäļ×æņŖżņŚÉņä£ 10Ļ░£ņØś 3ņ░© ņØśļŻīĻĖ░Ļ┤ĆņŚÉņä£ ņłśĒ¢ēĒĢ£ ņĀäĒ¢źņĀü ņŚ░ĻĄ¼ņŚÉņä£ 65-85ņäĖņØś ĒÖśņ×É 94ļ¬ģņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ ņĀä, ņłśņłĀ Ēøä 6Ļ░£ņøö, 12Ļ░£ņøö Ēøä ņØĖņ¦ĆĻĖ░ļŖźņØä ĒÅēĻ░ĆĒĢśņśĆļŗż[47]. ņłśņłĀ ņĀä ļé«ņØĆ ņØĖņ¦ĆĻĖ░ļŖź ņĀÉņłśļź╝ ļ░øņØĆ ĒÖśņ×ÉļōżņØś 80% ņØ┤ņāüņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ Ēøä 12Ļ░£ņøöņ¦Ė ņØĖņ¦ĆĻĖ░ļŖźņØś Ē¢źņāüņØä ļ│┤ņśĆĻ│Ā, ņØĖĻ│ĄņÖĆņÜ░ļź╝ ĒåĄĒĢ£ ņ▓ŁĻ░üņĀü ņ×¼ĒÖ£ņØ┤ ļģĖņØĖļōżņŚÉĻ▓ī ņåÉņāüļÉ£ ņØĖņ¦ĆĻĖ░ļŖźņØś Ļ░£ņäĀĻ│╝ Ļ┤ĆļĀ©ņØ┤ ņ׳ļŗżļŖö Ļ▓░ļĪĀņØä ļé┤ņŚłļŗż. ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ Ēøä ņØĖņ¦ĆĻĖ░ļŖźņØś Ļ▓░Ļ│╝ļź╝ ļ│┤ņŚ¼ņŻ╝ļŖö ņ▓┤Ļ│äņĀü ļ”¼ļĘ░ņŚÉ Ļ┤ĆĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£ļŖö, 166ļ¬ģņØś ĒÖśņ×ÉĻ░Ć ĒżĒĢ©ļÉ£ ņäĀĒāØļÉ£ 6Ļ░£ņØś ņŚ░ĻĄ¼ ņżæ 5Ļ░£ņŚÉņä£ ņØĖĻ│Ą ņÖĆņÜ░ ņłśņłĀ Ēøä ņØĖņ¦ĆĻĖ░ļŖźņØś Ē¢źņāüņØä ļ│┤Ļ│ĀĒĢśņśĆĻ│Ā[47-51], ņśżņ¦ü ĒĢ£ Ļ░£ņØś ņŚ░ĻĄ¼ņŚÉņä£ļ¦ī ņłśņłĀ ņØ┤Ēøä ņØĖņ¦Ć ņłśĒ¢ēļĀźņŚÉ ņ£ĀņØśĒĢ£ ļ│ĆĒÖöĻ░Ć ļ│┤ņØ┤ņ¦Ć ņĢŖņĢśļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[52]. Table 2ņŚÉņä£ ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀņØ┤ ņØĖņ¦ĆĻĖ░ļŖźņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņŚÉ ļīĆĒĢ£ 6Ļ░£ņØś ņŚ░ĻĄ¼ļōżņØä ņĀĢļ”¼ĒĢśņśĆļŗż.
Ohta ļō▒[53]ņØĆ 21ļ¬ģņØś 65ņäĖ ņØ┤ņāü ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņłśņłĀ ņĀä, ņłśņłĀ Ēøä 1ļģä, 2ļģäĻ╣īņ¦Ć Mini-Mental State Examination (MMSE)ņ£╝ļĪ£ ņØĖņ¦ĆĻĖ░ļŖźņØä ĒÅēĻ░ĆĒĢśņśĆņØä ļĢī, ņØīņä▒ ņāØņä▒ (speech production)ņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä ņØĖņ¦ĆĻĖ░ļŖź Ē¢źņāüņØä ņ£äĒĢ┤ ņżæņÜöĒĢśļ®░, ņØĖņ¦ĆĻĖ░ļŖźņØś Ē¢źņāüņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä 1ļģäņ¦Ė ņĄ£Ļ│ĀņĀÉņŚÉ ņØ┤ļź┤Ļ▓ī ļÉ©ņØä ļ│┤Ļ│ĀĒĢśņśĆļŗż. ļ╣äļĪØ ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ Ļ│Āņŗ¼ļÅäņØś ļé£ņ▓ŁņØ┤ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśļź╝ ņĢģĒÖöņŗ£Ēéżņ¦Ćļ¦ī, ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀņØĆ MMSE ņĀÉņłśĻ░Ć ņĄ£Ļ│ĀņĀÉņØĖ 1ļģä Ēøä(ņ”ē, ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä 2ļģäņ¦Ė) Ļ░ÉņåīĒĢśļŹöļØ╝ļÅä ņØĖņ¦Ć ĻĖ░ļŖźņŚÉ ĻĖŹņĀĢņĀüņØĖ ņśüĒ¢źņØä ļ»Ėņ╣£ļŗżĻ│Ā ļ│┤Ļ│ĀĒĢśņśĆļŗż[53]. ļśÉĒĢ£, ņ▓ŁĻ░üņŚÉ ĻĖ░ļ░śĒĢśņŚ¼ ļŗżļźĖ ņé¼ļ×īļōżĻ│╝ ļīĆĒÖöĒĢśļŖö Ļ▓āņØĆ ņØĖņ¦ĆĻĖ░ļŖźņØä Ē¢źņāüņŗ£ĒéżĻĖ░ ņ£äĒĢ┤ ļ¦żņÜ░ ņżæņÜöĒĢśļ®░, ļŗ©ņł£Ē׳ ņ▓ŁĻ░ü ņłśņżĆĻ│╝ ņØīņä▒ ņØĖņŗØ(speech recognition)ņØ┤ Ē¢źņāüļÉśļŖö Ļ▓āļ¦īņ£╝ļĪ£ļŖö ļČĆņĪ▒ĒĢ©ņØä ņŗ£ņé¼ĒĢśņśĆļŗż. ļö░ļØ╝ņä£, Ļ│ĀļĀ╣ņØś ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ĒÖśņ×ÉņŚÉņä£ ņ▓ŁĻ░üļ│┤ņāüņØä ĻĖ░ļ░śņ£╝ļĪ£ ĒĢ£ ļīĆĒÖöļŖźļĀź Ē¢źņāüņØä ļ¬®Ēæ£ļĪ£ ĒĢ£ ņ×¼ĒÖ£ņØ┤ ņ╣śļ¦ż ņśłļ░®ņØś ĒĢĄņŗ¼ ņĀäļץņØ┤ ļÉĀ Ļ▓āņØ┤ļŗż[53].
65ņäĖ ņØ┤ņāüņØś Ļ│ĀļĀ╣ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ĒÖśņ×É 70ļ¬ģņŚÉ ļīĆĒĢ£ ņŚ░ĻĄ¼ņŚÉņä£, Ļ▓ĮļÅäņØĖņ¦ĆņןņĢĀ(mild cognitive impairment) ĒÖĢļźĀņØĆ 45%ļĪ£[44], Ļ░ÖņØĆ ļéśņØ┤ņØś ņØ╝ļ░śņØĖņØ┤ 3%-19%ņØĖ Ļ▓āņŚÉ ļ╣äĒĢ┤ ļåÆņĢśĻ│Ā[54], ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ Ēøä ņ▓ŁĻ░üņ×¼ĒÖ£ņØ┤ ņØśņé¼ņåīĒåĄ, ņéČņØś ņ¦ł, ņØĖņ¦ĆĻĖ░ļŖź Ē¢źņāüņŚÉ ĻĖŹņĀĢņĀü ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ ņ╣śļ¦żļĪ£ņØś ņØ┤Ē¢ēņØ┤ ņżäņ¢┤ļō”ņØä ļ│┤ņŚ¼ņŻ╝ņŚłļŗż. ņØ┤ļŖö ļé£ņ▓ŁņŚÉ ņØśĒĢ£ Ļ▓ĮļÅäņØĖņ¦ĆņןņĢĀļŖö ņØĖņ¦ĆĻĖ░ļŖźņŚÉ ņ׳ņ¢┤ ņ▓ŁĻ░üņ×¼ĒÖ£ņŚÉ ņØśĒĢ┤ ĻĖŹņĀüņĀü ĒÜ©Ļ│╝ļź╝ Ļ░¢ļŖö ņĢäĒśĢ(subtype)ņØ╝ Ļ▓āņØ┤ļØ╝ļŖö Ļ░ĆņĀĢņØä ĒĢĀ ņłś ņ׳ļŗż[44]. ļö░ļØ╝ņä£, ĒŖ╣Ē׳ Ļ▓ĮļÅäņØĖņ¦ĆņןņĢĀļź╝ Ļ░Ćņ¦ĆļŖö Ļ│Āņŗ¼ļÅäņØś ļé£ņ▓Ł ĒÖśņ×ÉņŚÉņä£ ņ¦Ćņ▓┤ ņŚåņØ┤ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØä ņĀ£ņĢłĒĢśļŖö ņżæņÜöņä▒ņØä Ļ░ĢņĪ░ĒĢśĻ│Ā ņ׳ļŗż[44]. ļö░ļØ╝ņä£, ņŗ¼ļÅäņØś ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ Ļ▓ĮļÅäņØĖņ¦ĆņןņĢĀņÖĆ Ļ░ÖņØĆ cognitive syndromeņØä ĒŖ╣ņĀĢ ņ¦ĆņØä ņłś ņ׳ļŖö ļ░öņØ┤ņśżļ¦łņ╗żļéś ņŗĀĻ▓ĮĒĢÖņĀü ņśüņāüĻ▓Ćņé¼(neuroimaging) Ļ░ÖņØĆ ņČöĻ░ĆņĀü Ļ▓Ćņé¼Ļ░Ć ĒĢäņÜöĒĢĀ Ļ▓āņØ┤Ļ│Ā ĒŖ╣Ē׳, Ļ▓ĮļÅäņØĖņ¦Ć ņןņĢĀņÖĆ Ļ░ÖņØĆ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśĻ░Ć ņ׳ļŖö ĒÖśņ×ÉņØś Ļ▓ĮņÜ░ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀņØä ĒåĄĒĢ┤ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśļź╝ ņŚŁņĀäņŗ£ņ╝£ ņ╣śļ¦żļĪ£ņØś ņØ┤ĒÖśņØä ņśłļ░®ĒĢĀ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż[44].
ņ£äņÖĆ Ļ░ÖņØĆ ļ¦ÄņØĆ ņŚ░ĻĄ¼ļōżņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä ņØĖņ¦ĆĻĖ░ļŖźņØ┤ Ē¢źņāüļÉ©ņŚÉ ļīĆĒĢ£ ļ¬ģļ░▒ĒĢ£ Ļ▓░Ļ│╝ļź╝ ņ¢╗ņŚłļŗż. ĻĘĖļ¤¼ļéś ņŚ¼ņĀäĒ׳ ļé©ļŖö ņØśļ¼ĖņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤ĒøäņØś ņØĖņ¦ĆņĀü Ļ░£ņäĀņØ┤ ņ▓ŁĻ░üĻ│╝ Ļ┤ĆļĀ©ļÉ£ ņØĖņ¦ĆņĀü ņĀĆĒĢśļź╝ ņÖäņĀäĒ׳ ņŚŁņĀäņŗ£Ēé¼ ņłś ņ׳ņØä ļ¦īĒü╝ ņČ®ļČäĒ׳ Ēü░ ņ¦Ć ņŚ¼ļČĆņŚÉ ļīĆĒĢ£ ĒĢĄņŗ¼ ņØśļ¼Ėņ£╝ļĪ£ ļé©ņĢä ņ׳ļŗż. ņØ┤ļ¤░ ņØśļ¼ĖņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä ļé£ņ▓Ł ĒÖśņ×ÉļōżņØä ņŚ░ļĀ╣ņØ┤ ļ¦żņ╣śļÉ£ ņĀĢņāü ņ▓ŁļĀźņØś ļīĆņĪ░ĻĄ░Ļ│╝ņØś ļ╣äĻĄÉļź╝ ĒåĄĒĢ┤ ĒĢ┤Ļ▓░ĒĢĀ ņłś ņ׳ļŗż[55]. ļśÉĒĢ£, ņØĖņ¦ĆĻĖ░ļŖź Ļ▓Ćņé¼ ņżæ ņØ╝ļČĆ ĒĢŁļ¬®ļōżņØĆ ņ¦Ćņŗ£ļ¼ĖņØ┤ļéś ņłśĒ¢ēĻ│╝ņĀĢņØ┤ ņ▓ŁĻ░üņĀü Ēæ£Ēśäņ£╝ļĪ£ ļÉśņ¢┤ņ׳Ļ▒░ļéś, Ļ▓Ćņé¼ ņłśĒ¢ēĻ│╝ņĀĢņŚÉņä£ ĻĄ¼ņ¢┤ļź╝ ļ░śļ│ĄĒĢśļŖö ļō▒ ņ▓ŁĻ░üņŚÉ ņØśņĪ┤ĒĢ┤ņĢ╝ ĒĢśļŖö ņ¢Ėņ¢┤ Ļ│╝ņĀ£ņØ┤ĻĖ░ ļĢīļ¼ĖņŚÉ, ļé£ņ▓Łņ£╝ļĪ£ ņØĖĒĢ┤ Ļ▓Ćņé¼ ņłśĒ¢ēņØ┤ ņ¢┤ļĀżņøī ļé£ņ▓ŁņØĖņŚÉņä£ ņØĖņ¦ĆĻĖ░ļŖźņØ┤ ņĀĆĒÅēĻ░ĆļÉśļŖö Ļ▓ĮņÜ░ļōżņØ┤ ņ׳ļŗż. ņØ┤ļĀćĻ▓ī ņ▓ŁĻ░üņĀü Ēæ£ĒśäņŚÉ ņØśņĪ┤ĒĢśļŖö ņØĖņ¦ĆĻĖ░ļŖź Ļ▓Ćņé¼ņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņØ┤Ēøä Ļ┤Ćņ░░ļÉ£ ļ│ĆĒÖöļŖö ļŗ©ņł£Ē׳ ņØĖņ¦ĆņØś Ē¢źņāüņŚÉ ņØśĒĢ£ļŗżĻĖ░ ļ│┤ļŗżļŖö ņ▓ŁļĀźĻ░£ņäĀņØś Ļ▓░Ļ│╝ņØ╝ ņłś ņ׳ļŗż[55]. ņ▓ŁļĀźĻ░£ņäĀņŚÉ ņØśĒĢ£ ņØĖņ¦ĆĻĖ░ļŖź Ē¢źņāü ĒÜ©Ļ│╝ļź╝ ļ░░ņĀ£ĒĢśĻĖ░ ņ£äĒĢ┤ņä£ļŖö ņ▓ŁļĀźņŚÉ ņØśņĪ┤ĒĢśņ¦Ć ņĢŖļŖö ņØĖņ¦ĆĻĖ░ļŖź Ļ▓Ćņé¼ļéś, ĻĖ░ņĪ┤ Ļ▓Ćņé¼ņØś ļ│ĆĒśĢņØ┤ ĒĢäņÜöĒĢĀ Ļ▓āņØ┤ļŗż.
2021ļģä Huber ļō▒[55]ņØĆ ļéśņØ┤, ņä▒ļ│ä, ĻĄÉņ£Ī ņĀĢļÅäļź╝ ļ¦żņ╣ŁĒĢ£ ņĀĢņāü ņ▓ŁļĀźĻĄ░Ļ│╝ņØś ļ╣äĻĄÉļź╝ ĒåĄĒĢ┤, ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ņĀäĻ│╝ ņłśņłĀ Ēøä 12Ļ░£ņøöņ¦Ė ņØĖņ¦ĆĻĖ░ļŖź ņłśĒ¢ēņØä ĒÅēĻ░ĆĒĢśņśĆļŗż. ņØ┤ ņŚ░ĻĄ¼ņŚÉņä£, ņĀĢņāü ņ▓ŁļĀźĻĄ░Ļ│╝ ļ╣äĻĄÉĒĢśņŚ¼ ĒÖĢņŚ░ĒĢ£ ņ░©ņØ┤ļź╝ ļ│┤ņØ┤ļŖö ņØ╝ļČĆņØś ĒŖ╣ņĀĢ ņØĖņ¦Ć ĻĖ░ņłĀļ¦īņØ┤ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ Ēøä ļ│┤ņāüļÉĀ ņłś ņ׳ņŚłļŗż. ņĀĢņāü ņ▓ŁļĀźĻĄ░Ļ│╝ ļÅÖļō▒ĒĢ£ Ļ▓░Ļ│╝ļŖö Ļ│äĒÜŹ(planning), ņĪ░ņĀĢ(coordination), ņŻ╝ņØśļĀź ņĪ░ņĀł(attentional control)ņØä ĒĢäņÜöļĪ£ ĒĢśļŖö ņØĖņ¦Ć Ļ│╝ņŚģņØ┤ņŚłļŗż. ņ¦ĆņŚ░ ĒÜīņāü(delayed recall), ņ¢Ėņ¢┤ņä▒ ĻĖ░ņ¢ĄĒÜīņāü(verbal retrieval), ņ¢ĄņĀ£(inhibition), ņØĖņ¦ĆņĀü ņ£ĀņŚ░ņä▒(cognitive flexibility)ņØä Ļ░ĢņĪ░ĒĢśļŖö ņØĖņ¦ĆņĀü Ļ│╝ņŚģņØś ņłśĒ¢ēņØĆ ņØĖĻ│ĄņÖĆņÜ░ ņØ┤ņŗØņłĀ ĒÖśņ×ÉņŚÉņä£ ļŹö ņŚ┤ļō▒ĒĢśņśĆļŗż[55]. ļśÉĒĢ£, ņØĖņ¦Ć ĻĖ░ļŖźņØś Ē¢źņāüņØĆ ņłśņłĀ Ēøä 12Ļ░£ņøöņØ┤ ņĢäļŗī 3Ļ░£ņøöņ¦Ė ņØīņä▒ ņØĖņŗØ(speech recognition) Ļ▓░Ļ│╝ņÖĆ Ļ┤ĆļĀ©ņØ┤ ņ׳ņŚłļŗż[55].
Ļ▓░ļĪĀ
ļģĖņØĖņŚÉņä£ ļé£ņ▓ŁĻ│╝ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśļŖö ļåÆņØĆ Ļ┤ĆļĀ©ņä▒ņØä Ļ░Ćņ¦äļŗż. ļśÉĒĢ£, ļģĖĒÖöņä▒ ļé£ņ▓ŁņØĆ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢś ļ░Å ņ╣śļ¦żņØś ņżæņÜöĒĢ£ ņ£äĒŚśņÜöņØĖņ£╝ļĪ£ ņ×æņÜ®ĒĢśĻĖ░ ļĢīļ¼ĖņŚÉ, ļ│┤ņ▓ŁĻĖ░ļéś ņØĖĻ│ĄņÖĆņÜ░ ļō▒ņØä ĒåĄĒĢ£ ņ▓ŁĻ░üņĀü ņ×¼ĒÖ£ņØ┤ ņ╣śļ¦żļź╝ ņśłļ░®ĒĢĀ ņłś ņ׳ļŖö ļīĆņĢłņØ┤ ļÉĀ ņłś ņ׳ļŗż. ĒŖ╣Ē׳ Ļ│Āņŗ¼ļÅä ņØ┤ņāüņØś ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØĆ ņ▓ŁĻ░üņĀü ņłśĒ¢ēļĀźņØä ļåÆņØ╝ ņłś ņ׳ļŖö ĒÜ©Ļ│╝ņĀüņØĖ ņ▓ŁĻ░üņ×¼ĒÖ£ ļ░®ļ▓ĢņØ┤ļŗż. ļģĖņØĖĒÖśņ×ÉņŚÉņä£ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀ Ēøä ņ▓ŁĻ░üņ×¼ĒÖ£ņØ┤ ņØĖņ¦ĆĻĖ░ļŖź Ē¢źņāüņŚÉ ĻĖŹņĀĢņĀü ĒÜ©Ļ│╝ļź╝ ļ│┤ņŚ¼ ņ╣śļ¦żļĪ£ņØś ņØ┤Ē¢ēņØ┤ ņżäņ¢┤ļōż Ļ▓āņ£╝ļĪ£ ņāØĻ░üļÉ£ļŗż. ĒŖ╣Ē׳, ņŗ¼Ļ│ĀļÅäņØś ļé£ņ▓ŁņØä Ļ░Ćņ¦ä ļģĖņØĖ ĒÖśņ×ÉņŚÉņä£ ļ░öņØ┤ņśżļ¦łņ╗żļéś ņŗĀĻ▓ĮĒĢÖņĀü ņśüņāüĻ▓Ćņé¼ ļō▒ņØä ĒåĄĒĢ£ Ļ▓ĮļÅäņØś ņØĖņ¦ĆĻĖ░ļŖź ņןņĢĀņÖĆ Ļ░ÖņØĆ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśļź╝ ņĪ░ĻĖ░ņŚÉ ļ░£Ļ▓¼ĒĢśņŚ¼, ņØĖĻ│ĄņÖĆņÜ░ Ļ░ÖņØĆ ņóĆ ļŹö ņĀüĻĘ╣ņĀüņØĖ ņłśņłĀņĀü ņ╣śļŻīļź╝ ĒåĄĒĢ┤ ņØĖņ¦ĆĻĖ░ļŖź ņĀĆĒĢśļź╝ ņŚŁņĀäņŗ£ņ╝£ ņ╣śļ¦żļĪ£ņØś ņØ┤Ē¢ēņØä Ļ░Éņåīņŗ£Ēé¼ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż. ņĢ×ņ£╝ļĪ£ ņóĆ ļŹö ņ▓ŁĻ░üņĀü ņśüĒ¢źļĀźņØä ļ░░ņĀ£ĒĢ£ ņØĖņ¦ĆĻĖ░ļŖź Ļ▓Ćņé¼ņÖĆ ņśżļ×£ Ļ▓ĮĻ│╝ Ļ┤Ćņ░░ ĻĖ░Ļ░äņØä Ļ░Ćņ¦ĆļŖö ņל ļööņ×ÉņØĖļÉ£ ņŚ░ĻĄ¼ļź╝ ĒåĄĒĢ┤ ņØĖĻ│ĄņÖĆņÜ░ ņłśņłĀņØ┤ ņØĖņ¦ĆĻĖ░ļŖźņŚÉ ļ»Ėņ╣śļŖö ņśüĒ¢źņØä ņóĆ ļŹö ņ▓┤Ļ│äņĀüņ£╝ļĪ£ ļČäņäØĒĢĀ ņłś ņ׳ņØä Ļ▓āņØ┤ļŗż.